Active ingredient: Levothyroxine sodium.
1 tablet Euthyrox 25 μg contains 25 microgram levothyroxine sodium.
1 tablet Euthyrox 50 μg contains 50 microgram levothyroxine sodium.
1 tablet Euthyrox 75 μg contains 75 microgram levothyroxine sodium.
1 tablet Euthyrox 100 μg contains 100 microgram levothyroxine sodium.
Excipients/Inactive Ingredients: Corn starch, croscarmellose sodium, gelatine, magnesium stearate, citric acid, mannitol.
Pharmacological class: Thyroid hormones. ATC code: H03A A01.
Pharmacology: Pharmacodynamics: The synthetic levothyroxine is identical in effect with the naturally occurring major hormone secreted by the thyroid. It is converted to T3 in peripheral organs and, like the endogenous hormone, develops its specific effects at the T3 receptors. The body is not able to differentiate between endogenous and exogenous levothyroxine.
Pharmacokinetics: Orally given levothyroxine is absorbed almost exclusively in the upper small intestine. Depending on the galenic formulation absorption amounts up to 80%. tmax is approximately 5 - 6 hours.
Following oral administration the onset of action is seen after 3 - 5 days. Levothyroxine exhibits an extremely high binding to specific transport proteins of about 99.97%. This protein hormone binding is not covalent and so the bound hormone in plasma is in continuous and very rapid exchange with the fraction of the free hormone.
Due to its high protein binding levothyroxine cannot be eliminated via haemodialysis or haemoperfusion.
The half-life of levothyroxine is on average 7 days. In hyperthyroidism it is shorter (3 -4 days) and in hypothyroidism it is longer (approx. 9 - 10 days). The volume of distribution amounts to about 10 - 12 l. The liver contains 1/3 of the entire extra-thyroidal levothyroxine, which is rapidly exchangeable with the levothyroxine in serum. Thyroid hormones are metabolised mainly in the liver, kidneys, brain and muscles. The metabolites are excreted with urine and faeces. The overall metabolic clearance for levothyroxine is about 1.2 l plasma per day.
Treatment of benign euthyroid goitre; Prophylaxis of relapse after surgery for euthyroid goitre; Substitution therapy in hypothyroidism; Concomitant therapy during anti-thyroid medicinal treatment of hyperthyroidism; Suppression therapy in thyroid cancer.
Applies only to tablets of 100 microgram: Diagnostic use for thyroid suppression testing.
In order to treat each patient according to his/her individual needs, tablets are available with a levothyroxine sodium content ranging from 25 - 200 microgram. Patients therefore usually need to take only one tablet per day.
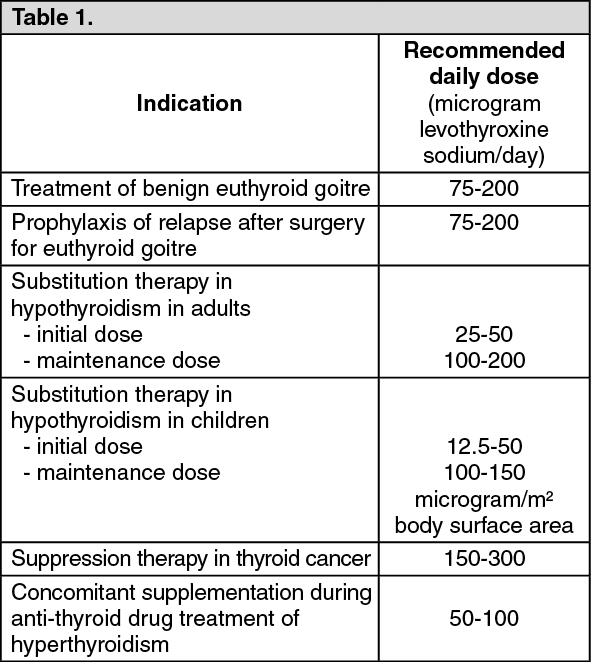
The dosage recommendations given are only for guidance. Determination of the individual daily dose on the basis of laboratory tests and clinical examinations is recommended.
In children with a sound heart, and for neonates where rapid replacement is important, the entire dose may be started. In adults, initiation of thyroid hormone therapy at low dose is recommended. The dose may be increased gradually every 2 - 4 weeks until the full replacement dose is reached.
In elderly patients, in patients with coronary heart disease, and in patients with severe or long-existing hypothyroidism, special caution is required when initiating therapy with thyroid hormones: Treatment is initiated at a low dose, which is increased slowly and at lengthy intervals with frequent monitoring of thyroid hormones. A maintenance dose lower than that required for complete correction of TSH levels may be considered.
Experience has shown that a lower dose is sufficient in low-weight patients and in patients with a large nodular goitre. (See Table 1.)
 Click on icon to see table/diagram/image
Applies only to tablets of 100 microgram:
Click on icon to see table/diagram/image
Applies only to tablets of 100 microgram: (See Table 2.)
Click on icon to see table/diagram/image
Administration: The daily doses can be given in a single administration.
Ingestion: as a single daily dose in the morning on an empty stomach, half an hour before breakfast, preferably with a little liquid (for example, half a glass of water).
Infants receive the entire dose at once at least 30 minutes before the first meal of the day.
Tablets are suspended in some water and the resultant suspension is administered with some more liquid. The suspension must be prepared freshly prior to each administration.
Duration of treatment: In the case of substitution in hypothyroidism and after strumectomy or thyroidectomy as well as for relapse prophylaxis after euthyroid goitre removal treatment is usually continued for lifespan.
Concomitant therapy of hyperthyroidism after achieving euthyroid status is indicated for the period in which the anti-thyroid agent is given.
For benign euthyroid goitre, treatment duration is for some months up to lifespan. If the medical treatment was not sufficient within this time, surgery or radioiodine therapy of the goitre should be considered.
Symptoms: Overdose may cause symptoms of a significant increase in the metabolic rate. For typical symptoms, see "Adverse Reactions".
In predisposed patients isolated cases of seizures have been reported when the individual dose tolerance limit was exceeded. Overdose of levothyroxine may result in hyperthyroidism and could lead to symptoms of acute psychosis, especially in patients at risk of psychotic disorders.
Several cases of sudden cardiac death have been reported in patients with long years of levothyroxine abuse.
Management: An elevated T3 level is a reliable indicator of overdose, more than elevated T4 or fT4 levels.
Depending on the extent of the overdose it is recommended that treatment is interrupted and that tests are carried out.
Beta-sympathomimetic effects such as tachycardia, anxiety, agitation or hyperkinesia can be relieved by betablockers. After extreme doses plasmapheresis may be indicated.
Euthyrox must not be used in patients with: hypersensitivity to any of the excipients of the product (see 'Description'); untreated adrenal insufficiency; untreated pituitary insufficiency; hyperthyroidism or untreated thyrotoxicosis, including untreated subclinical (suppressed serum TSH level with normal T3 and T4 levels) hyperthyroidism.
Treatment with levothyroxine must not be initiated in patients with acute myocardial infarction, acute myocarditis, or acute pancarditis.
Combination therapy of Euthyrox and an antithyroid agent for hyperthyroidism is not indicated during pregnancy.
Thyroid hormones should not be given for weight reduction. In euthyroid patients, treatment with levothyroxine does not cause weight reduction. Substantial doses may cause serious or even life-threatening undesirable effects, particularly in combination with certain substances for weight reduction, and especially with sympathomimetic amines (see also 'Overdosage').
Before starting therapy with thyroid hormones or before performing a thyroid suppression test, the following diseases or medical conditions must be excluded or treated: coronary insufficiency, angina pectoris, arteriosclerosis, hypertension, pituitary insufficiency or adrenal insufficiency.
Thyroid autonomy should also be excluded or treated before starting therapy with thyroid hormones.
When initiating levothyroxine therapy in patients at risk of psychotic disorders, it is recommended to start at a low levothyroxine dose and to slowly increase the dosage at the beginning of the therapy. Monitoring of the patient is advised. If signs of psychotic disorders occurs, adjustment of the dose of levothyroxine should be considered.
Even slight drug-induced hyperthyroidism must be avoided in patients with coronary insufficiency, heart failure or tachycardiac arrhythmias. Hence frequent checks of thyroid hormone parameters must be made in these cases.
The aetiology of secondary hypothyroidism must be determined before thyroid hormone replacement therapy is given. If necessary replacement treatment of a compensated adrenal insufficiency must be commenced.
Where thyroid autonomy is suspected, a TRH test or a suppression scintigram is recommended before initiation of treatment.
Haemodynamic parameters should be monitored when levothyroxine therapy is initiated in very low birth weight preterm neonates as circulatory collapse may occur due to the immature adrenal function.
In postmenopausal women with hypothyroidism and an increased risk of osteoporosis supraphysiological serum levels of levothyroxine have to be avoided. Therefore, close monitoring of the thyroid function is recommended.
Levothyroxine is not recommended in hyperthyroid metabolic states. An exception is the concomitant supplementation during anti-thyroid drug treatment of hyperthyroidism.
If a switch to another levothyroxine-containing product is required, there is a need to undertake close clinical monitoring, which may include a laboratory test, during the transition period due to a potential risk of thyroid imbalance. In some patients, a dose adjustment could be necessary.
Hypothyroidism and / or reduced control of hypothyroidism may occur when orlistat and levothyroxine are co-administered (see 'Interactions'). Patients taking levothyroxine should consult a doctor before starting treatment with orlistat, as orlistat and levothyroxine may need to be taken at different times and the dose of levothyroxine may need to be adjusted. Further, it is recommended to monitor the patient by checking the hormone levels in the serum.
Biotin may interfere with thyroid immunoassays that are based on a biotin/streptavidin interaction, leading to either falsely decreased or falsely increased test results. The risk of interference increases with higher doses of biotin.
When interpreting results of laboratory tests, possible biotin interference has to be taken into consideration, especially if a lack of coherence with the clinical presentation is observed. For patients taking biotin-containing products, laboratory personnel should be informed when a thyroid function test is requested. Alternative tests not susceptible to biotin interference should be used, if available (see Interactions).
Effects on bone mineral density: In women, long-term levothyroxine sodium therapy has been associated with increased bone resorption, thereby decreasing bone mineral density, especially in post-menopausal women on greater than replacement doses or in women who are receiving suppressive doses of levothyroxine sodium. The increased bone resorption may be associated with increased serum levels and urinary excretion of calcium and phosphorus, elevations in bone alkaline phosphatase and suppressed serum parathyroid hormone levels. Therefore, it is recommended that patients receiving levothyroxine sodium be given the minimum dose necessary to achieve a desired clinical and biochemical response.
Effects on the ability to drive and use machines: No studies on the effects on the ability to drive and use machines have been performed. However, since levothyroxine is identical to the naturally occurring thyroid hormone, it is not expected that Euthyrox has any influence on the ability to drive and use machines, if used as recommended.
Treatment with thyroid hormones should be given consistently during pregnancy and breastfeeding in particular. Dosage requirements may even increase during pregnancy. Since elevations in serum TSH may occur as early as 4 weeks of gestation, pregnant women taking levothyroxine should have their TSH measured during each trimester, in order to confirm that the maternal serum TSH values lie within the trimester-specific pregnancy reference range. An elevated serum TSH level should be corrected by an increase in the dose of levothyroxine. Since postpartum TSH levels are similar to preconception values, the levothyroxine dosage should return to the pre-pregnancy dose immediately after delivery. A serum TSH level should be obtained 6-8 weeks postpartum.
Pregnancy: Thyroid suppression diagnostic tests must be avoided during pregnancy, as the application of radioactive substances in pregnant women is contraindicated.
There is no evidence of drug-induced teratogenicity and/or foeto-toxicity in humans at the recommended therapeutic dose level. Excessively high dose levels of levothyroxine during pregnancy may have a negative effect on foetal and postnatal development.
Combination therapy of hyperthyroidism with levothyroxine and anti-thyroid agents is not indicated during pregnancy. Such combination would require higher doses of anti-thyroid agents, which are known to pass the placenta and to induce hypothyroidism in the infant.
Lactation: Levothyroxine is secreted into breast milk during lactation but the concentrations achieved at the recommended therapeutic dose level are not sufficient to cause development of hyperthyroidism or suppression of TSH secretion in the infant.
Clinical signs of hyperthyroidism may occur in case of overdose, if the individual tolerance limit for levothyroxine is exceeded, or if the dose is increased too fast at the start of treatment. The following symptoms are typical: tachycardia, palpitation, cardiac arrhythmias (e.g. atrial fibrillation and extrasystoles), angina pectoris, headache, muscular weakness and cramps, flushing, fever, vomiting, disorders of menstruation, pseudotumour cerebri, tremor, restlessness, insomnia, hyperhidrosis, weight loss, diarrhoea.
In such cases the daily dose has to be reduced or the medication withdrawn for several days. Therapy may carefully be resumed once the adverse reactions have disappeared.
In case of hypersensitivity to any of the ingredients of Euthyrox allergic reactions, particularly of the skin, may occur. Cases of angioedema have been reported.
Protease inhibitors: Protease inhibitors (e.g. ritonavir, indinavir, lopinavir) may influence the effect of levothyroxine. Close monitoring of thyroid hormone parameters is recommended. If necessary, the levothyroxine dose has to be adjusted.
Phenytoin: Phenytoin may influence the effect of levothyroxine by displacing levothyroxine from plasma proteins resulting in an elevated fT4 and fT3 fraction. On the other hand, phenytoin increases the hepatic metabolisation of levothyroxine. Close monitoring of thyroid hormone parameters is recommended.
Influence of levothyroxine on other medicinal products: Anti-diabetic medicinal products: Levothyroxine may reduce the effect of anti-diabetics. Therefore, it is necessary to check blood glucose levels frequently at the start of thyroid hormone therapy. If necessary, the anti-diabetic dose has to be adjusted.
Coumarin derivates: Levothyroxine may intensify the effect of anticoagulants by displacing them from plasma protein bounds, which may increase the risk of haemorrhage e.g. CNS or gastrointestinal bleeding, especially in elderly patients. Therefore, it is necessary to check the coagulation parameters regularly at the start of and during concomitant therapy. If necessary, the anticoagulant dose has to be adjusted.
The following medicinal products intensify the effect of levothyroxine: Salicylates, dicumarol, furosemide, clofibrate: Salicylates, dicumarol, furosemide in high doses (250 mg), clofibrate and other substances can displace levothyroxine from plasma proteins, resulting in an elevated fT4 fraction.
The following medicinal products may reduce the effect of levothyroxine: Proton pump inhibitors (PPIs): Possible decrease in the absorption of the thyroid hormones, due to the increase of the intragastric pH caused by PPIs. Regular biological and clinical monitoring, with a possible increase in the dose of thyroid hormones.
Orlistat: Hypothyroidism and / or reduced control of hypothyroidism may occur when orlistat and levothyroxine are taken at the same time. This could be due to a decreased absorption of iodine salts and / or levothyroxine.
Sevelamer: Sevelamer may decrease levothyroxine absorption. Therefore, it is recommended that patients are monitored for changes in thyroid function at the start or end of concomitant treatment. If necessary, the levothyroxine dose has to be adjusted.
Tyrosine kinase inhibitors: Tyrosine kinase inhibitors (e.g. imatinib, sunitinib) may decrease the efficacy of levothyroxine. Therefore, it is recommended that patients are monitored for changes in thyroid function at the start or end of concomitant treatment. If necessary, the levothyroxine dose has to be adjusted.
Ion exchange resins: Ion exchange resins (e.g. cholestyramine or cholestipol) inhibit the absorption of levothyroxine. It is therefore recommended that levothyroxine be taken 4 - 5 hours before administration of such agents.
Aluminium, iron and calcium salts: Aluminium-containing medicinal products (antacids, sucralfate) have been reported in literature as potentially decreasing the effect of levothyroxine. It is therefore recommended that levothyroxine be administered at least 2 hours prior to the administration of aluminium-containing medicinal products. The same applies to medicinal products containing iron and calcium salts.
Propylthiouracil, glucocorticoids, beta-sympatholytics, and iodine-containing contrast media: These substances inhibit the peripheral conversion of T4 to T3.
Amiodarone: This substance inhibits the peripheral conversion of T4 to T3.
Due to its high iodine content amiodarone can trigger hyperthyroidism as well as hypothyroidism. Particular caution is advised in the case of nodular goiter with possibly unrecognised autonomy.
Sertraline, chloroquine/proguanil: These substances decrease the efficacy of levothyroxine and increase the serum TSH level.
Medicinal products leading to hepatic enzyme induction (e.g. barbiturates, carbamazepine): These substances can increase the hepatic clearance of levothyroxine.
Oestrogens: Women using oestrogen-containing contraceptives or postmenopausal women under hormone-replacement therapy may have an increased need for levothyroxine.
Interaction with food: Soy containing compounds: Soy containing compounds can decrease the intestinal absorption of levothyroxine. Therefore, a dosage adjustment of Euthyrox may be necessary, in particular at the beginning or after termination of nutrition with soy supplements.
Interference with laboratory test: Biotin may interfere with thyroid immunoassays that are based on a biotin/streptavidin interaction, leading to either falsely decreased or falsely increased test results (see Precautions).
Keep the container of Euthyrox in the outer carton. Do not store above 30°C. Protect from light.
H03AA01 - levothyroxine sodium ; Belongs to the class of thyroid hormones.
Euthyrox tab 100 mcg
4 × 25's
Euthyrox tab 25 mcg
4 × 25's
Euthyrox tab 50 mcg
4 × 25's
Euthyrox tab 75 mcg
4 × 25's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image




 Sign Out
Sign Out
