


 Sign Out
Sign Out


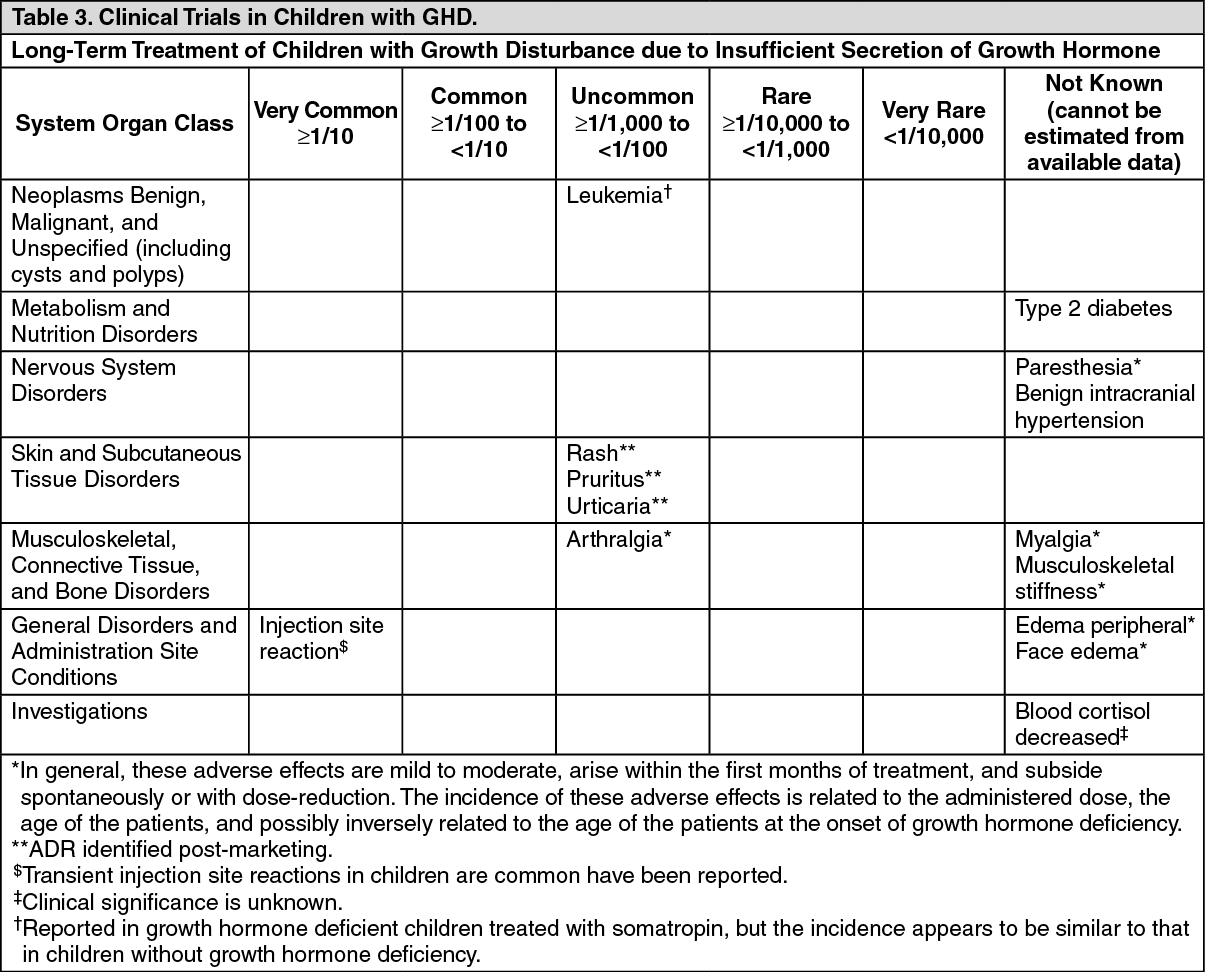
The incidence of these adverse effects is related to the administered dose, the age of the patients, and possibly inversely related to the age of the patients at the onset of growth hormone deficiency.
Tabulated list of adverse reactions: Tables 3-5 show the adverse reactions ranked under headings of System Organ Class and frequency using the following convention: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); not known (cannot be estimated from the available data) for each of the indicated conditions. (See Tables 3, 4 and 5).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image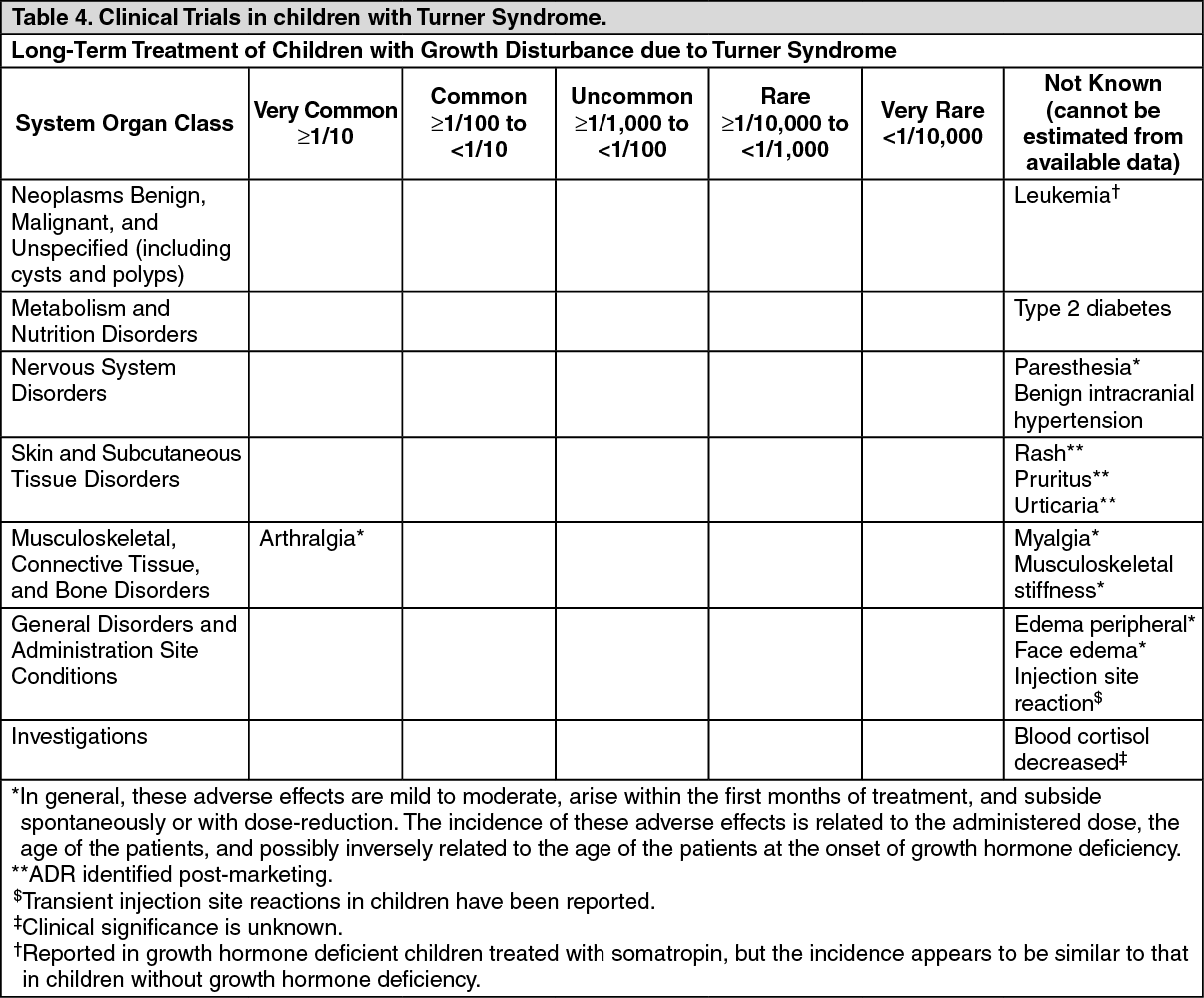 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image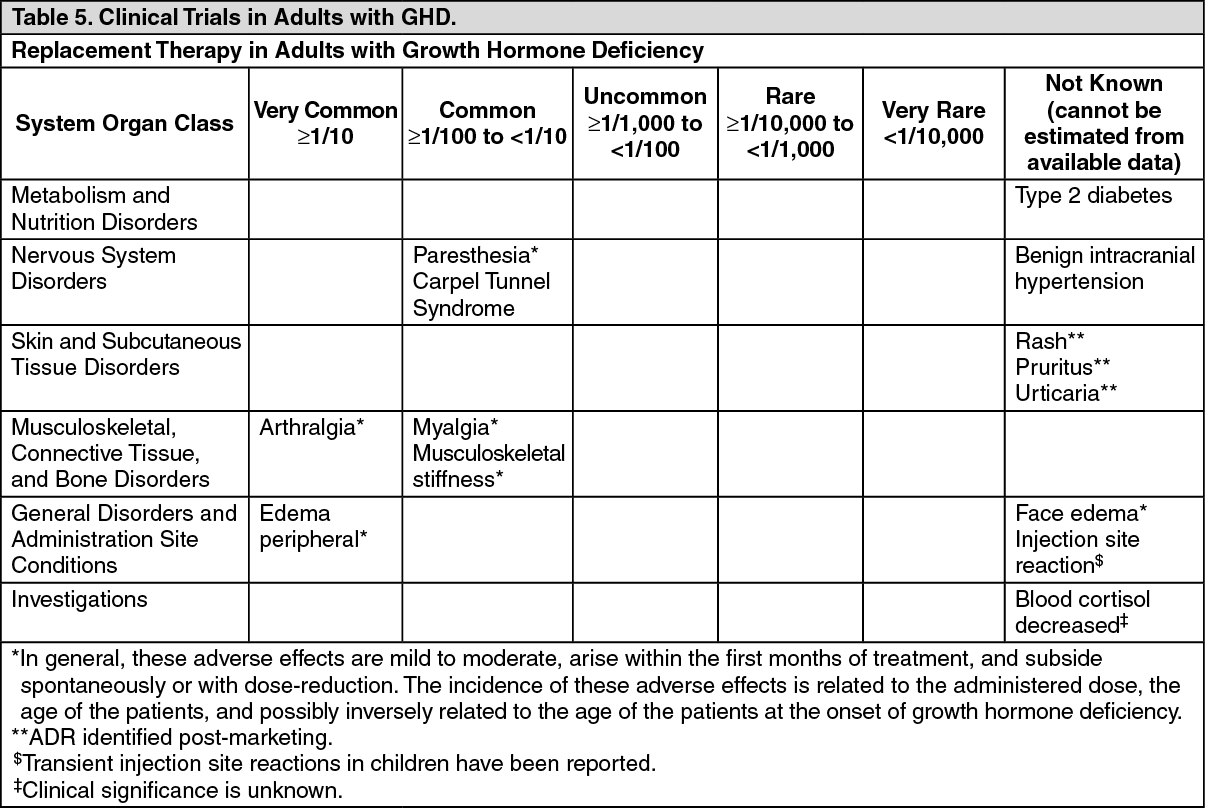 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTransient injection site reactions in children have been reported.
Somatropin has been reported to reduce serum cortisol levels, possibly by affecting carrier proteins or by increased hepatic clearance. The clinical relevance of these findings may be limited. Nevertheless, corticosteroid replacement therapy should be optimized before initiation of Genotropin therapy.
Rare cases of leukemia have been reported in growth hormone deficient children treated with somatropin, but the incidence appears to be similar to that in children without growth hormone deficiency.
Slipped capital femoral epiphysis and Legg-Calve-Perthes disease have been reported in children treated with growth hormone. But, it is unknown if these 2 pathologies are more frequent or not while treated with somatropin.
View ADR Monitoring Form