Dosage with single and daily doses: An ECG (50 mm/s) should be recorded before and 1 and 3 weeks after commencing treatment and the Bazett frequency-corrected QT time (QTc) determined manually. Such an ECG should also be recorded before and 2 weeks after any subsequent dose increase. Further ECG check-ups should then take place at least once a year.
Treatment must be avoided or discontinued in patients who show baseline QTc values above 420 ms, an increase of more than 60 ms during treatment with Amantadine Sulphate (PK-Merz)100 mg film-coated tablets, or a QTc in excess of 480 ms during treatment with Amantadine Sulphate (PK-Merz) 100 mg film-coated tablets, and in patients who show discernible U waves.
By following the previously mentioned precautions and taking into account the listed contraindications, the very rare, but life-threatening, side effect torsade de pointes ventricular tachycardia can be prevented.
Treatment of patients with parkinsonian syndromes and drug-related movement disturbances should normally be introduced gradually, with the dose guided by the therapeutic effect.
Treatment should be commenced at a dose of 1 Amantadine Sulphate (PK-Merz) 100 mg film-coated tablet (equivalent to 100 mg amantadine sulphate per day) once daily for the first 4 to 7 days, followed by a once-weekly increase in daily dose of one tablet until the maintenance dose is reached.
The usual effective dose is 1 to 3 Amantadine Sulphate (PK-Merz) 100 mg film-coated tablets twice daily (equivalent to 200–600 mg amantadine sulphate per day).
In elderly patients, particularly those with states of agitation and confusion or delirious syndromes, treatment should be commenced at a lower dose.
If given in combination with other antiparkinsonian drugs, the dosage should be individually adjusted.
In patients previously treated with amantadine infusion solution, a higher starting dose can be chosen.
In the event of an acute worsening of parkinsonian symptoms in the sense of an akinetic crisis, amantadine infusion treatment should be administered.
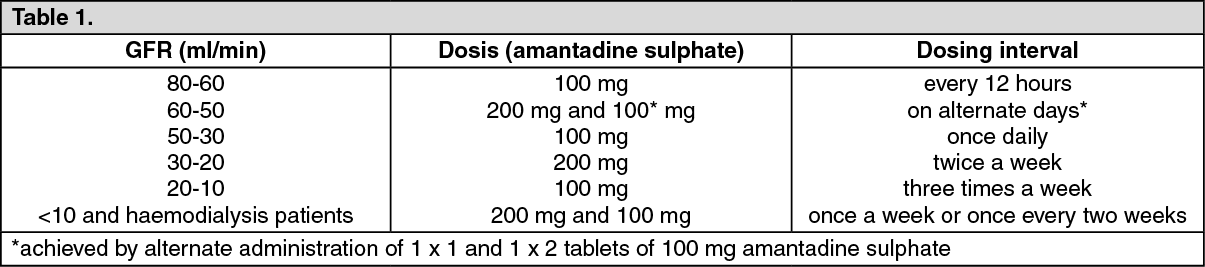
Dosage in patients with renal impairment: In patients with renal impairment the dosage must be tailored according to the extent of the decrease in renal clearance (measured as the glomerular filtration rate: GFR), as shown in the following table: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The glomerular filtration rate (GFR) can be estimated according to the following approximation: See Equation.
Click on icon to see table/diagram/image
The creatinine clearance calculated according to this expression applies to men only (the corresponding value in women is approximately 85 % of this value) and can be equated to the inulin clearance for determination of the GFR (120 ml/min in adults). Amantadine is dialysed only slightly (approx. 5 %).
Method and duration of administration: The film-coated tablets are to be taken with a little liquid, preferably in the morning and afternoon. The last daily dose should not be taken later than 4 p.m.
The duration of treatment is guided by the nature and severity of the disease course and is determined by the medical doctor giving treatment. Patients must not discontinue treatment unilaterally.
Abrupt discontinuation of Amantadine Sulphate (PK-Merz) 100 mg film-coated tablets must be avoided, as patients with Parkinson's disease may otherwise experience a severe intensification in extrapyramidal symptoms, sometimes including akinetic crisis, and withdrawal effects sometimes including delirium can occur.
Children: There has been insufficient experience in children.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image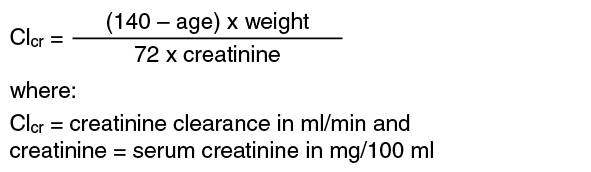 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
