Pharmacotherapeutic Group: Sex hormones and modulators of the genital system; Progestogens; Pregnen-(4) derivatives.
ATC Code: G03DA04.
Pharmacology: Pharmacodynamics: Mechanism of Action: Progesterone is a naturally occurring steroid that is secreted by the ovary, placenta, and adrenal gland. In the presence of adequate estrogen, progesterone transforms a proliferative endometrium into a secretory endometrium. Progesterone is necessary to increase endometrial receptivity for implantation of an embryo. Once an embryo is implanted, progesterone acts to maintain the pregnancy.
Clinical Efficacy and Safety: A randomized, open-label, active-controlled study evaluated the efficacy of treatment with two different daily dosing regimens of ENDOMETRIN (100 mg twice daily and 100 mg three times daily) for luteal support as part of an Assisted Reproductive Technology (ART) treatment program for infertile women. The study included 1,211 women, of whom 1,175 women underwent embryo transfer (n=392 ENDOMETRIN 100 mg BID, n=390 ENDOMETRIN 100 mg TID and n=393 active comparator). Subjects ranged in age from 19 to 42 years.
The study drug was initiated on the day after oocyte retrieval and was continued for a total duration of approximately 10 weeks if the patient conceived. The patient population in this study was pre-stratified and randomised according to age (<35, 35-37, 38-40, 41-42 years). Women up to 35 years of age constituted 61% (N=737) of the trial population and the majority had FSH levels <10 IU/L (N=1,047/1,193, 88%). The study was powered to demonstrate non-inferiority overall for the entire trial population, not for each of the age groups.
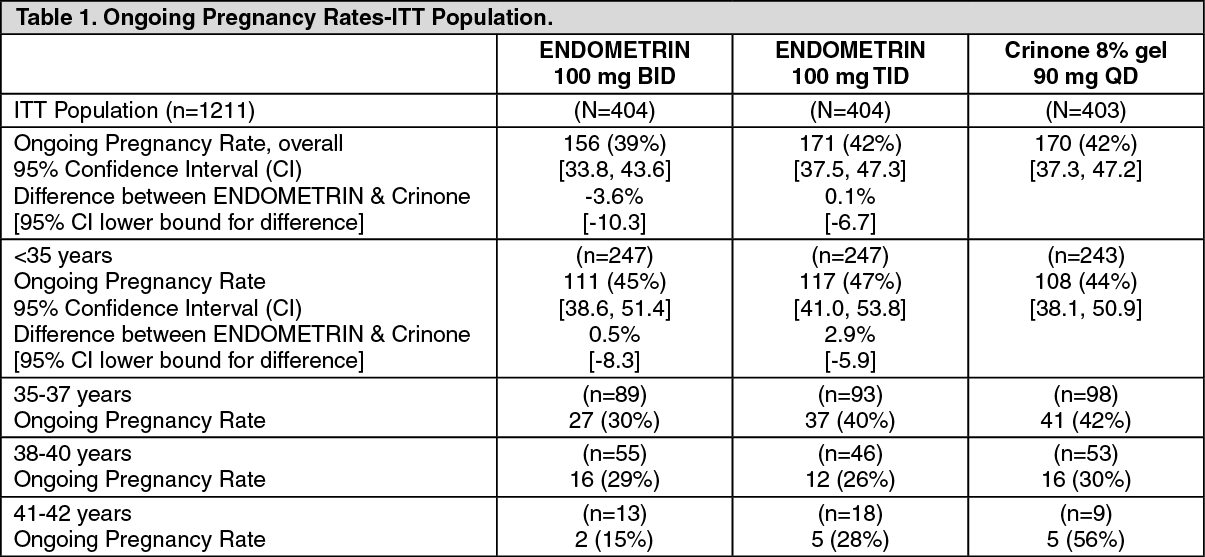
The primary efficacy variable was ongoing pregnancy rate which was defined as the identification of foetal heart movement at approximately 6 weeks of gestation. The ongoing pregnancy rate in the study were as follows overall, and per age-strata. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
ENDOMETRIN 100 mg TID met the non-inferiority criterion relative to CRINONE 8%, as ENDOMETRIN TID was well within the 10% lower bound to demonstrate non-inferiority in ongoing pregnancy rate to CRINONE 8%. ENDOMETRIN BID was just above the 10% lower bound in ongoing pregnancy rate.
Ongoing pregnancy and live birth rates following 10-week luteal support with ENDOMETRIN PESSARIES are available from the Phase III clinical trial. ENDOMETRIN 100 mg BID (N=392) was associated with an ongoing pregnancy rate of 39.8% (95% CI 34.9; 44.9) and a live birth rate of 36.0% (95% CI 31.2; 40.9) in patients who had an embryo transfer. For ENDOMETRIN 100 mg TID (N=390), the ongoing pregnancy and live birth rates in patients with embryo transfer were 43.8% (95% CI 38.9; 48.9) and 39.5% (95% CI 34.6; 44.5), respectively.
Pharmacokinetics: Absorption: Progesterone serum concentrations increased following the administration of the ENDOMETRIN vaginal tablets in 12 healthy premenopausal females. On day 1 of treatment, the mean C
max 19.8 ± 2.9 ng/mL with a T
max of 17.3 ± 3.0 hours after administration of ENDOMETRIN three times daily 8 hours apart.
On multiple dosing, steady state concentrations were attained within approximately 1 day after initiation of treatment with ENDOMETRIN. Trough values of 10.9 ± 2.7 ng/mL were observed with an AUC
0-24 of 436 ± 43 ng*hr/mL on Day 5.
Distribution: Progesterone is approximately 96% to 99% bound to serum proteins, primarily to serum albumin and corticosteroid binding globulin.
Biotransformation: Progesterone is metabolized primarily by the liver largely to pregnanediols and pregnanolones. Pregnanediols and pregnanolones are conjugated in the liver to glucuronide and sulfate metabolites. Progesterone metabolites that are excreted in the bile may be deconjugated and may be further metabolized in the gut via reduction, dehydroxylation, and epimerization.
Elimination: Progesterone undergoes renal and biliary elimination.
Following injection of labelled progesterone, 50-60% of the excretion of metabolites occurs via the kidney; approximately 10% occurs via the bile and faeces. Overall recovery of the labelled material accounts for 70% of an administered dose. Only a small portion of unchanged progesterone is excreted in the bile.
Toxicology: Preclinical Safety Data: Progesterone is a well known natural reproductive steroidal hormone in humans and animals, with no known toxicological effects. Therefore no toxicity studies have been performed with this progesterone vaginal dosage form, with the exception of local tolerance and skin sensitization studies.
ENDOMETRIN was found to be non-irritative for up to 90 days of twice daily vaginal administration in rabbits, and was also shown to be non-sensitising in Guinea pigs.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
