Pharmacotherapeutic Group: Second generation cephalosporins.
ATC Code: J01DC02.
Pharmacology: Pharmacodynamics: Cefuroxime inhibits cell wall production and are selective inhibitors of peptidoglycan synthesis.
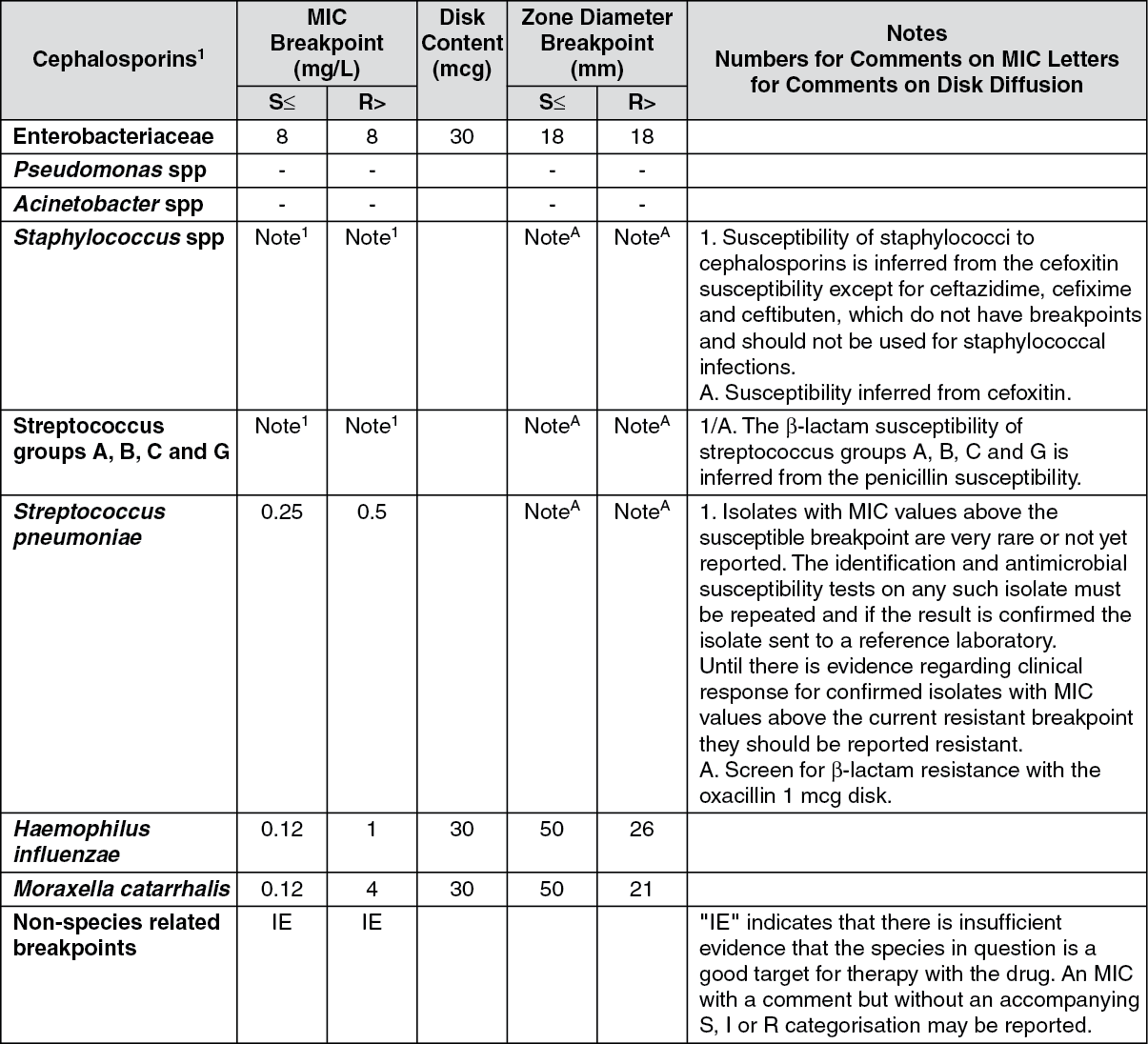
Breakpoints: According to the EUCAST clinical breakpoint table v. 2, valid from January 1, 2012, the following breakpoints have been defined for cefuroxime axetil: See table.
 Click on icon to see table/diagram/image
Pharmacokinetics:
Click on icon to see table/diagram/image
Pharmacokinetics: After oral administration cefuroxime axetil is slowly absorbed from the gastrointestinal tract and rapidly hydrolysed in the intestinal mucosa and blood to release cefuroxime into the circulation.
Optimum absorption occurs when it is administered shortly after a meal.
Peak serum levels (2-3 mg/L for a 125 mg dose, 4-6 mg/L for a 250 mg dose, 5-8 mg/L for a 500 mg dose and 9-14 mg/L for a 1 g dose) occur approximately 2-3 hrs after dosing when taken after food, unlike IV dosing which peaks immediately.
The absorption of cefuroxime from the suspension is more prolonged compared with tablets, leading to later, lower peak serum levels and slightly reduced systemic bioavailability (4-17% less). Post peak levels, the serum half life (t
½) is between 1 hr and 1.5 hrs. Protein-binding has been variously stated as 33-50% depending on the methodology used. Cefuroxime is not metabolized and is excreted by glomerular filtration and tubular secretion.
Concurrent administration of probenecid increases the area under the mean serum concentrations time curve by 50%. Serum levels of cefuroxime are reduced by dialysis.
Microbiology: Susceptibility: Cefuroxime is usually active against the following organisms
in vitro.
Aerobes Gram Negative: Haemophilus influenzae (including ampicillin-resistant strains),
Haemophilus parainfluenzae,
Moraxella (Branhamella) catarrhalis,
Neisseria gonorrhoeae (including penicillinase and non-penicillinase producing strains),
Escherichia coli,
Klebsiella spp,
Proteus mirabilis,
Providencia spp,
Proteus rettgeri.
Aerobes Gram Positive: Staphylococcus aureus and
Staphylococcus epidermidis (including penicillinase producing strains but excluding methicillin resistant strains),
Streptococcus pyogenes (and other β-haemolytic streptococci),
Streptococcus pneumoniae, Streptococcus Group B (
Streptococcus agalactiae).
Anaerobes: Gram-positive and gram-negative cocci (including
Peptococcus and
Peptostreptococcus spp), gram positive bacilli (including
Clostridium spp), gram negative bacilli (including
Bacteroides spp and
Fusobacterium spp),
Propionibacterium spp.
Other Organisms: Borrelia burgdorferi.
The Following Organisms are Not Susceptible to Cefuroxime: Clostridium difficile,
Pseudomonas spp,
Campylobacter spp,
Acinetobacter calcoaceticus,
Listeria monocytogenes, methicillin resistant strains of
Staphylococcus aureus and
Staphylococcus epidermidis,
Legionella spp.
Some Strains of the Following Genera are Not Susceptible to Cefuroxime: Enterococcus (Streptococcus) faecalis,
Morganella morganii,
Proteus vulgaris,
Enterobacter spp,
Citrobacter spp,
Serratia spp,
Bacteroides fragilis.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
