


 Sign Out
Sign Out


Most adverse reactions are reversible and do not need to result in discontinuation, although doses may need to be withheld or reduced.
Gemcitabine for injection has been used in a wide variety of malignancies, both as a single-agent and in combination with other cytotoxic drugs.
Single-Agent Use: Myelosuppression is the principal dose-limiting toxicity with gemcitabine for injection therapy. Dosage adjustments for hematologic toxicity are frequently needed [see Dosage & Administration].
The data in Table 4 are based on 979 patients receiving gemcitabine for injection as a single-agent administered weekly as a 30-minute infusion for treatment of a wide variety of malignancies. The gemcitabine for injection starting doses ranged from 800 to 1250 mg/m2. Data are also shown for the subset of patients with pancreatic cancer treated in 5 clinical studies. The frequency of all grades and severe (WHO Grade 3 or 4) adverse reactions were generally similar in the single-agent safety database of 979 patients and the subset of patients with pancreatic cancer. Adverse reactions reported in the single-agent safety database resulted in discontinuation of gemcitabine for injection therapy in about 10% of patients. In the comparative trial in pancreatic cancer, the discontinuation rate for adverse reactions was 14.3% for the gemcitabine for injection arm and 4.8% for the 5-FU arm. All WHO-graded laboratory adverse reactions are listed in Table 4, regardless of causality. Non-laboratory adverse reactions listed in Table 4 or discussed as follows were those reported, regardless of causality, for at least 10% of all patients, except the categories of Extravasation, Allergic, and Cardiovascular and certain specific adverse reactions under the Renal, Pulmonary, and Infection categories. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageHematologic: In studies in pancreatic cancer myelosuppression is the dose-limiting toxicity with gemcitabine for injection, but <1% of patients discontinued therapy for either anemia, leukopenia, or thrombocytopenia. Red blood cell transfusions were required by 19% of patients. The incidence of sepsis was less than 1%. Petechiae or mild blood loss (hemorrhage), from any cause, was reported in 16% of patients; less than 1% of patients required platelet transfusions. Patients should be monitored for myelosuppression during gemcitabine for injection therapy and dosage modified or suspended according to the degree of hematologic toxicity [see Dosage & Administration].
Gastrointestinal: Nausea and vomiting were commonly reported (69%) but were usually of mild to moderate severity. Severe nausea and vomiting (WHO Grade 3/4) occurred in <15% of patients. Diarrhea was reported by 19% of patients, and stomatitis by 11% of patients.
Hepatic: In clinical trials, gemcitabine for injection was associated with transient elevations of one or both serum transaminases in approximately 70% of patients, but there was no evidence of increasing hepatic toxicity with either longer duration of exposure to gemcitabine for injection or with greater total cumulative dose. Serious hepatotoxicity, including liver failure and death, has been reported very rarely in patients receiving gemcitabine for injection alone or in combination with other potentially hepatotoxic drugs [see Adverse Reactions].
Renal: In clinical trials, mild proteinuria and hematuria were commonly reported. Clinical findings consistent with the Hemolytic Uremic Syndrome (HUS) were reported in 6 of 2429 patients (0.25%) receiving gemcitabine for injection in clinical trials. Four patients developed HUS on gemcitabine for injection therapy, 2 immediately posttherapy. The diagnosis of HUS should be considered if the patient develops anemia with evidence of microangiopathic hemolysis, elevation of bilirubin or LDH, reticulocytosis, severe thrombocytopenia, and/or evidence of renal failure (elevation of serum creatinine or BUN). Gemcitabine for injection therapy should be discontinued immediately. Renal failure may not be reversible even with discontinuation of therapy and dialysis may be required [see Adverse Reactions].
Fever: The overall incidence of fever was 41%. This is in contrast to the incidence of infection (16%) and indicates that gemcitabine for injection may cause fever in the absence of clinical infection. Fever was frequently associated with other flu-like symptoms and was usually mild and clinically manageable.
Rash: Rash was reported in 30% of patients. The rash was typically a macular or finely granular maculopapular pruritic eruption of mild to moderate severity involving the trunk and extremities. Pruritus was reported for 13% of patients.
Pulmonary: In clinical trials, dyspnea, unrelated to underlying disease, has been reported in association with gemcitabine for injection therapy. Dyspnea was occasionally accompanied by bronchospasm. Pulmonary toxicity has been reported with the use of gemcitabine for injection [see Adverse Reactions]. The etiology of these effects is unknown. If such effects develop, gemcitabine for injection should be discontinued. Early use of supportive care measures may help ameliorate these conditions.
Edema: Edema (13%), peripheral edema (20%), and generalized edema (<1%) were reported. Less than 1% of patients discontinued due to edema.
Flu-like Symptoms: "Flu syndrome" was reported for 19% of patients. Individual symptoms of fever, asthenia, anorexia, headache, cough, chills, and myalgia were commonly reported. Fever and asthenia were also reported frequently as isolated symptoms. Insomnia, rhinitis, sweating, and malaise were reported infrequently. Less than 1% of patients discontinued due to flu-like symptoms.
Infection: Infections were reported for 16% of patients. Sepsis was rarely reported (<1%).
Alopecia: Hair loss, usually minimal, was reported by 15% of patients.
Neurotoxicity: There was a 10% incidence of mild paresthesias and a <1% rate of severe paresthesias.
Extravasation: Injection-site related events were reported for 4% of patients. There were no reports of injection site necrosis. Gemcitabine for injection is not a vesicant.
Allergic: Bronchospasm was reported for less than 2% of patients. Anaphylactoid reaction has been reported rarely. Gemcitabine for injection should not be administered to patients with a known hypersensitivity to this drug [see Contraindications].
Cardiovascular: During clinical trials, 2% of patients discontinued therapy with gemcitabine for injection due to cardiovascular events such as myocardial infarction, cerebrovascular accident, arrhythmia, and hypertension. Many of these patients had a prior history of cardiovascular disease [see Adverse Reactions].
Combination Use in Non-Small Cell Lung Cancer: In the gemcitabine for injection plus cisplatin versus cisplatin study, dose adjustments occurred with 35% of gemcitabine for injection injections and 17% of cisplatin injections on the combination arm, versus 6% on the cisplatin-only arm. Dose adjustments were required in greater than 90% of patients on the combination, versus 16% on cisplatin. Study discontinuations for possibly drug-related adverse reactions occurred in 15% of patients on the combination arm and 8% of patients on the cisplatin arm. With a median of 4 cycles of gemcitabine for injection plus cisplatin treatment, 94 of 262 patients (36%) experienced a total of 149 hospitalizations due to possibly treatment-related adverse reactions. With a median of 2 cycles of cisplatin treatment, 61 of 260 patients (23%) experienced 78 hospitalizations due to possibly treatment-related adverse reactions.
In the gemcitabine for injection plus cisplatin versus etoposide plus cisplatin study, dose adjustments occurred with 20% of gemcitabine for injection injections and 16% of cisplatin injections in the gemcitabine for injection plus cisplatin arm compared with 20% of etoposide injections and 15% of cisplatin injections in the etoposide plus cisplatin arm. With a median of 5 cycles of gemcitabine for injection plus cisplatin treatment, 15 of 69 patients (22%) experienced 15 hospitalizations due to possibly treatment-related adverse reactions. With a median of 4 cycles of etoposide plus cisplatin treatment, 18 of 66 patients (27%) experienced 22 hospitalizations due to possibly treatment-related adverse reactions. In patients who completed more than one cycle, dose adjustments were reported in 81% of the gemcitabine for injection plus cisplatin patients, compared with 68% on the etoposide plus cisplatin arm. Study discontinuations for possibly drug-related adverse reactions occurred in 14% of patients on the gemcitabine for injection plus cisplatin arm and in 8% of patients on the etoposide plus cisplatin arm. The incidence of myelosuppression was increased in frequency with gemcitabine for injection plus cisplatin treatment (~90%) compared to that with the gemcitabine for injection monotherapy (~60%). With combination therapy gemcitabine for injection dosage adjustments for hematologic toxicity were required more often while cisplatin dose adjustments were less frequently required.
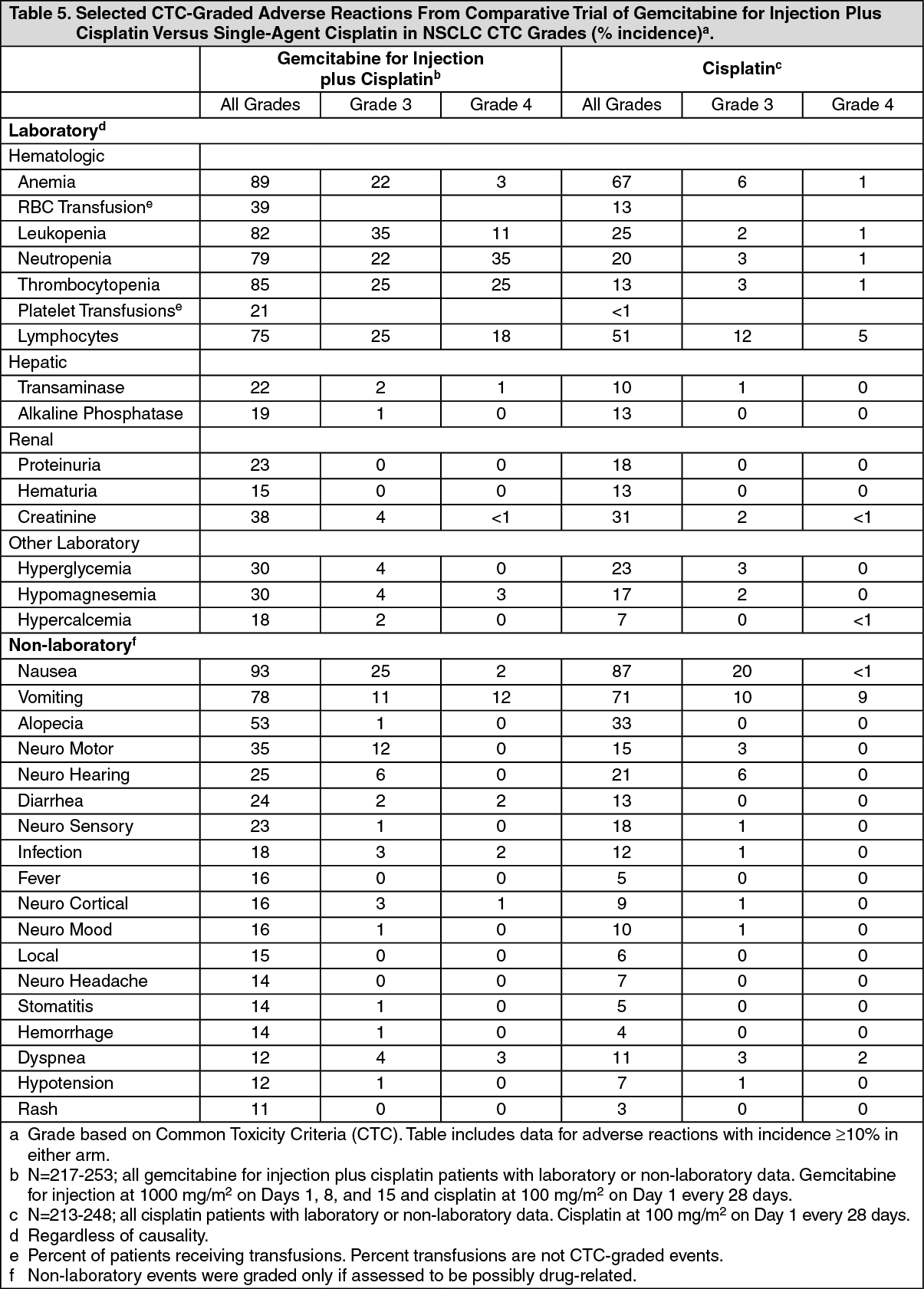
Table 5 presents the safety data from the gemcitabine for injection plus cisplatin versus cisplatin study in non-small cell lung cancer. The NCI Common Toxicity Criteria (CTC) were used. The two-drug combination was more myelosuppressive with 4 (1.5%) possibly treatment-related deaths, including 3 resulting from myelosuppression with infection and one case of renal failure associated with pancytopenia and infection. No deaths due to treatment were reported on the cisplatin arm. Nine cases of febrile neutropenia were reported on the combination therapy arm compared to 2 on the cisplatin arm. More patients required RBC and platelet transfusions on the gemcitabine for injection plus cisplatin arm.
Myelosuppression occurred more frequently on the combination arm, and in 4 possibly treatment-related deaths myelosuppression was observed. Sepsis was reported in 4% of patients on the gemcitabine for injection plus cisplatin arm compared to 1% on the cisplatin arm. Platelet transfusions were required in 21% of patients on the combination arm and <1% of patients on the cisplatin arm. Hemorrhagic events occurred in 14% of patients on the combination arm and 4% on the cisplatin arm. However, severe hemorrhagic events were rare. Red blood cell transfusions were required in 39% of the patients on the gemcitabine for injection plus cisplatin arm, versus 13% on the cisplatin arm. The data suggest cumulative anemia with continued gemcitabine for injection plus cisplatin use.
Nausea and vomiting despite the use of antiemetics occurred more often with gemcitabine for injection plus cisplatin therapy (78%) than with cisplatin alone (71%). In studies with single-agent gemcitabine for injection, a lower incidence of nausea and vomiting (58% to 69%) was reported. Renal function abnormalities, hypomagnesemia, neuromotor, neurocortical, and neurocerebellar toxicity occurred more often with gemcitabine for injection plus cisplatin than with cisplatin monotherapy. Neurohearing toxicity was similar on both arms.
Cardiac dysrrhythmias of Grade 3 or greater were reported in 7 (3%) patients treated with gemcitabine for injection plus cisplatin compared to one (<1%) Grade 3 dysrrhythmia reported with cisplatin therapy. Hypomagnesemia and hypokalemia were associated with one Grade 4 arrhythmia on the gemcitabine for injection plus cisplatin combination arm.
Table 6 presents data from the randomized study of gemcitabine for injection plus cisplatin versus etoposide plus cisplatin in 135 patients with NSCLC. One death (1.5%) was reported on the gemcitabine for injection plus cisplatin arm due to febrile neutropenia associated with renal failure which was possibly treatment-related. No deaths related to treatment occurred on the etoposide plus cisplatin arm. The overall incidence of Grade 4 neutropenia on the gemcitabine for injection plus cisplatin arm was less than on the etoposide plus cisplatin arm (28% versus 56%). Sepsis was experienced by 2% of patients on both treatment arms. Grade 3 anemia and Grade 3/4 thrombocytopenia were more common on the gemcitabine for injection plus cisplatin arm. RBC transfusions were given to 29% of the patients who received gemcitabine for injection plus cisplatin versus 21% of patients who received etoposide plus cisplatin. Platelet transfusions were given to 3% of the patients who received gemcitabine for injection plus cisplatin versus 8% of patients who received etoposide plus cisplatin. Grade 3/4 nausea and vomiting were also more common on the gemcitabine for injection plus cisplatin arm. On the gemcitabine for injection plus cisplatin arm, 7% of participants were hospitalized due to febrile neutropenia compared to 12% on the etoposide plus cisplatin arm. More than twice as many patients had dose reductions or omissions of a scheduled dose of gemcitabine for injection as compared to etoposide, which may explain the differences in the incidence of neutropenia and febrile neutropenia between treatment arms. Flu syndrome was reported by 3% of patients on the gemcitabine for injection plus cisplatin arm with none reported on the comparator arm. Eight patients (12%) on the gemcitabine for injection plus cisplatin arm reported edema compared to one patient (2%) on the etoposide plus cisplatin arm. (See Tables 5 and 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
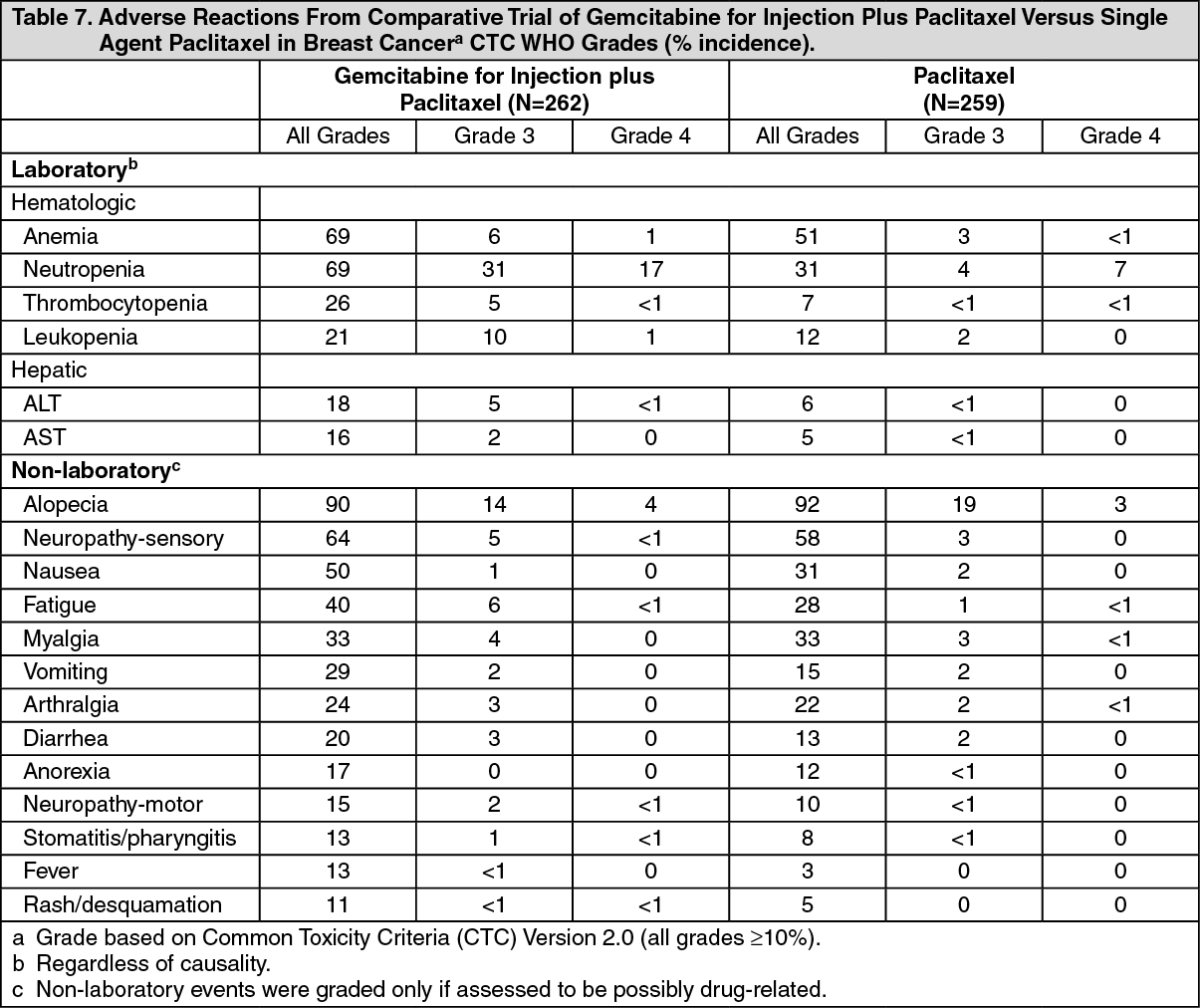
Click on icon to see table/diagram/imageCombination Use in Breast Cancer: In the gemcitabine for injection plus paclitaxel versus paclitaxel study, dose reductions occurred with 8% of gemcitabine for injection injections and 5% of paclitaxel injections on the combination arm, versus 2% on the paclitaxel arm. On the combination arm, 7% of gemcitabine for injection doses were omitted and <1% of paclitaxel doses were omitted, compared to <1% of paclitaxel doses on the paclitaxel arm. A total of 18 patients (7%) on the gemcitabine for injection plus paclitaxel arm and 12 (5%) on the paclitaxel arm discontinued the study because of adverse reactions. There were two deaths on study or within 30 days after study drug discontinuation that were possibly drug-related, one on each arm.
Table 7 presents the safety data occurrences of ≥10% (all grades) from the gemcitabine for injection plus paclitaxel versus paclitaxel study in breast cancer. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe following are the clinically relevant adverse reactions that occurred in >1% and <10% (all grades) of patients on either arm. In parentheses are the incidences of Grade 3 and 4 adverse reactions (gemcitabine for injection plus paclitaxel versus paclitaxel): febrile neutropenia (5.0% versus 1.2%), infection (0.8% versus 0.8%), dyspnea (1.9% versus 0), and allergic reaction/hypersensitivity (0 versus 0.8%).
No differences in the incidence of laboratory and non-laboratory events were observed in patients 65 years or older, as compared to patients younger than 65.
View ADR Monitoring Form