Posology: see Tables 2 and 3.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Paediatric population: The safety and efficacy of Ceftazidime administered as continuous infusion to neonates and infants ≤ 2 months has not been established.
Elderly: In view of age related reduced clearance of Ceftazidime in elderly patients, the daily dose should not normally exceed 3 g in those over 80 years of age.
Hepatic impairment: Available data do not indicate the need for dose adjustment in mild or moderate liver function impairment. There are no study data in patients with severe hepatic impairment. Close clinical monitoring for safety and efficacy is advised.
Renal impairment: Ceftazidime is excreted unchanged by the kidneys. Therefore, in patients with impaired renal function, the dosage should be reduced.
An initial loading dose of 1 g should be given. Maintenance doses should be based on creatinine clearance: see Table 4.
Click on icon to see table/diagram/image
In patients with severe infections the unit dose should be increased by 50% or the dosing frequency increased.
In children the creatinine clearance should be adjusted for body surface area or lean body mass. (See Table 5.)
Click on icon to see table/diagram/image
Close clinical monitoring for safety and efficacy is advised. (See Table 6.)
Click on icon to see table/diagram/image
Caution is advised in dose selection. Close clinical monitoring for safety and efficacy is advised.
Children < 40 kg: The safety and effectiveness of Ceftazidime administered as continuous infusion in renally impaired children < 40 kg has not been established. Close clinical monitoring for safety and efficacy is advised.
If continuous infusion is used in children with renal impairment, the creatinine clearance should be adjusted for body surface area or lean body mass.
Haemodialysis: The serum half-life during haemodialysis ranges from 3 to 5 h.
Following each haemodialysis period, the maintenance dose of ceftazidime recommended in the table as follows should be repeated.
Peritoneal dialysis: Ceftazidime may be used in peritoneal dialysis and continuous ambulatory peritoneal dialysis (CAPD).
In addition to intravenous use, ceftazidime can be incorporated into the dialysis fluid (usually 125 to 250 mg for 2 litres of dialysis solution).
For patients in renal failure on continuous arterio-venous haemodialysis or high-flux haemofiltration in intensive therapy units: 1 g daily either as a single dose or in divided doses. For low-flux haemofiltration, follow the dose recommended under renal impairment.
For patients on veno-venous haemofiltration and veno-venous haemodialysis, follow the dosage recommendations in tables 7 & 8 as follows. (See Tables 7 and 8.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Method of administration: The dose depends on the severity, susceptibility, site and type of infection and on the age and renal function of the patient.
Ceftazidime should be administered by intravenous injection or infusion, or by deep intramuscular injection. Recommended intramuscular injection sites are the upper outer quadrant of the gluteus maximus or lateral part of the thigh. Ceftazidime solutions may be given directly into the vein or introduced into the tubing of a giving set if the patient is receiving parenteral fluids.
The standard recommended route of administration is by intravenous intermittent injection or intravenous continuous infusion. Intramuscular administration should only be considered when the intravenous route is not possible or less appropriate for the patient.
Directions for Reconstitution: For single use. Discard any unused contents.
Instructions for reconstitution: See table for addition volumes and solution concentrations, which may be useful when fractional doses are required.
Preparation of Solution: see Table 9.
Click on icon to see table/diagram/image
Solutions range from light yellow to amber depending on concentration, diluent and storage conditions used.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image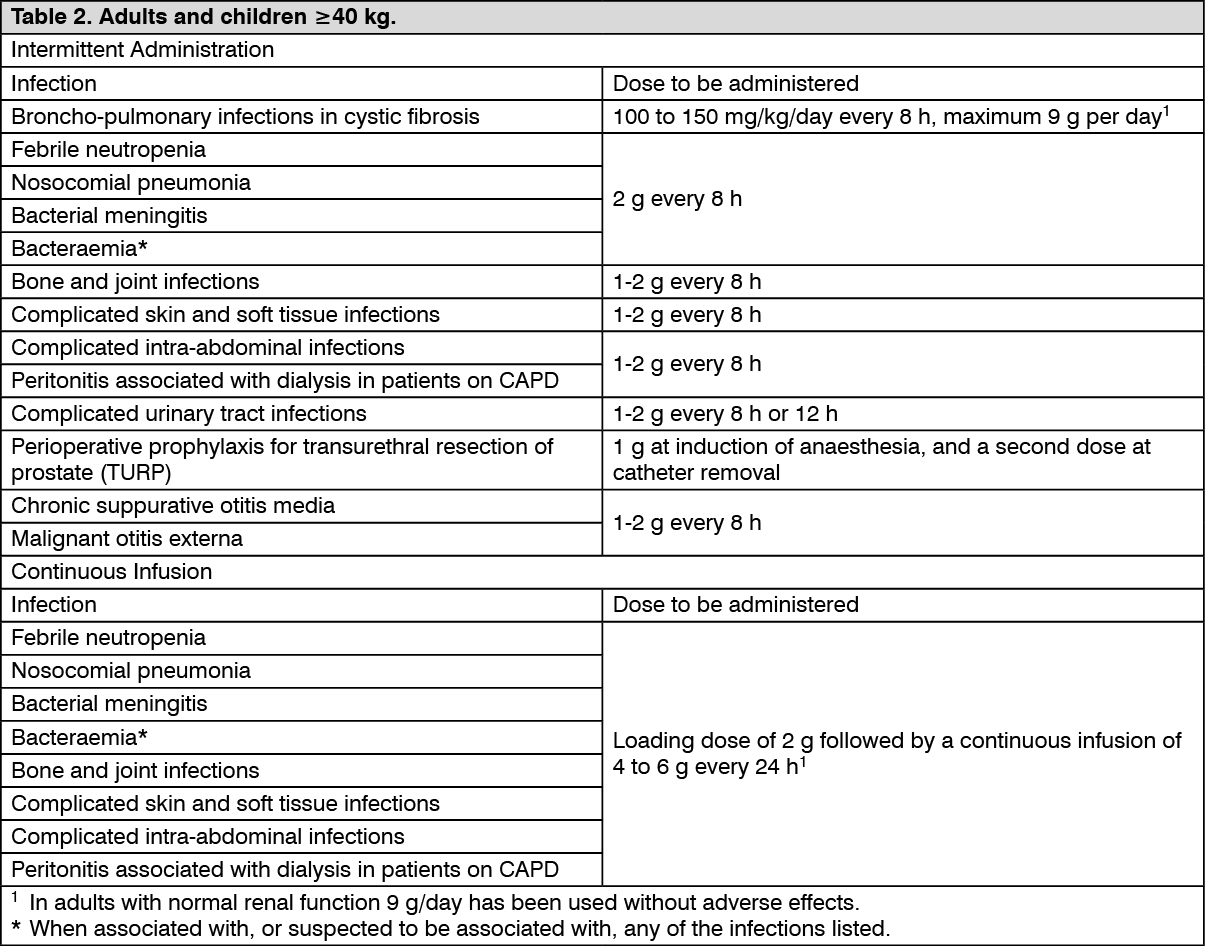 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image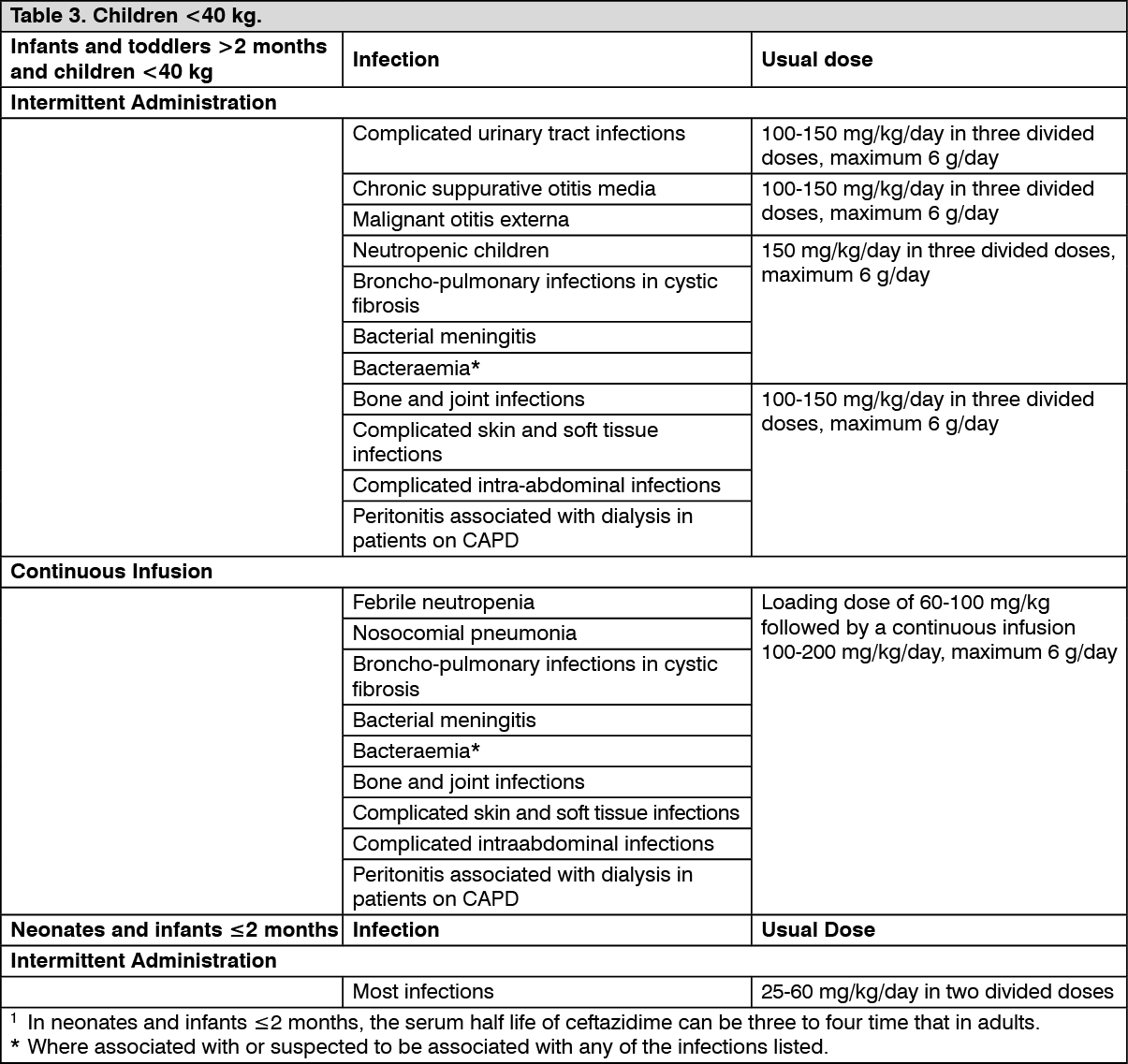 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image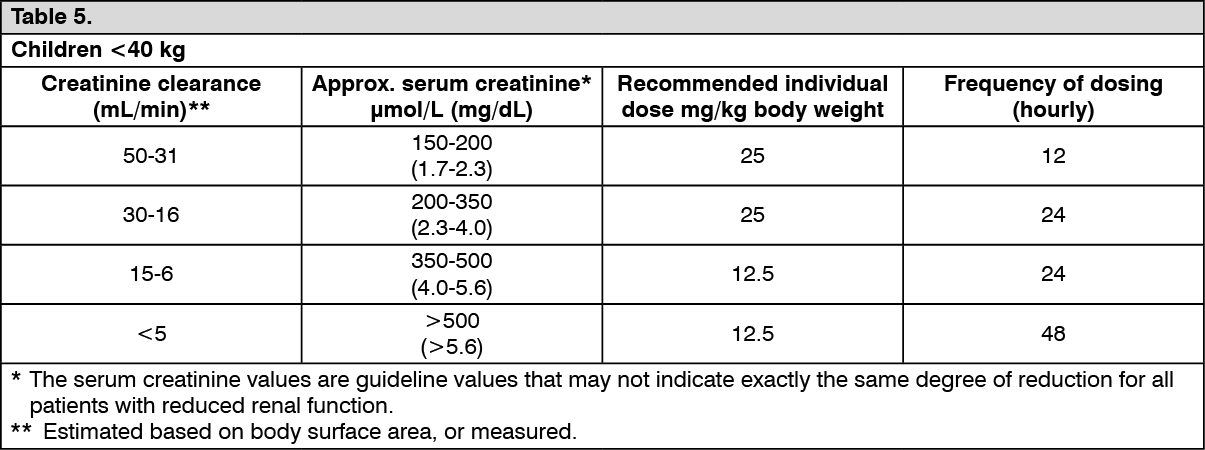 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image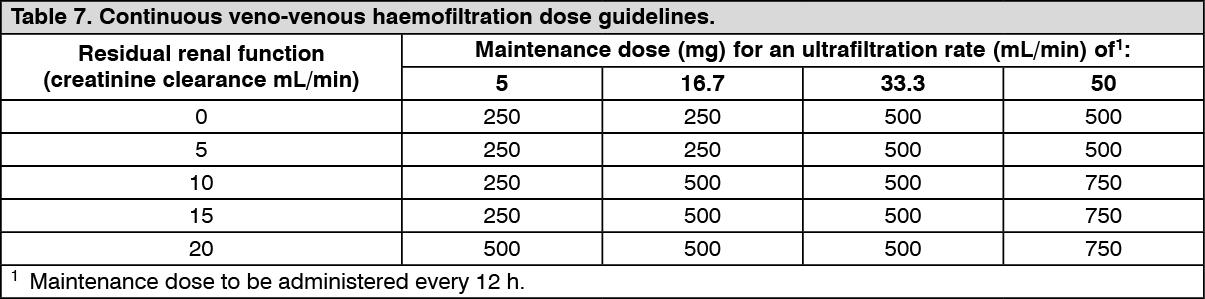 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image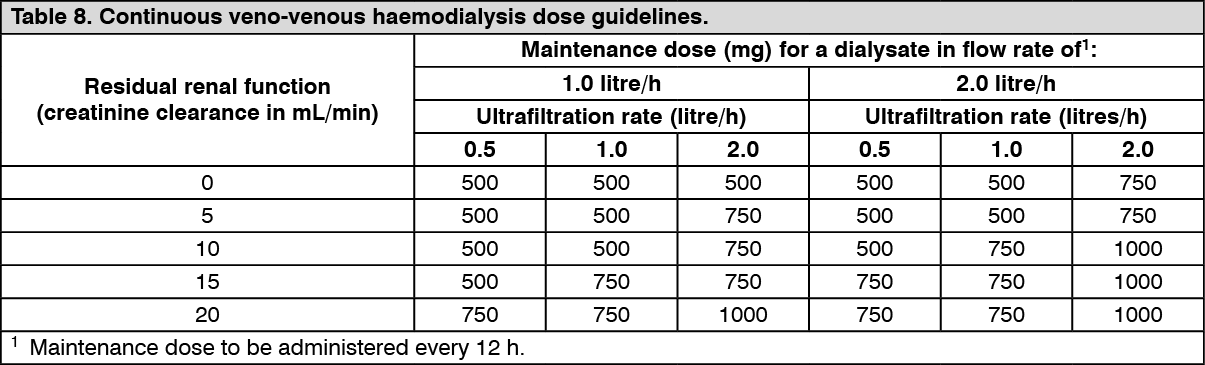 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image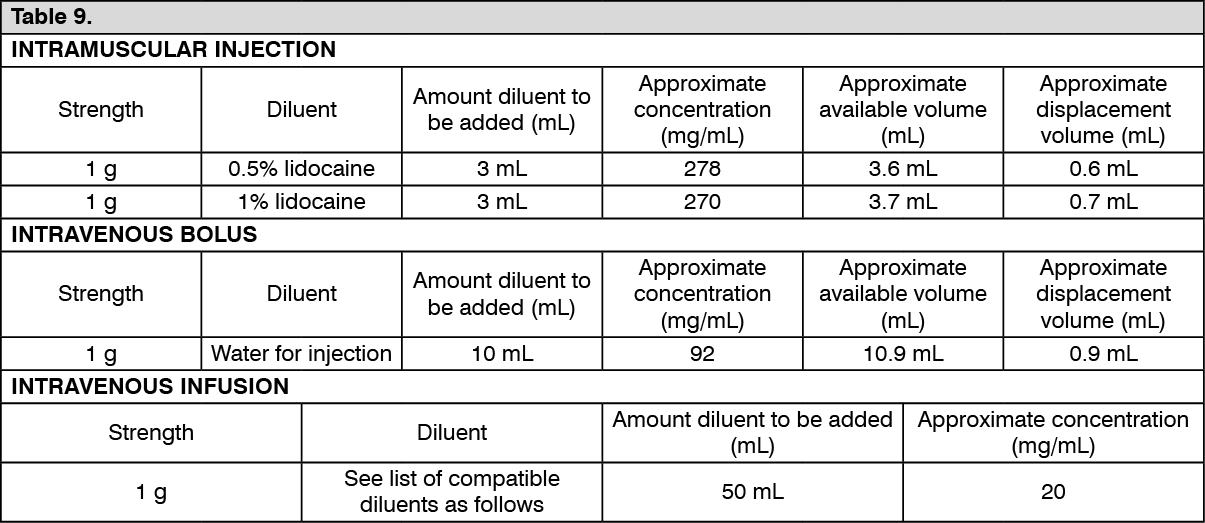 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
