Dose-limiting toxicities during therapy are cardiotoxicity and myelosuppression.
Cardiac Effects: Sinus tachycardia, ECG abnormalities, tachyarrhythmias, atrio-ventricular and bundle branch block, asymptomatic reductions in the left ventricular ejection fraction (LVEF), CHF, acute life-threatening arrhythmias during or within few hours after Doxorubicin administration.
Hematologic Effects: Leukopenia, neutropenia, anemia, thrombocytopenia, and hemorrhage.
Gastrointestinal (GI) Effects: Acute nausea and vomiting occurs frequently and may be severe, but this may be alleviated by antiemetic therapy. Mucositis (stomatitis and esophagitis) may occur 5 to 10 days after administration and its effect may be severe leading to ulceration and represents a site of origin for severe infections. A dosage regimen of Doxorubicin given on three successive days results in a higher incidence and severity of mucositis. Stomatitis usually begins as a burning sensation accompanied by erythema of the oral mucosa, which in 2 to 3 days may progress to ulceration, particularly in the sublingual and lateral tongue margins and on the palate. Ulceration is sometimes severe enough to result in difficulty in swallowing, but seldom requires cessation of therapy. Stomatitis is maximal during the second week of therapy and lasts an additional 3 to 7 days. GI toxicity (frequently nausea and vomiting and occasionally anorexia and diarrhea) may occur, usually on the day of drug administration. Ulceration and necrosis of the colon, especially the cecum, may occur leading to bleeding or severe infections which can be fatal. These reactions have been reported in patients with acute myelogenous leukemia treated with a 3-day course of doxorubicin combined with cytarabine. Anorexia, abdominal pain, dehydration, diarrhea, hyperpigmentation, GI tract bleeding, and colitis have been occasionally reported.
Dermatological Effects: Reversible complete alopecia occurs in most cases. Regrowth of hair usually begins 2 to 3 months after doxorubicin is discontinued. Hyperpigmentation of nailbeds, pigmented banding of fingernails, and phalangeal and other dermal creases (primarily in pediatric patients) may occur. Oncholysis, plantar callus formation, and epidermolysis have been reported in patients receiving doxorubicin. Recurrence of skin reaction due to prior radiotherapy has occurred; the reaction occurred from 4 to 7 days after each dose was administered and lasted an average of 7 days thereafter. Rash, itching, photosensitivity, acral erythema, and palmar plantar erythrodysesthesia may occur.
Local Effects: Extravasation produces severe local tissue necrosis, as well as possible cellulitis, vesication, lymphangitis, or painful induration and may result in limitation of mobility to the adjacent joints. Erythematous streaking along the vein proximal to the site of injection has been reported. Intravesical instillation can cause bladder and urethral irritation, hematuria, and hemorrhagic cystitis.
Hypersensitivity: Fever, chills, rash, or itching and urticaria have been reported occasionally. Anaphylaxis may occur. A case of apparent cross sensitivity to lincomycin has been reported.
Vascular Effects: Phlebosclerosis has been reported especially when a single vein is used or small veins are used for repeated administration. Facial flushing may occur if the injection is given too rapidly. Phlebitis, thrombophlebitis and thromboembolism can occur.
Neurological Effects: Peripheral neurotoxicity in the form of local-regional sensory and/or motor disturbance has been reported in patients treated with intra-arterial Doxorubicin, mostly in combination with cisplatin. Concomitant use of doxorubicin with cisplatin or vincristine also reported seizures and coma.
Endocrine/Metabolic Effects: Hyperuricemia may occur due to tumor lysis syndrome and serum uric acid concentrations should be monitored. Amenorrhea, hot flushes, oligospermia, azoospermia, and weight gain have been reported.
Ocular Effects: Conjunctivitis, keratitis and lacrimation occur but rarely.
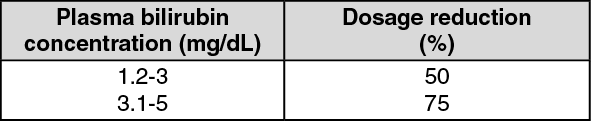
Hepatic Effects: Changes in transaminase level have been reported. Hepatitis and hepatocellular damage have been reported in patients receiving doxorubicin as part of combination therapy. A characteristic hepatotoxicity can also be produced by the combination of radiotherapy with doxorubicin.
Urological Effects: Pain, hemorrhage and occasionally decreased bladder capacity upon instillation, reddish urine for 1 to 2 days after administration.
Others: Malaise/asthenia, shock.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image for soln 10 mg02b68091-c7a0-4ec4-ade6-a79901071e3b.GIF)
 for soln 50 mg8b228552-8e65-4321-9e0e-a79901071e49.GIF)

 Sign Out
Sign Out
