ELIGARD 7.5 mg: One prefilled syringe with powder for solution for injection contains 7.5 mg leuprorelin acetate, equivalent to 6.96 mg leuprorelin.
ELIGARD 22.5 mg: One prefilled syringe with powder for solution for injection contains 22.5 mg leuprorelin acetate, equivalent to 20.87 mg leuprorelin.
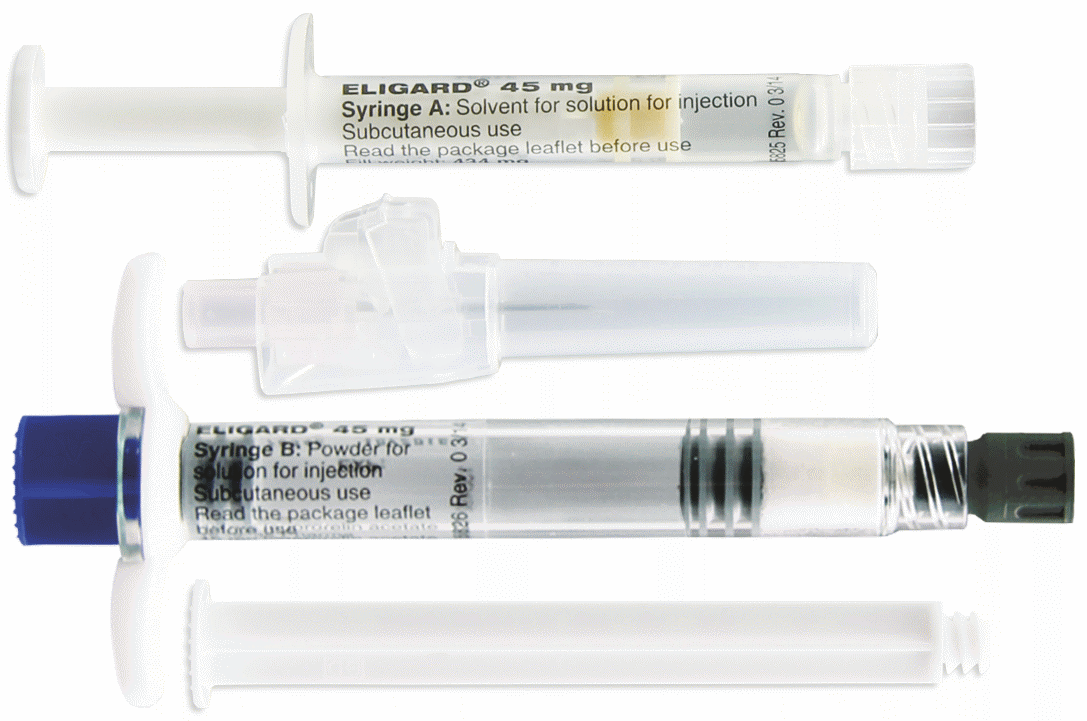
ELIGARD 45 mg: One prefilled syringe with powder for solution for injection contains 45 mg leuprorelin acetate, equivalent to 41.7 mg leuprorelin.
Excipients/Inactive Ingredients: ELIGARD 7.5 mg: Solvent (syringe A): Poly (DL-lactic-co-glycolic-acid) (50:50); N-Methyl-pyrrolidone.
ELIGARD 22.5 mg: Solvent (syringe A): Poly (DL-lactic-co-glycolic-acid) (75:25); N-Methylpyrrolidone.
ELIGARD 45 mg: Solvent (syringe A): Poly (DL-lactic-co-glycolic-acid) (85:15); N-Methylpyrrolidone.
Powder (syringe B): None.
Pharmacotherapeutic group: Gonadotropin releasing hormone analogues. ATC code: L02A E02.
Pharmacology: Pharmacodynamics: Leuprorelin acetate is a synthetic nonapeptide agonist of naturally occurring gonadotropin releasing hormone (GnRH) that, when given continuously, inhibits pituitary gonadotropin secretion and suppresses testicular steroidogenesis in males. This effect is reversible upon discontinuation of medicinal product therapy. However, the agonist possesses greater potency than the natural hormone and the time to recovery of testosterone levels may vary between patients.
Administration of leuprorelin acetate results in an initial increase in circulating levels of luteinising hormone (LH) and follicle stimulating hormone (FSH), leading to a transient increase in levels of the gonadal steroids, testosterone and dihydrotestosterone in males. Continuous administration of leuprorelin acetate results in decreased levels of LH and FSH. In males, testosterone is reduced to below castrate threshold (≤ 50 ng/dL).
ELIGARD 7.5 mg: These decreases occur within three to five weeks after initiation of treatment. Mean testosterone levels at six months are 6.1 (± 0.4) ng/dL, comparable to levels following bilateral orchiectomy. All patients in the pivotal clinical study reached castrate levels at 6 weeks; 94% had reached this by day 28 and 98% by day 35. In the vast majority of patients the testosterone levels seen were below 20 ng/dL although the full benefit of these low levels has not yet been established. PSA levels decreased by 94% over six months.
ELIGARD 22.5 mg: These decreases occur within three to five weeks after initiation of treatment. Mean testosterone levels at six months are 10.1 (± 0.7) ng/dL, comparable to levels following bilateral orchiectomy. All patients who received the full dose of 22.5 mg leuprorelin in the pivotal clinical study reached castrate levels at 5 weeks; 99% had reached this by day 28. In the vast majority of patients the testosterone levels seen were below 20 ng/dL although the full benefit of these low levels has not yet been established. PSA levels decreased by 98% over six months.
ELIGARD 45 mg: These decreases occur within three to four weeks after initiation of treatment. Mean testosterone levels at six months are 10.4 (± 0.53) ng/dL, comparable to levels following bilateral orchiectomy. All but one patient who received the full dose of 45 mg leuprorelin in the pivotal clinical study reached castrate levels at 4 weeks. In the vast majority of patients the testosterone levels seen were below 20 ng/dL although the full benefit of these low levels has not yet been established. PSA levels decreased by 97% over six months.
Long-term studies have shown that continuation of therapy maintains testosterone below the castrate level for up to seven years, and presumably indefinitely.
Tumour size was not measured directly during the clinical trial programme, but there was an indirect beneficial tumour response as shown by a 94% reduction in mean PSA for ELIGARD 7.5 mg, 98% reduction for ELIGARD 22.5 mg and 97% reduction for ELIGARD 45 mg.
Pharmacokinetics: Absorption: ELIGARD 7.5 mg: In patients with advanced carcinoma of the prostate, mean serum leuprorelin concentrations following the initial injection rise to 25.3 ng/ml at 4-8 hr (Cmax) after injection. After the initial increase following each injection (the plateau phase from 2-28 days after each dose), serum concentrations remain relatively constant (0.28 - 1.67 ng/ml). There is no evidence of accumulation during repeated dosing.
ELIGARD 22.5 mg: In patients with advanced carcinoma of the prostate, mean serum leuprorelin concentrations following the initial injection rise to 127 ng/ml at 4.6 hr (Cmax) after injection. After the initial increase following each injection (the plateau phase from 3 - 84 days after each dose), serum concentrations remained relatively constant (0.2 - 2 ng/ml). There is no evidence of accumulation during repeated dosing.
ELIGARD 45 mg: In patients with advanced carcinoma of the prostate, mean serum leuprorelin concentrations following the initial injection rise to 82 ng/ml at 4.4 hr (Cmax) after injection. After the initial increase following each injection (the plateau phase from 3 - 168 days after each dose), serum concentrations remained relatively constant (0.2 - 2 ng/ml). There is no evidence of accumulation during repeated dosing.
Distribution: The mean steady-state volume of distribution of leuprorelin following intravenous bolus administration to healthy male volunteers was 27 litres. In vitro binding to human plasma proteins ranged from 43% to 49%.
Elimination: In healthy male volunteers, a 1 mg bolus of leuprorelin acetate administered intravenously revealed that the mean systemic clearance was 8.34 l/h, with a terminal elimination half-life of approximately 3 hours based on a two compartment model.
No excretion studies have been conducted with ELIGARD.
No drug metabolism study was conducted with ELIGARD.
Toxicology: Preclinical safety data: Preclinical studies with leuprorelin acetate, revealed in both sexes effects on the reproductive system, including atrophy of the reproductive organs and suppression of reproductive function, which were expected from the known pharmacological properties. These effects were shown to be reversible after discontinuation of the treatment and an appropriate period of regeneration. Leuprorelin acetate did not show teratogenicity. Embryotoxicity/lethality was observed in rabbits, in line with the pharmacological effects of leuprorelin acetate on the reproductive system.
Carcinogenicity studies were performed in rats and mice over 24 months. In rats, a dose-related increase in pituitary apoplexy was observed after subcutaneous administration at doses of 0.6 to 4 mg/kg/day. No such effect was observed in mice.
Leuprorelin acetate and related one-month product ELIGARD 7.5 mg were not mutagenic in a set of in vitro and in vivo assays.
ELIGARD is indicated for the palliative treatment of hormone dependent advanced prostate cancer.
Posology: Adult Males: ELIGARD should be administered under the direction of a healthcare professional having available the appropriate expertise for monitoring the response to treatment.
ELIGARD 7.5 mg is administered as a single subcutaneous injection every month. The injected solution forms a solid medicinal product delivery depot and provides continuous release of leuprorelin acetate for one month.
ELIGARD 22.5 mg is administered as a single subcutaneous injection every three months. The injected solution forms a solid medicinal product delivery depot and provides continuous release of leuprorelin acetate over a three-month period.
ELIGARD 45 mg is administered as a single subcutaneous injection every six months. The injected solution forms a solid medicinal product delivery depot and provides continuous release of leuprorelin acetate over a six-month period.
As a rule, therapy of advanced prostate cancer with ELIGARD entails long-term treatment and therapy should not be discontinued when remission or improvement occurs.
Response to ELIGARD should be monitored by clinical parameters and by measuring prostate specific antigen (PSA) serum levels. Clinical studies have shown that testosterone levels increased during the first 3 days of treatment in the majority of non-orchiectomised patients and then decreased to below medical castration levels within 3 - 4 weeks. Once attained, castrate levels were maintained as long as medicinal product therapy continued (<1% testosterone breakthroughs). In case the patient's response appears to be sub-optimal, it should be confirmed that serum testosterone levels have reached or are remaining at castrate levels. As lack of efficacy may result from incorrect preparation, reconstitution, or administration, testosterone levels should be evaluated in cases of suspected or known handling errors (see Precautions).
Paediatric population: The safety and efficacy in children aged 0 to 18 years have not been established (see also Contraindications).
Specific Patient Populations: No clinical studies were performed in patients with either liver or kidney impairment.
Method of Administration: ELIGARD should be prepared, reconstituted and administered only by healthcare professionals who are familiar with these procedures. Instructions for reconstitution and administration must be strictly followed (see Precautions and Special precautions for disposal and other handling under Cautions for Usage). If the product is not prepared appropriately, it should not be administered.
The contents of the two pre-filled sterile syringes must be mixed immediately prior to administration of ELIGARD by subcutaneous injection.
Based on data from animal experience, intra-arterial or intravenous injection, respectively, has to be strictly avoided.
As with other medicinal products administered by subcutaneous injection, the injection site should be varied periodically. The specific injection location chosen should be an area with sufficient soft or loose subcutaneous tissue that does not have excessive pigment, nodules, lesions, or hair. In clinical trials, the injection was administered in the upper-or mid-abdominal area. Avoid areas with brawny or fibrous subcutaneous tissue or locations that could be rubbed or compressed (e.g. with a belt or clothing waistband).
ELIGARD does not have the potential for abuse, and deliberate overdose is unlikely. There are no reports of abuse or overdose having occurred in clinical practice with leuprorelin acetate, but in the event that excessive exposure becomes a reality, observation and symptomatic supportive treatment are recommended.
ELIGARD is contraindicated in women and in paediatric patients.
Hypersensitivity to leuprorelin acetate, to other GnRH agonists or to any of the excipients listed in Description.
In patients who previously underwent orchiectomy (as with other GnRH agonists, ELIGARD does not result in further decrease of serum testosterone in case of surgical castration).
As sole treatment in prostate cancer patients with spinal cord compression or evidence of spinal metastases (see also Precautions).
Correct reconstitution: Cases of handling errors which can occur during any step of the preparation process, and which could potentially result in lack of efficacy have been reported. Instructions for reconstitution and administration must be strictly followed (see Special precautions for disposal and other handling under Cautions for Usage). In cases of suspected or known handling error, patients should be monitored appropriately (see Dosage & Administration).
Androgen deprivation therapy may prolong the QT interval: In patients with a history of or risk factors for QT prolongation and in patients receiving concomitant medicinal products that might prolong the QT interval (see Interactions) physicians should assess the benefit risk ratio including the potential for Torsade de pointes prior to initiating ELIGARD. Electrolyte abnormalities should be corrected. Consider periodic monitoring of electrocardiograms and electrolytes.
Cardiovascular diseases: Increased risk of developing myocardial infarction, sudden cardiac death and stroke has been reported in association with the use of GnRH agonists in men. The risk appears low based on the reported odds ratios, and should be evaluated carefully along with cardiovascular risk factors when determining a treatment for patients with prostate cancer. Patients receiving GnRH agonists should be monitored for symptoms and signs suggestive of development of cardiovascular disease and be managed according to current clinical practice.
Transient testosterone flare: Leuprorelin acetate, like other GnRH agonists, causes a transient increase in serum concentrations of testosterone, dihydrotestosterone and acid phosphatase during the first week of treatment. Patients may experience worsening of symptoms or onset of new symptoms, including bone pain, neuropathy, haematuria, or ureteral or bladder outlet obstruction (see Adverse Reactions). These symptoms usually subside on continuation of therapy.
Additional administration of an appropriate antiandrogen should be considered beginning 3 days prior to leuprorelin therapy and continuing for the first two to three weeks of treatment. This has been reported to prevent the sequelae of an initial rise in serum testosterone.
Following surgical castration, ELIGARD does not lead to a further decrease in serum testosterone levels in male patients.
Bone density: Decreased bone density has been reported in the medical literature in men who have had orchiectomy or who have been treated with GnRH agonists (see Adverse Reactions).
Antiandrogen therapy significantly increases the risk for fractures owing to osteoporosis. Only limited data is available on this issue. Fractures owing to osteoporosis were observed in 5% of patients following 22 months of pharmacological androgen deprivation therapy and in 4% of patients following 5 to 10 years of treatment. The risk for fractures owing to osteoporosis is generally higher than the risk for pathological fractures.
Apart from long lasting testosterone deficiency, increased age, smoking and consumption of alcoholic beverages, obesity and insufficient exercise may have an influence on the development of osteoporosis.
Pituitary apoplexy: During post-marketing surveillance, rare cases of pituitary apoplexy (a clinical syndrome secondary to infarction of the pituitary gland) have been reported after the administration of GnRH-agonists, with a majority occurring within 2 weeks of the first dose, and some within the first hour. In these cases, pituitary apoplexy was presented as sudden headache, vomiting, visual changes, ophthalmoplegia, altered mental status, and sometimes cardiovascular collapse. Immediate medical attention is required.
Hyperglycemia and diabetes: Hyperglycemia and an increased risk of developing diabetes have been reported in men receiving GnRH agonists. Hyperglycemia may represent development of diabetes mellitus or worsening of glycemic control in patients with diabetes. Monitor blood glucose and/or glycosylated hemoglobin (HbA1c) periodically in patients receiving a GnRH agonist and manage with current practice for treatment of hyperglycemia or diabetes.
Convulsions: Post marketing reports of convulsions have been observed in patients on leuprorelin acetate therapy with or without a history of predisposing factors. Convulsions are to be managed according to the current clinical practice.
Other events: Cases of ureteral obstruction and spinal cord compression, which may contribute to paralysis with or without fatal complications, have been reported with GnRH agonists. If spinal cord compression or renal impairment develops, standard treatment of these complications should be instituted.
Patients with vertebral and/or brain metastases as well as patients with urinary tract obstruction should be closely monitored during the first few weeks of therapy.
Effects on ability to drive and use machines: No studies on the effects of ELIGARD on the ability to drive and use machines have been performed.
The ability to drive and operate machines may be impaired due to fatigue, dizziness and visual disturbances being possible side effects of treatment or resulting from the underlying disease.
Not applicable as ELIGARD is contraindicated in women. Expected hormonal changes that occur with Eligard treatment increase the risk for pregnancy loss. In non-clinical studies in rats, major fetal abnormalities were observed after administration of leuprorelin acetate throughout gestation. There were increased fetal mortality and decreased fetal weights in rats and rabbits. The effects of fetal mortality are expected consequences of the alterations in hormonal levels brought about by this drug. The possibility exists that spontaneous abortion may occur. It is not known whether leuprorelin acetate is excreted into human milk.
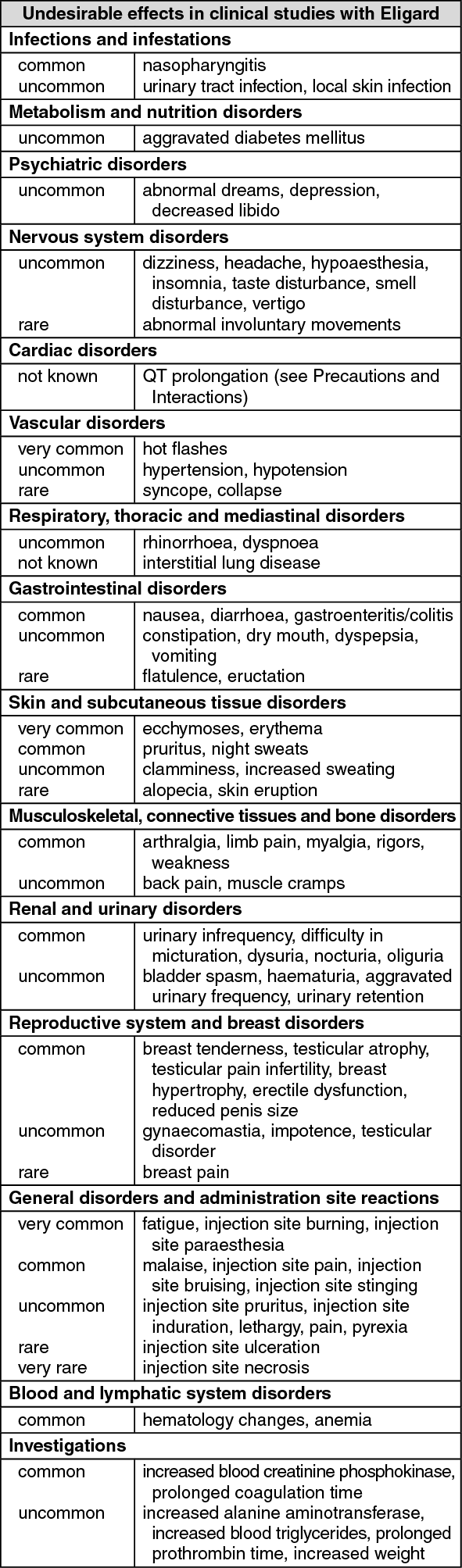
Adverse reactions seen with ELIGARD are mainly subject to the specific pharmacological action of leuprorelin acetate, namely increases and decreases in certain hormone levels. The most commonly reported adverse reactions are hot flashes, malaise, nausea and fatigue and transient local irritation at the site of injection. Mild or moderate hot flashes occur in approximately 58% of patients.
Tabulated list of adverse reactions: The following adverse events were reported during clinical trials with ELIGARD in patients with advanced prostate carcinoma. Adverse events are classified, by frequency, as very common (≥1/10), common (≥1/100, <1/10), uncommon (≥1/1,000, <1/100), rare (≥1/10,000, <1/1,000), and very rare (<1/10,000), not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Other adverse events which have been reported in general to occur with leuprorelin acetate treatment include peripheral oedema, pulmonary embolism, palpitations, myalgia, muscle weakness, an alteration in the skin sensation, chills, rash, amnesia and visual disturbances. Muscular atrophy has been observed with long term use of products in this class. Infarction of pre-existing pituitary apoplexy has been reported rarely after administration of both short and long acting GnRH agonists. There have been rare reports of thrombocytopenia and leucopenia. Changes in glucose tolerance have been reported.
Convulsions have been reported after GnRH agonist analogue administration (see Precautions).
Local adverse events reported after injection of ELIGARD are similar to the local adverse events associated with similar subcutaneously injected products. Generally, these localised adverse events following subcutaneous injection are mild and described as being of brief duration.
Anaphylactic/anaphylactoid reactions have been reported after GnRH agonist analogue administration.
Changes in Bone Density: Decreased bone density has been reported in the medical literature in men who have had orchiectomy or who have been treated with a GnRH analogue. It can be anticipated that long periods of treatment with leuprorelin may show increasing signs of osteoporosis. Regarding the increased risk for fractures owing to osteoporosis (see Precautions).
Exacerbation of signs and symptoms of the disease: Treatment with leuprorelin acetate can cause exacerbations of signs and symptoms of the disease during the first few weeks. If conditions such as vertebral metastases and/or urinary obstruction or haematuria are aggravated, neurological problems such as weakness and/or paraesthesia of the lower limbs or worsening of urinary symptoms may occur.
No pharmacokinetic drug-drug interaction studies have been performed with ELIGARD. There have been no reports of any interactions of leuprorelin acetate with other medicinal products.
Since androgen deprivation treatment may prolong the QT interval, the concomitant use of ELIGARD with medicinal products known to prolong the QT interval or medicinal products able to induce Torsade de pointes such as Class IA (e.g., quinidine, disopyramide, procainamide) or Class III (e.g., amiodarone, sotalol, dofetilide, ibutilide) antiarrhythmic medicinal products, methadone, moxifloxacin, antipsychotics, etc. should be carefully evaluated (see Precautions).
Incompatibilities: The leuprorelin present in syringe B must only be mixed with the solvent in syringe A and must not be mixed with other medicinal products.
Special precautions for disposal and other handling: Allow the product to come to room temperature by removing from the refrigerator approximately 30 minutes prior to use.
Prepare the patient for injection first, followed by the preparation of the product, using the instructions as follows. If the product is not prepared using the proper technique, it should not be administered, as lack of clinical efficacy may occur due to incorrect reconstitution of the product.
Step 1: Open both trays (tear off the foil from the corner which can be recognized by a small bubble) and empty the contents onto a clean field (two trays containing Syringe A and Syringe B). Discard the desiccant pouches.
Step 2: Pull out and do not unscrew the blue coloured short plunger rod together with the attached grey stopper from Syringe B and discard. Do not attempt to mix the product with two stoppers in place.
Step 3: Gently screw the Syringe B white plunger rod to the remaining grey stopper in Syringe B.
Step 4: Remove the grey rubber plug from Syringe B and put down the Syringe.
Step 5: Hold Syringe A in a vertical position to ensure no liquid leaks out and unscrew the clear cap from Syringe A.
Step 6: Join the two syringes together by pushing in and twisting Syringe B onto Syringe A until secure. Do not over tighten.
Step 7: Flip the connected unit over and continue to hold the syringes vertically with Syringe B on the bottom while injecting the liquid contents of Syringe A into Syringe B containing the powder (leuproreline acetate).
Step 8: Thoroughly mix the product by gently pushing the contents of both syringes back and forth between syringes (60 times in total, which takes approximately 60 seconds) in a horizontal position to obtain a homogenous, viscous solution. Do not bend the syringe system (note that this may cause leakage as it may partially unscrew the syringes).
When thoroughly mixed, the viscous solution will appear with a colour in the range of colourless to white to pale yellow (which could include shades of white to pale yellow).
Important: After mixing proceed with the next step immediately as the product gets more viscous over time. Do not refrigerate the mixed product.
Note: Product must be mixed as described; shaking WILL NOT provide adequate mixing of the product.
Step 9: Hold the syringes vertically with Syringe B on the bottom. The syringes should remain securely coupled. Draw the entire mixed product into Syringe B (wide syringe) by pushing down the Syringe A plunger and slightly withdrawing the Syringe B plunger.
Step 10: Twist off Syringe A while continuing to push down on the Syringe A plunger. Ensure that no product leaks out as the needle will then not secure properly when attached.
Note: one large or a few small air bubbles may remain in the formulation - this is acceptable. Do not purge the air bubbles from Syringe B at this stage as product may be lost.
Step 11: Hold Syringe B upright and hold back the white plunger to prevent loss of the product.
Open pack of the safety needle by peeling back paper tab and take out safety needle. Do not remove the hinged safety shield.
Secure the safety needle to Syringe B by holding the syringe and gently turning the needle clockwise with approximately a three-quarter turn until the needle is secure.
Do not over tighten as this may cause cracking of the needle hub resulting in leakage of the product during injection.
Should the needle hub crack, appear to be damaged, or have any leakage, the product should not be used. The damaged needle should not be substituted/replaced and the product should not be injected.
The entire product should be disposed of securely.
In the event of damage to the needle hub, a new replacement product should be used.
Step 12: Move the safety shield away from the needle and pull off the protective needle cap prior to administration.
Important: Do not operate the safety needle mechanism before administration.
Step 13: Prior to administration, purge any large air bubbles from Syringe B. Administer the product subcutaneously whilst keeping the safety shield away from the needle. Ensure that the full amount of the product in Syringe B is injected.
Step 14: After injection, lock the safety shield using any of the activation methods listed as follows.
1. Closure on a flat surface: Press the safety shield, lever side down, onto a flat surface to cover the needle and lock the shield.
Verify locked position through audible and tactile "click". Locked position will completely cover needle tip.
2. Closure with the thumb: Placing the thumb on safety shield, cover the needle tip and lock the shield.
Verify locked position through audible and tactile "click". Locked position will completely cover needle tip.
Step 15: Once safety shield is locked, immediately dispose of the needle and syringe in an approved sharps container.
Shelf life: 2 years.
Once the product has been removed from the refrigerator, it may be stored in the original packaging at room temperature (below 25°C) for up to four weeks.
After first opening of the tray, the powder and solvent for solution for injection are to be immediately reconstituted and administered to the patient.
Once reconstituted: use immediately, as the viscosity of the solution increases with time.
Store in a refrigerator (2°C - 8°C); in the original package in order to protect from moisture.
This product must be at room temperature prior to injection. Remove from the refrigerator approximately 30 minutes before use. Once outside the refrigerator this product may be stored in its original packaging at room temperature (below 25°C) for up to four weeks.
L02AE02 - leuprorelin ; Belongs to the class of gonadotropin releasing hormone analogues. Used in endocrine therapy.
Eligard powd for inj 22.5 mg
(+ solvent) 1's
Eligard powd for inj 45 mg
(+ solvent) 1's
Eligard powd for inj 7.5 mg
(+ solvent) 1's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image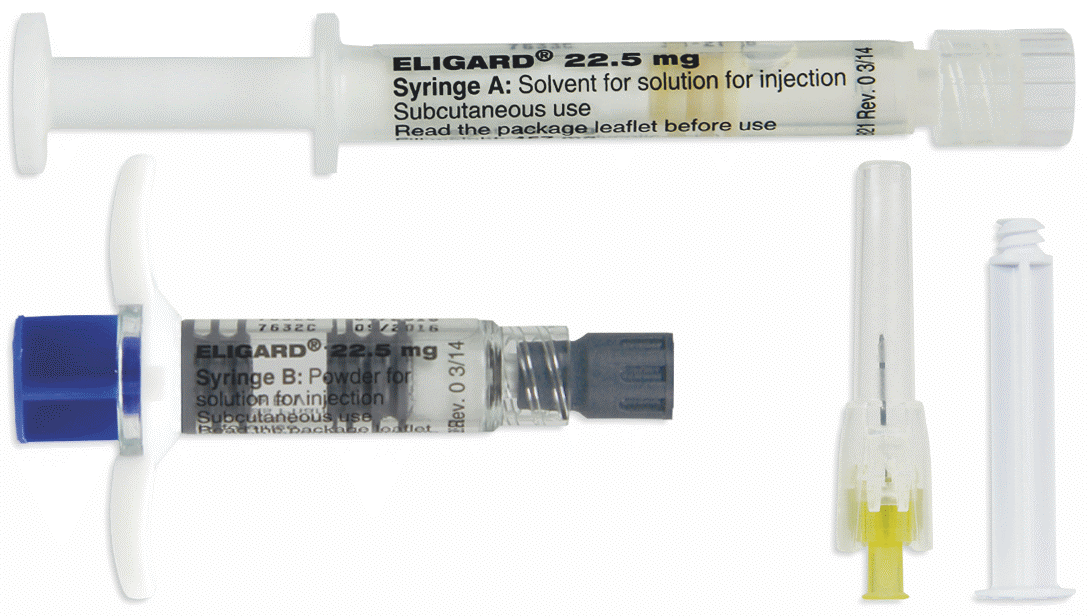


 Sign Out
Sign Out
