Each tablet contains lisinopril (as the dihydrate) 5, 10 or 20 mg, respectively.
Lisinopril is an inhibitor of the angiotensin-converting enzyme (ACE) and inhibits the formation of angiotensin II, a powerful vasoconstrictor. Lisinopril modulates a specific physiological mechanism, the renin-angiotensin-aldosterone system, which plays a significant role in the regulation of blood pressure. Its onset of action begins within 2 hrs following oral administration, achieves its peak effect 4-6 hrs after an oral dose and its effects continue for at least 24 hrs after a single daily dose. Data indicate no loss of effect during long-term therapy. Rebound hypertension does not occur after abrupt cessation of treatment with ACE inhibitors.
Congestive heart failure patients treated with lisinopril benefit particularly from reduction in preload and afterload of the heart, with an increase in cardiac output, without reflex tachycardia.
Lisinopril is not significantly metabolized by the liver, has negligible plasma protein-binding and is excreted unchanged in the urine. Lisinopril minimizes the development of thiazide-induced hypokalaemia and hyperuricaemia.
Treatment of essential hypertension and renovascular hypertension.
As monotherapy or in combination with other classes of antihypertensive agents.
Treatment of congestive heart failure in patients not controlled adequately by digitalis and diuretic therapy.
Essential Hypertension: Usual Recommended Starting Dose: 10 mg. Usual Effective Maintenance Dosage: 20 mg administered in a single daily dose. Dosage should be adjusted according to blood pressure response. The maximum dosage is 80 mg/day.
A lower starting dose is required in the presence of renal impairment in patients whom diuretic therapy cannot be discontinued, patients who are volume- and/or salt-depleted for any reason, and in patients with renovascular hypertension.
Diuretic-Treated Patients: Symptomatic hypotension may occur following initiation of therapy with Dapril, this is more likely in patients who are being treated currently with diuretics. Caution is recommended, therefore, since these patients may be volume- and/or salt-depleted. The diuretic should be discontinued 2-3 days before beginning therapy with Dapril (see Precautions). In hypertensive patients whom the diuretic cannot be discontinued, therapy with Dapril should be initiated with a 5-mg dose. The subsequent dosage of Dapril should be adjusted according to blood pressure response. If required, diuretic therapy may be resumed.
Renovascular Hypertension: Some patients with renovascular hypertension, especially those with bilateral renal artery stenosis or stenosis of the artery to a solitary kidney, may develop an exaggerated response to the 1st dose of Dapril. Therefore, a lower starting dose of 2.5 or 5 mg is recommended. Thereafter, the dosage may be adjusted according to the blood pressure response.
Congestive Heart Failure: In patients not adequately controlled by diuretics and/or digitalis, Dapril may be added in a starting dose of 2.5 mg once daily. The usual effective dosage range is 5-20 mg.
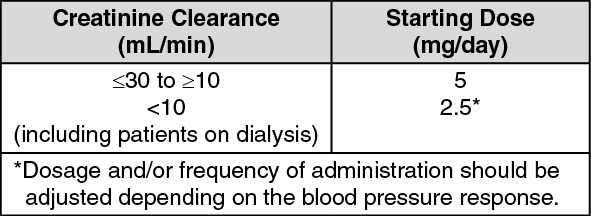
Renal Impairment: Dosage Adjustment: Dosage in patients with renal impairment should be based on creatinine clearance as outlined in the table. (See Table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
*Dosage and/or frequency of administration should be adjusted depending on the blood pressure response.
The dosage may be titrated upward until blood pressure is controlled or to a maximum of 40 mg daily.
Administration: Since absorption of Dapril is not affected by food, the tablets may be administered before, during or after meals. Dapril should be administered as a single daily dose.
There are no data on overdosage in humans. The most likely manifestation of overdosage would be hypotension, for which the usual treatment would be IV infusion of normal saline solution. Dapril can be removed by haemodialysis.
Hypersensitivity to any component of Dapril.
The concomitant use of Dapril with aliskiren-containing products is contraindicated in patients with diabetes mellitus or renal impairment [glomerular filtration rate (GFR) <60 mL/min/1.73 m2] (see Interactions).
Dual Blockade of the Renin-Angiotensin-Aldosterone System (RAAS): There is evidence that the concomitant use of angiotensin-converting enzyme angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers or aliskiren increases the risk of hypotension, hyperkalaemia and decreased renal function (including acute renal failure). Dual blockade of RAAS through the combined use of ACE inhibitors, angiotensin II receptor blockers or aliskiren is therefore not recommended (see Interactions).
If dual blockade therapy is considered absolutely necessary, this should only occur under specialist supervision and subject to frequent close monitoring of renal function, electrolytes and blood pressure.
Angiotensin-converting enzyme-inhibitors and angiotensin II receptor blockers should not be used concomitantly in patients with diabetic nephropathy.
Symptomatic Hypotension: Symptomatic hypotension was seen rarely in uncomplicated hypertensive patients. In hypertensive patients receiving Dapril, hypotension is more likely to occur if the patient has been volume-depleted eg, by diuretic therapy, dietary salt restriction, dialysis, diarrhoea or vomiting (see Side Effects).
In patients with congestive heart failure, with or without associated renal insufficiency, symptomatic hypotension has been observed. This is most likely to occur in those patients with more severe degrees of heart failure, as reflected by the use of high doses of loop diuretics, hyponatremia or functional renal impairment. In these patients, therapy should be started under medical supervision and the patients should be monitored closely whenever the dose of Dapril and/or diuretic is adjusted. If hypotension occurs, the patient should be placed in the supine position and, if necessary, should receive an IV infusion of normal saline.
A transient hypotensive response is not a contraindication to further doses, which can be given usually without difficulty once the blood pressure has increased after volume expansion.
In some patients with congestive heart failure who have normal or low blood pressure, additional lowering of systemic blood pressure may occur with Dapril. This effect is anticipated and is not usually a reason to discontinue treatment. If hypotension becomes symptomatic, a reduction of dose or discontinuation of Dapril may be necessary.
Renal Function Impairment: In patients with congestive heart failure, hypotension following the initiation of therapy with ACE inhibitors may lead to some further impairment in renal function. Acute renal failure, usually reversible, has been reported in this situation.
In some patients with bilateral renal artery stenosis or stenosis of the artery to a solitary kidney, who have been treated with ACE inhibitors, increases of blood urea and serum creatinine, reversible upon discontinuation of therapy have been seen. This is especially likely in patients with renal insufficiency.
Some hypertensive patients with no apparent preexisting renal vascular disease have developed increases in blood urea and serum creatinine, usually minor and transient, especially when Dapril has been given concomitantly with a diuretic.
This is more likely to occur in patients with preexisting renal impairment. Dosage reduction of Dapril and/or discontinuation of the diuretic may be required.
Hypersensitivity/Angioneurotic Oedema: Angioneurotic oedema of the face, extremities, lips, tongue, glottis and/or larynx has been reported rarely in patients treated with ACE inhibitors, including Dapril. In such cases, Dapril should be discontinued promptly and the patient observed carefully until the swelling disappears. In those instances where swelling has been confined to the face and lips, the condition generally resolved without treatment, although antihistamines have been useful in relieving symptoms.
Angioneurotic oedema associated with laryngeal oedema may be fatal. Where there is involvement of the tongue, glottis and larynx, likely to cause airway obstruction, SC adrenaline solution 1:1000 (0.3-0.5 mL) should be administered promptly, and other appropriate therapy instituted.
Surgery/Anaesthesia: In patients undergoing major surgery or during anaesthesia with agents that produce hypotension, Dapril may block angiotensin II formation secondary to compensatory rennin release. If hypotension occurs and is considered to be due to this mechanism, it can be corrected by volume expansion.
Further Information: Where Dapril replaces a β-adrenoceptor blocking agent, the β-adrenoceptor blocker should be withdrawn gradually; the dose should be titrated down after commencing Dapril therapy.
Use in pregnancy: When used in pregnancy during the 2nd and 3rd trimesters, ACE inhibitors can cause injury and even death to the developing foetus. When pregnancy is detected, Dapril should be discontinued as soon as possible.
Use in lactation: It is not known whether Dapril is secreted in human milk. Because many drugs are secreted in human milk, caution should be exercised if Dapril is given to a nursing mother.
Use in children: Safety and effectiveness of Dapril in children have not been established.
Use in the elderly: In clinical studies, there was no age-related change in the efficacy or safety profile of Dapril. When advanced age is associated with decrease in renal function, however, the guidelines set out in the table (see Dosage & Administration) should be used to determine the starting dose of Dapril. Thereafter, the dosage should be adjusted according to the blood pressure response.
Use in pregnancy: When used in pregnancy during the 2nd and 3rd trimesters, ACE inhibitors can cause injury and even death to the developing foetus. When pregnancy is detected, Dapril should be discontinued as soon as possible.
Use in lactation: It is not known whether Dapril is secreted in human milk. Because many drugs are secreted in human milk, caution should be exercised if Dapril is given to a nursing mother.
Dapril has been found in controlled clinical trials to be generally well tolerated. For the most part, side effects were mild and transient in nature.
The most frequent clinical side effects of Dapril in controlled trials were: Dizziness (6.5%), headache (5.4%), diarrhoea (3.8%) and fatigue (2.9%).
Other side effects occurring less frequently, but in >1% of patients treated with Dapril, in controlled clinical trials were: Cough, nausea, rash, hypotension, orthostatic effects, palpitation, chest pain, asthenia.
Hypersensitivity/Angioneurotic Oedema: Angioneurotic oedema of the face, extremities, lips, tongue, glottis and/or larynx has been reported rarely (see Precautions).
Laboratory Test Findings: Clinically important changes in standard laboratory parameters were rarely associated with administration of Dapril. Increases in blood urea and serum creatinine, usually reversible upon discontinuation of Dapril have been seen.
Small decreases in haemoglobin and haematocrit, rarely of clinical importance unless another cause of anaemia coexisted, have occurred. Plasma potassium concentrations >5.7 mEq/L were reported in isolated instances in clinical trials, but were usually transient.
Clinical trial data has shown that dual blockade of the renin-angiotensin-aldosterone system (RAAS) through the combined use of angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers or aliskiren is associated with a higher frequency of adverse events eg, hypotension, hyperkalaemia and decreased renal function (including acute renal failure) compared to the use of a single RAAS-acting agent (see Contraindications and Precautions).
Diuretics: When a diuretic is added to the therapy of a patient receiving Dapril, the antihypertensive effect is usually potentiated.
Patients already on diuretics and especially those in whom diuretic therapy was recently instituted, may occasionally experience an excessive reduction of blood pressure when Dapril is added. The possibility of symptomatic hypotension with Dapril can be minimized by discontinuing the diuretic prior to initiation of treatment with Dapril (see Dosage & Administration and Precautions).
Other Agents: Indomethacin may diminish the antihypertensive efficacy of concomitantly administered Dapril.
Dapril has been used concomitantly with nitrates without evidence of clinically significant adverse interactions.
Serum Potassium: In clinical trials, serum potassium usually remained within normal limits. If Dapril is given with a potassium-losing diuretic, diuretic-induced hypokalaemia may be ameliorated.
Risk factors for the development of hyperkalaemia include renal insufficiency, diabetes mellitus and concomitant use of potassium-sparing diuretics (eg, spironolactone, triamterene or amiloride) or potassium supplements.
The use of potassium supplements or potassium-sparing diuretics particularly in patients with impaired renal function may lead to a significant increase in serum potassium.
If concomitant use of Dapril and any of the previously mentioned agents is deemed appropriate, they should be used with caution and with frequent monitoring of serum potassium.
Store below 25°C in the original blister.
C09AA03 - lisinopril ; Belongs to the class of ACE inhibitors. Used in the treatment of cardiovascular disease.
Dapril tab 10 mg
100 × 10's;3 × 10's
Dapril tab 20 mg
100 × 10's;3 × 10's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
