


 Sign Out
Sign Out


Meropenem exerts its bactericidal action by interfering with vital bacterial cell wall synthesis. The ease with which it penetrates bacterial cell walls, its high level of stability to all serine β-lactamases and its marked affinity for the penicillin binding proteins (PBPs) explain the potent bactericidal action of meropenem against a broad spectrum of aerobic and anaerobic bacteria. Minimum bactericidal concentrations (MBC) are commonly the same as the minimum inhibitory concentrations (MIC). For 76% of the bacteria tested, the MBC: MIC ratios were ≤2.
Meropenem is stable in susceptibility tests and these tests can be performed using normal routine methods. In vitro tests show that meropenem acts synergistically with various antibiotics. It has been demonstrated both in vitro and in vivo that meropenem has a post-antibiotic effect.
A single set of meropenem susceptibility criteria are recommended based on pharmacokinetics and correlation of clinical and microbiological outcomes with zone diameter and MIC of the infecting organisms. (See Table 1.)
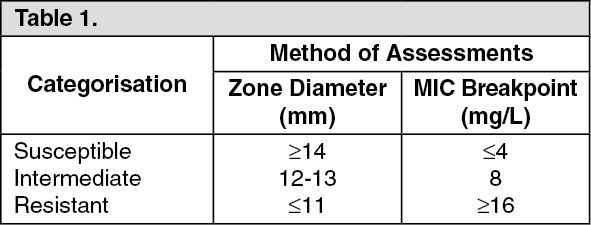 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetic/Pharmacodynamic (PK/PD) Relationship: Similar to other β-lactam antibacterial agents, the time that meropenem concentration exceed the MIC (T>MIC) has been shown to best correlate with efficacy. In preclinical models meropenem demonstrated activity when plasma concentrations exceeded the MIC of the infecting organisms for approximately 40% of the dosing interval. This target has not been established clinically.
Pharmacokinetics: In healthy subjects the mean plasma half-life (t½) is approximately 1 hr; the mean volume of distribution is approximately 0.25 L/kg (11-27 L) and the mean clearance is 287 mL/min at 250 mg falling to 205 mL/min at 2 g. Doses of 500, 1000 and 2000 mg doses infused over 30 min give mean peak plasma concentration (Cmax) values of approximately 23, 49 and 115 mcg/mL respectively, corresponding AUC values were 39.3, 62.3 and 153 mcg·hr/mL. After infusion over 5 min Cmax values are 52 and 112 mcg/mL after 500 and 1000 mg doses respectively. When multiple doses are administered 8-hourly to subjects with normal renal function, accumulation of meropenem does not occur.
A study of 12 patients administered meropenem 1000 mg 8 hourly post-surgically for intra-abdominal infections showed a comparable Cmax and t½ to normal subjects but a greater volume of distribution 27 L.
Distribution: The average plasma protein-binding of meropenem was approximately 2% and was independent of concentration. After rapid administration (≤5 min) the pharmacokinetics are biexponential but this is much less evident after 30 min infusion. Meropenem has been shown to penetrate well into several body fluids and tissues including: Lung, bronchial secretions, bile, cerebrospinal fluid, gynaecological tissues, skin, fascia, muscle and peritoneal exudates.
Metabolism: Meropenem is metabolised by hydrolysis of the β-lactam ring generating a microbiologically inactive metabolite. In vitro meropenem shows reduced susceptibility to hydrolysis by human DHP-I compared to imipenem and there is no requirement to co-administer a DHP-I inhibitor.
Elimination: Meropenem is primarily excreted unchanged by the kidneys; approximately 70% (50-75%) of the dose is excreted unchanged within 12 hrs. A further 28% is recovered as the microbiologically inactive metabolite. Faecal elimination represents only approximately 2% of the dose. The measured renal clearance and the effect of probenecid show that meropenem undergoes both filtration and tubular secretion.
Adults: Pharmacokinetic studies performed in patients have not shown significant pharmacokinetic differences versus healthy subjects with equivalent renal function. A population model developed from data in 79 patients with intra-abdominal infection or pneumonia, showed a dependence of the central volume on weight and the clearance on creatinine clearance (CrCl) and age.
Children: The pharmacokinetics in infants and children with infection at doses of 10, 20 and 40 mg/kg showed Cmax values approximating to those in adults following 500, 1000 and 2000 mg doses, respectively. Comparison showed consistent pharmacokinetics between the doses and t½ similar to those observed in adults in all but the youngest subjects (<6 months t½ 1.6 hrs). The mean meropenem clearance values were 5.8 mL/min/kg (6-12 years), 6.2 mL/min/kg (2-5 years), 5.3 mL/min/kg (6-23 months) and 4.3 mL/min/kg (2-5 months). Approximately 60% of the dose is excreted in urine over 12 hrs as meropenem with a further 12% as metabolite. Meropenem concentrations in the cerebrospinal fluid of children with meningitis are approximately 20% of concurrent plasma levels although there is significant inter-individual variability.
The pharmacokinetics of meropenem in neonates requiring anti-infective treatment showed greater clearance in neonates with higher chronological or gestational age with an overall average t½ of 2.9 hrs. Monte Carlo simulation based on a population PK model showed that a dose regimen of 20 mg/kg 8 hrly achieved 60% T>MIC for P. aeruginosa in 95% of pre-term and 91% of full term neonates.
Elderly: Pharmacokinetic studies in healthy elderly subjects (65-80 years) have shown a reduction in plasma clearance, which correlated with age-associated reduction in CrCl, and a smaller reduction in nonrenal clearance. No dose adjustment is required in elderly patients, except in cases of moderate to severe renal impairment (see Dosage & Administration).
Renal Insufficiency: Renal impairment results in higher plasma area under the concentration-time curve (AUC) and longer t½ for meropenem. There were AUC increases of 2.4-fold in patients with moderate impairment (CrCl 33-74 mL/min), 5-fold in severe impairment (CrCl 4-23 mL/min) and 10-fold in haemodialysis patients (CrCl <2 mL/min) when compared to healthy subjects (CrCl >80 mL/min). The AUC of the microbiologically inactive ring opened metabolite was also considerably increased in patients with renal impairment. Dose adjustment is recommended for patients with moderate and severe renal impairment (see Dosage & Administration).
Meropenem is cleared by haemodialysis with clearance during haemodialysis being approximately 4 times higher than in anuric patients.
Hepatic Insufficiency: A study in patients with alcoholic cirrhosis shows no effect of liver disease on the pharmacokinetics of meropenem after repeated doses.
Toxicology: Preclinical Safety Data: Animal studies indicate that meropenem is well tolerated by the kidney. In animal studies meropenem has shown nephrotoxic effects, only at high dose levels (500 mg/kg).
Effects on the CNS; convulsions in rats and vomiting in dogs, were seen only at high doses (>2000 mg/kg).
For an IV dose the LD50 in rodents is >2000 mg/kg. In repeat dose studies (up to 6 months) only minor effects were seen including a small decrease in red cell parameters and an increase in liver weight in dogs treated with doses of 500 mg/kg.
There was no evidence of mutagenic potential in the 5 tests conducted and no evidence of reproductive and teratogenic toxicity in studies at the highest possible doses in rats and monkeys; the no effect dose level of a (small) reduction in F1 body weight in rat was 120 mg/kg. There was an increased incidence of abortions at 500 mg/kg in a preliminary study in monkeys.
There was no evidence of increased sensitivity to meropenem in juveniles compared to adult animals. The intravenous formulation was well tolerated in animal studies.
The sole metabolite of meropenem had a similar profile of toxicity in animal studies.
Microbiology: Mechanism of Resistance: Bacterial resistance to meropenem may result from: Decreased permeability of the outer membrane of gram-negative bacteria (due to diminished production of porins); reduced affinity of the target PBPs; increased expression of efflux pump components, and production of β-lactamases that can hydrolyse carbapenems.
Localised clusters of infections due to carbapenem-resistant bacteria have been reported in some regions.
There is no target-based cross-resistance between meropenem and agents of the quinolone, aminoglycoside, macrolide and tetracycline classes. However, bacteria may exhibit resistance to >1 class of antibacterials agents when the mechanism involved includes impermeability and/or an efflux pump(s).
Breakpoints: European committee on antimicrobial susceptibility testing (EUCAST) clinical breakpoints for MIC testing are presented in Table 2 (See Table 2).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe susceptibility to meropenem of a given clinical isolate should be determined by standard methods. Interpretations of test results should be made in accordance with local infectious diseases and clinical microbiology guidelines.
The antibacterial spectrum of meropenem includes the following species, based on clinical experience and therapeutic guidelines.
Gram-Positive Aerobes: Enterococcus faecalis (note that E. faecalis can naturally display intermediate susceptibility), Staphylococcus aureus [methicillin-susceptible strains only: Methicillin-resistant staphylococci including methicillin-resistant staphylococcus aureus (MRSA) are resistant to meropenem], Staphylococcus species including Staphylococcus epidermidis [methicillin-susceptible strains only: Methicillin-resistant staphylococci including methicillin-resistant staphylococcus epidermidis (MRSE) are resistant to meropenem], Streptococcus agalactiae (Group B streptococcus), Streptococcus milleri group (S. anginosus, S. constellatus, and S. intermedius), Streptococcus pneumoniae, Streptococcus pyogenes (Group A streptococcus).
Gram-Negative Aerobes: Citrobacter freundii, Citrobacter koseri, Enterobacter aerogenes, Enterobacter cloacae, Escherichia coli, Haemophilus influenzae, Klebsiella oxytoca, Klebsiella pneumoniae, Morganella morganii, Neisseria meningitidis, Proteus mirabilis, Proteus vulgaris, Serratia marcescens.
Anaerobic Bacteria: Clostridium perfringens, Peptoniphilus asaccharolyticus, Peptostreptococcus spp (including P. micros, P anaerobius, P. magnus).
Bacteroides caccae, Bacteroides fragilis group, Prevotella bivia, Prevotella disiens.
Species for Which Acquired Resistance may be a Problem: Gram-Positive Aerobes: Enterococcus faecium (E. faecium can naturally display intermediate susceptibility even without acquired resistance mechanisms; note that in some European countries the frequency of resistance among E. faecium is >50% of isolates).
Species for Which Acquired Resistance may be a Problem: Gram-Negative Aerobes: Acinetobacter species, Burkholderia cepacia, Pseudomonas aeruginosa.
Inherently Resistant Organisms: Gram-negative aerobes.
Stenotrophomonas maltophilia, Legionella species.
Other Inherently Resistant Organisms: Chlamydophila pneumoniae, Chlamydophila psittaci, Coxiella burnetii, Mycoplasma pneumonia.
The published medical microbiology literature describes in vitro meropenem-susceptibilities of many other bacterial species. However the clinical significance of such in vitro findings is uncertain. Advice on the clinical significance of in vitro findings should be obtained from local infectious diseases and clinical microbiology experts and local professional guidelines. Meropenem and imipenem have a similar profile of clinical utility and activity against multiresistant bacteria. However, meropenem is intrinsically more potent against Pseudomonas aeruginosa and may be active in vitro against imipenem-resistant strains.
Meropenem is active in vitro against many strains resistant to other β-lactam antibiotics. This is explained in part by enhanced stability to β-lactamases. Activity in vitro against strains resistant to unrelated classes of antibiotics eg, aminoglycosides or quinolones is common.
The prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent in at least some types of infections is questionable.