Pharmacotherapeutic group: None.
ATC code: None.
Pharmacology: Mechanism of Action: Lemborexant is a competitive antagonist of both orexin receptors, OX1R and OX2R, with a higher affinity for OX2R. It belongs to the pharmacologic class of orexin receptor antagonists. The orexin neuropeptide signaling system is a central promoter of wakefulness. Blocking the binding of wake-promoting neuropeptides orexin A and orexin B to receptors OX1R and OX2R is thought to suppress wake drive.
Pharmacodynamics: Cardiac Electrophysiology: The effect of lemborexant on the QTc interval using a high precision analysis was measured in multiple dose studies in human patients administered daily doses up to 75 mg. The concentration-response relationship was analyzed using a linear mixed-effects model. The model-predicted QTc effect at the highest observed concentration was 1.1 msec (90% CI: -3.49 to 5.78), indicating that a QTc prolongation effect >10 msec could be excluded at a dose 7.5-times the maximum recommended dose. Thus, lemborexant does not prolong the QTc interval at clinically relevant doses.
Clinical Efficacy: Lemborexant was evaluated for efficacy and safety in 2 clinical trials (each with >900 patients) in patients with insomnia characterized by difficulties with sleep onset and/or sleep maintenance.
The efficacy and safety of lemborexant was evaluated in Study E2006-G000-303 (Study 303), a randomized, double-blind and placebo-controlled 6 month sleep diary study, followed by an additional 6 months of blinded active treatment period where all patients received lemborexant. Study E2006-G000-304 (Study 304) was a 1-month, randomized, double-blind, placebo- and active-controlled, parallel-group polysomnography (PSG) and sleep diary study. In both studies, adult patients (mean age 51.8 years; 714 females, 213 males) were treated with lemborexant 5 mg (n=467) or 10 mg (n=460). Elderly patients (≥65 years; mean age 70.4 years, 342 females, 149 males) were treated with lemborexant 5 mg (n=246) or 10 mg (n=245).
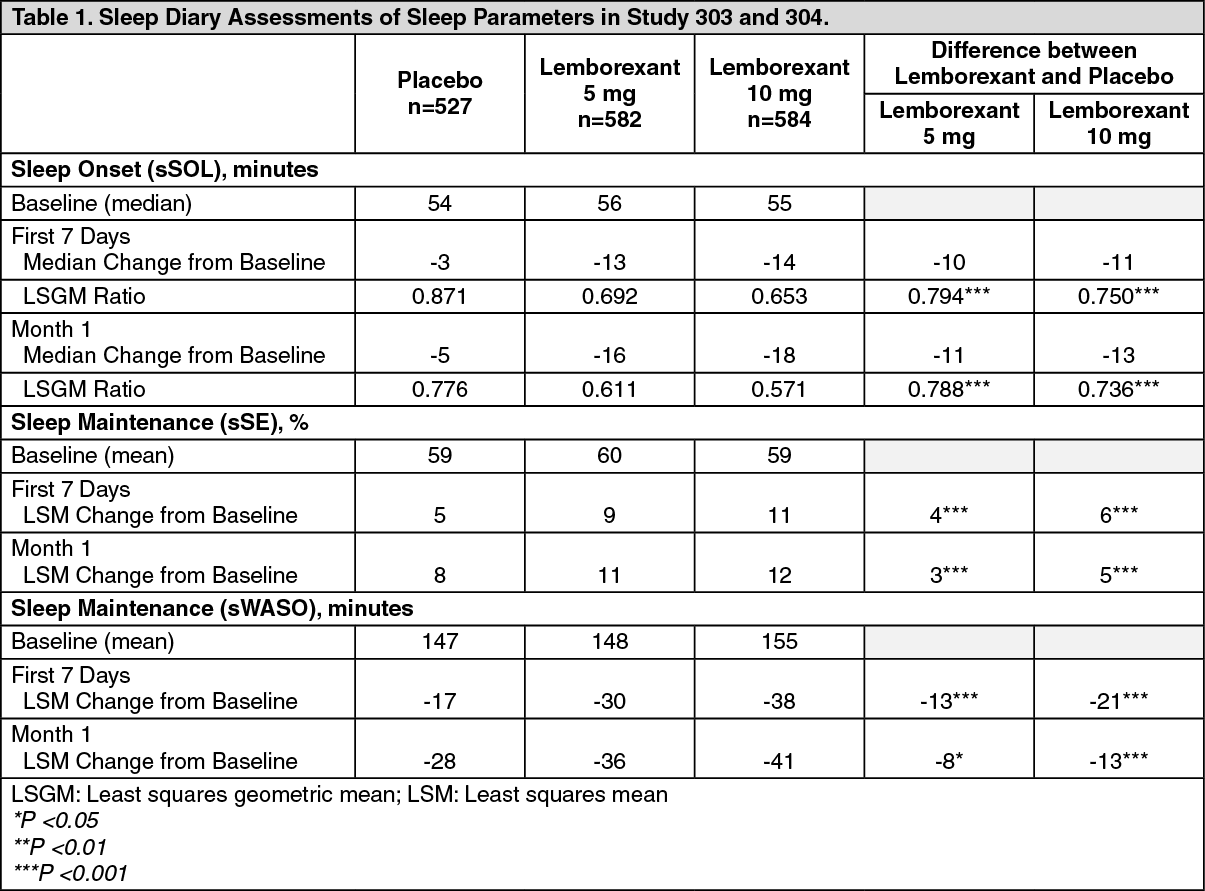
In Study 303 and Study 304, as measured by subjective and/or objective methods, lemborexant led to significantly larger decreases (improvements) in both the time needed to fall asleep and the amount of time spent awake during the night after sleep onset compared to placebo, and significantly larger increases in sleep efficiency (time spent asleep/time spent in bed) compared to placebo, all of which were sustained through 6 months (Tables 1, 2, & 3).
In Study 304, lemborexant 5 mg and 10 mg led to significantly larger decreases in sleep onset (latency to persistent sleep [LPS]) and wake after sleep onset (WASO) during the full sleep period and during the second half of the sleep period) compared to placebo as assessed objectively by PSG. Lemborexant led to significantly larger increases in sleep efficiency (SE) compared to placebo (Table 1). As measured by PSG, lemborexant 5 mg and 10 mg led to significantly larger decreases in sleep onset (LPS), WASO across the entire night, and WASO in the second half of the night compared with active comparator.
The statistically significant effects of lemborexant on patient-reported (subjective) sleep onset and sleep maintenance (sWASO and sSE) after the first 7 nights of treatment remained statistically significant compared with placebo through 6 months (Study 303).
The efficacy of lemborexant was similar between women and men, adult and elderly, and between Caucasians and non-Caucasians. (See Tables 1, 2 and 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Special Safety Studies:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Special Safety Studies: Effects on Driving: A randomized, double-blind, placebo- and active-controlled, four-period crossover study evaluated the effects of nighttime administration of lemborexant on next-morning driving performance approximately 9 hours after dosing in 24 healthy elderly patients (≥65 years old, median age 67 years; 14 men, 10 women) and 24 adult patients (median age 49 years; 12 men, 12 women). The primary driving performance outcome measure was change in Standard Deviation of Lateral Position (SDLP). Testing was conducted after one night (a single dose) and after eight consecutive nights of treatment with lemborexant. Although lemborexant at doses of 5 mg and 10 mg did not cause statistically significant impairment in next-morning driving performance in adult or elderly subjects (compared with placebo), driving ability was impaired in some subjects taking 10 mg lemborexant. Patients using the 10 mg dose should be cautioned about the potential for next-morning driving impairment because there is individual variation in sensitivity to lemborexant. The results of a symmetry analysis support the findings from the primary outcome.
Effects on Next-day Postural Stability and Cognitive Performance: The effect of lemborexant on next-day postural stability and cognitive performance (tests of attention and memory) compared to placebo was evaluated in 2 randomized, placebo-and active-controlled trials in healthy subjects and insomnia patients age 55 and older. There were no meaningful differences between lemborexant (5 mg or 10 mg) and placebo on next-day postural stability or memory.
Middle of the Night Safety in Older Patients (age 55 years and older): The effect of lemborexant was evaluated in a randomized, placebo- and active-controlled trial with a scheduled awakening 4 hours after the start of the 8-hour time in bed. Postural stability, the ability to awaken in response to a sound stimulus, and attention and memory were tested following the awakening. The active comparator in the study, showed a statistically significant decrease in postural stability (increased body sway) compared to both lemborexant and placebo. There were no statistical differences between lemborexant and placebo on the ability to awaken in response to sound. There were no statistically significant differences between lemborexant 5 mg and placebo on measures of attention and memory.
Rebound Insomnia: Rebound insomnia was assessed by comparing sleep diary-recorded sSOL and sWASO from the screening period to the two weeks following treatment discontinuation in both Study 303 (12 months) and Study 304 (1 month). Analyses of group means and the proportion of patients with rebound insomnia suggest that lemborexant was not associated with rebound insomnia following treatment discontinuation.
Withdrawal Effects: In a 12-month and 1-month controlled safety and efficacy trials (Study 303, Study 304, respectively), withdrawal effects were assessed by the Tyrer Benzodiazepine Withdrawal Symptom Questionnaire following discontinuation from study drug in patients who received lemborexant 5 mg or 10 mg. There was no evidence of withdrawal effects following lemborexant discontinuation at either dose.
Respiratory Safety: In a study of healthy adult and elderly patients, there were no differences between placebo and lemborexant 10 mg and 25 mg with respect to mean peripheral capillary oxygen saturation during sleep. In a study of patients with mild sleep apnea, overall, lemborexant did not increase the frequency of apneic events or decrease mean peripheral capillary oxygen saturation when compared with placebo following single and multiple doses of 10 mg.
In a study of patients with moderate or severe obstructive sleep apnea (apnea-hypopnea index ≥15 events per hour of sleep), overall, lemborexant did not increase the frequency of apneic events or decrease mean peripheral capillary oxygen saturation following single or multiple doses of 10 mg. In a study of patients with moderate or severe chronic obstructive pulmonary disease (COPD), overall, lemborexant did not increase the frequency of apneic events or decrease mean peripheral capillary oxygen saturation following single or multiple doses of 10 mg.
Daily Functioning: In Study 303 and Study 304, the effect of lemborexant on daily functioning was assessed by scores on the Insomnia Severity Index (ISI). For patients treated with lemborexant, the ISI score decreased significantly compared to placebo, indicating that patients treated with lemborexant had improvement of functional impairment.
Sleep Stages: In Study 304, sleep stages for patients treated with lemborexant were assessed by polysomnography. Lemborexant demonstrated a significant increase in rapid eye movement (REM) sleep compared to placebo and to zolpidem tartrate ER.
Pharmacokinetics: Absorption: In healthy patients, the pharmacokinetic profile of lemborexant was examined after single doses of up to 200 mg and after once-daily administration of up to 75 mg for 14 days. Lemborexant is rapidly absorbed, with a time to peak concentration (tmax) of approximately 1 to 3 hours. Lemborexant exhibits linear pharmacokinetics with multi-exponential decline in plasma concentrations. The extent of accumulation of lemborexant at steady-state is 1.5- to 2-fold across the dose range. The effective half-life for 5 mg and 10 mg is 17 and 19 hours respectively. The plasma concentration at 9 hours after administration is approximately 10% to 13% of the Cmax.
Ingestion of lemborexant with a high-fat meal resulted in a decrease in the rate of absorption as demonstrated by 23% decrease in C
max and delay in t
max of 2 hours and 18% increase in total exposure AUC.
Time to sleep onset may be delayed if taken with or soon after a meal.
Distribution: The volume of distribution of lemborexant is 1970 L. Plasma protein binding of lemborexant in clinical samples is approximately 94%. The blood to plasma concentration ratio of lemborexant is 0.65.
In vitro binding of lemborexant and its major circulating metabolite, M10 (the N-oxide of lemborexant) to human plasma proteins ranged from 87.4% to 88.7% and 91.5% to 92.0%, respectively, at concentrations of 100 to 1000 ng/mL. At these concentrations in vitro, lemborexant was bound primarily to human serum albumin, low-density lipoprotein, and high-density lipoprotein. In vitro blood to plasma concentration ratios of lemborexant and M10 in humans were 0.610 to 0.656 and 0.562 to 0.616, respectively, at concentrations of 100 to 1,000 ng/mL.
Metabolism: Lemborexant is primarily metabolized by CYP3A4, and to a lesser extent by CYP3A5. M10 is the only major circulating metabolite (12% of parent). The contribution of this metabolite to the pharmacologic activity of lemborexant is considered to be minimal.
Elimination: The primary route of elimination is through the feces, with 57.4% of radiolabeled dose recovered in the feces and 29.1% in the urine. The percent of lemborexant excreted unchanged in the urine is negligible (<1% dose). The effective half-life of lemborexant 5 mg and 10 mg is 17 and 19 hours respectively.
Special Populations: Age, Sex, Race/Ethnicity and BMI: No clinically significant differences in the pharmacokinetics of lemborexant were observed based on age, sex, race/ethnicity, or body mass index.
Geriatric Patients: Based on a population pharmacokinetic analysis in patients receiving 5 or 10 mg lemborexant once daily, apparent clearance was 26% lower in elderly (>65 years of age). However, this effect was not clinically relevant.
Pediatric Patients: No studies have been conducted to investigate the pharmacokinetics of lemborexant in pediatric patients.
Patients with Renal Impairment: Severe renal impairment (urinary creatinine clearance ≤30 mL/min/1.73m
2) increased lemborexant exposure (AUC) 1.5-fold but had no effect on C
max. No dose adjustment is required in patients with renal impairment.
Patients with Hepatic Impairment: Lemborexant has not been studied in patients with severe hepatic impairment. Use in this population is not recommended.
Mild (Child-Pugh A) and moderate (Child-Pugh B) hepatic insufficiency increased lemborexant AUC and C
max by 1.5-fold. Terminal half-life was only increased in patients with moderate hepatic impairment (Child-Pugh class B). No relationship between these findings and hepatic function was observed.
Exposures of lemborexant in patients with hepatic and renal impairment are summarized in Figure 1. (See Figure 1.)
Click on icon to see table/diagram/image
Drug Interaction Studies: Effects of Other Drugs on Lemborexant: The effects of other drugs on the pharmacokinetics of lemborexant (10 mg) are presented in Figure 2 as change relative to lemborexant alone (test/reference). Based on these results, drug interactions between lemborexant and strong CYP3A inducers, strong CYP3A inhibitors, and moderate CYP3A inhibitors are clinically significant. Using a physiologically based pharmacokinetic (PBPK) model, a weak effect is predicted when weak CYP3A inhibitors (e.g.,fluoxetine) are co-administered with lemborexant. Co-administration of moderate (e.g., fluconazole) or strong (e.g., itraconazole) CYP3A inhibitors significantly increased lemborexant exposure. CYP3A inducers (e.g., rifampin) significantly decreased lemborexant exposure.
There was no evidence of an additive effect on impairing postural stability (as evidenced by body sway) when lemborexant was co-administered with alcohol; lemborexant did not impact postural stability when dosed alone. An additive negative effect on cognitive performance was observed up to 6 hours post dose when lemborexant 10 mg was co-administered with a single dose of alcohol (0.6 g/kg for females and 0.7 g/kg for males).
Co-administration of an H2 blocker (famotidine) with lemborexant decreased C
max by 27% and delayed t
max by 0.5 hours, but had no statistically significant effect on overall lemborexant exposure (AUC). A population analysis of Phase 1-3 data also showed no effect of proton pump inhibitors (PPIs) on apparent clearance of lemborexant. A pooled analysis conducted on patients with a medical history of gastroesophageal reflex disease (GERD) or taking PPIs or H2 blockers in Study 303 and 304 showed that there was no effect on sleep latency or on safety parameters. Thus lemborexant can be co-administered with gastric acid-reducing agents (PPIs or H2 blockers).
Co-administration of an oral contraceptive containing norethindrone (NE) and ethinyl estradiol (EE) with lemborexant had no statistically significant effect on lemborexant pharmacokinetics. (See Figure 2.)
Click on icon to see table/diagram/image
Effects of Lemborexant on Other Drugs: In vitro metabolism studies demonstrated that lemborexant and M10 have a potential to induce CYP3A and a weak potential to inhibit CYP3A and induce CYP2B6. Lemborexant and M10 do not have the potential to inhibit other CYP isoforms or transporters (P-gp, BCRP, BSEP, OAT1, OAT3, OATP1B1, OATP1B3, OCT1, OCT2, MATE1, and MATE2-K). Lemborexant and M10 do not induce CYP2C8, CYP2C9, and CYP2C19 at clinically relevant concentrations. Lemborexant is a poor substrate of P-gp, but M10 is a substrate of P-gp. Lemborexant and M10 are not substrates of BCRP, OATP1B1, or OATP1B3.
Specific in vivo effects of lemborexant (10 mg) on the pharmacokinetics of bupropion, oral contraceptives, and midazolam are presented in Figure 3 as a change relative to the interacting drug administered alone (test/reference). Based on these results, drug interactions between lemborexant and CYP2B6 substrates are clinically significant. Lemborexant is expected to have minimal effect on the pharmacokinetics of CYP2C8, CYP2C9, or CYP2C19 substrates.
Co-administration of an oral contraceptive containing norethindrone (NE) and ethinyl estradiol (EE) with lemborexant (10 mg) did not affect the Cmax and AUC of NE or the Cmax of EE, and increased AUC of EE by 13%. This latter small change is not considered clinically relevant.
Clinical studies with substrates of CYP3A or CYP2B6: Despite the in vitro findings, lemborexant does not induce or inhibit CYP3A4. Lemborexant weakly induces CYP2B6 (e.g., bupropion is CYP2B6 substrate). CYP3A and CYP2B6 substrates can be co-administered with lemborexant. (See Figure 3.)
Click on icon to see table/diagram/image
Toxicology: Preclinical Safety Data: Fertility: Lemborexant was orally administered to female rats at doses of 30, 100, or 1000 mg/kg/day prior to and throughout mating and continuing to gestation Day 6. These doses are approximately 12 to >500 times the MRHD based on AUC. Irregular estrous cycles and decreased pregnancy rate were observed at 60 times the MRHD based on AUC, and decreased numbers of corpora lutea, implantations, and live embryos were observed at >500 times the MRHD based on AUC. The exposure at the NOAEL of 30 mg/kg/day is approximately 12 times the MRHD based on AUC. Lemborexant did not affect fertility when orally administered to male rats at doses of 30, 100, or 1000 mg/kg/day prior to and throughout mating; the highest dose is approximately 138 times the MRHD based on AUC.
Carcinogenesis: Lemborexant did not increase the incidence of tumors in rats treated for 2 years at oral doses of 30, 100, and 300 mg/kg/day (males) and 10, 30, and 100 mg/kg/day (females), which are >80 times the MRHD based on AUC. Lemborexant did not increase the incidence of tumors in Tg ras H2 mice treated for 26 weeks at oral doses of 50, 150, and 500 mg/kg/day.
Mutagenesis: Lemborexant was neither mutagenic nor clastogenic in a standard battery of in vitro and in vivo genotoxicity studies.
Animal Toxicology and/or Pharmacology: Lemborexant administered to mice at oral doses of 10 or 30 mg/kg resulted in behavior characteristic of cataplexy when presented with chocolate. Chocolate is a stimulus that has been demonstrated to increase cataplexy occurrences in narcoleptic mice.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image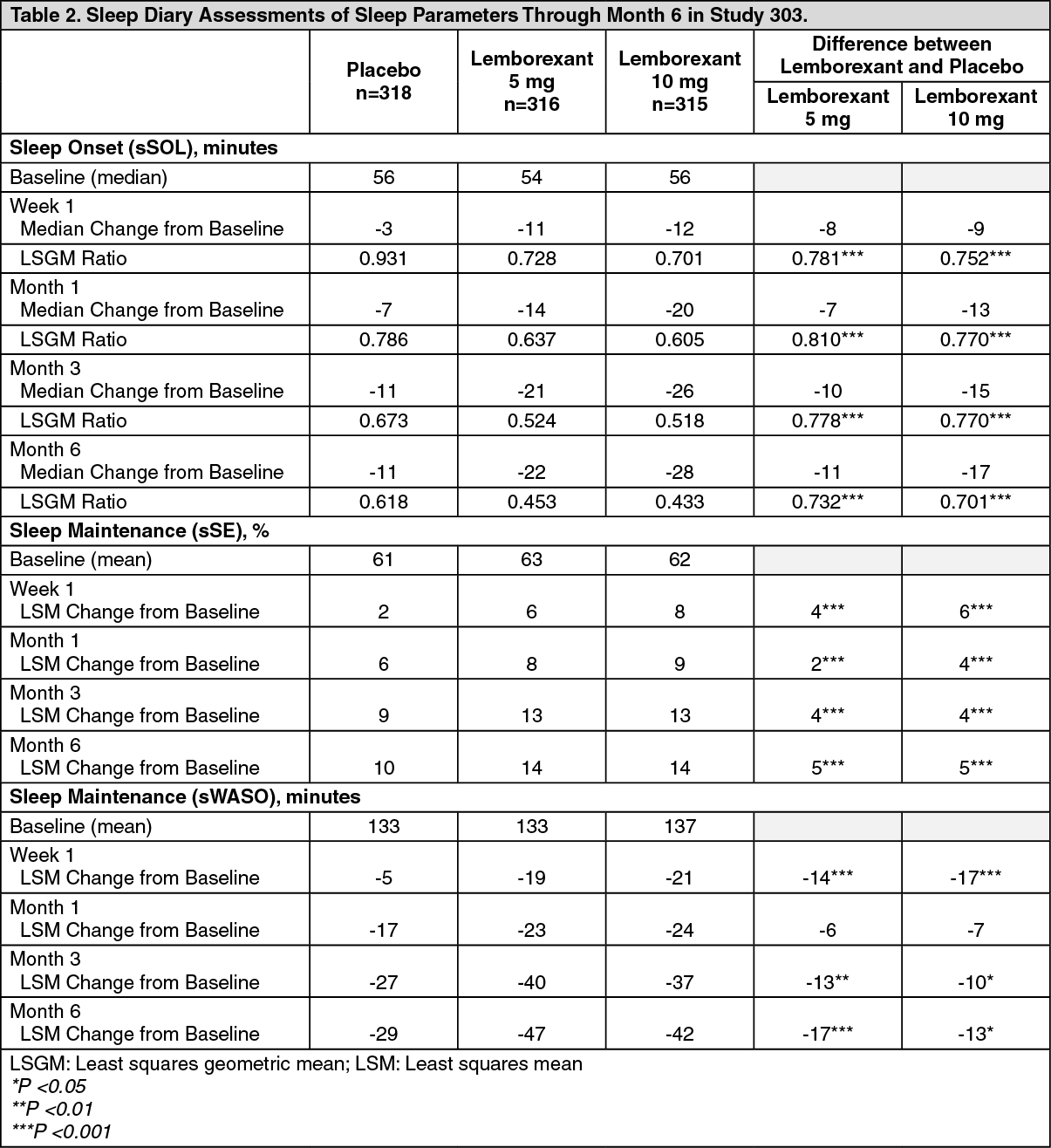 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image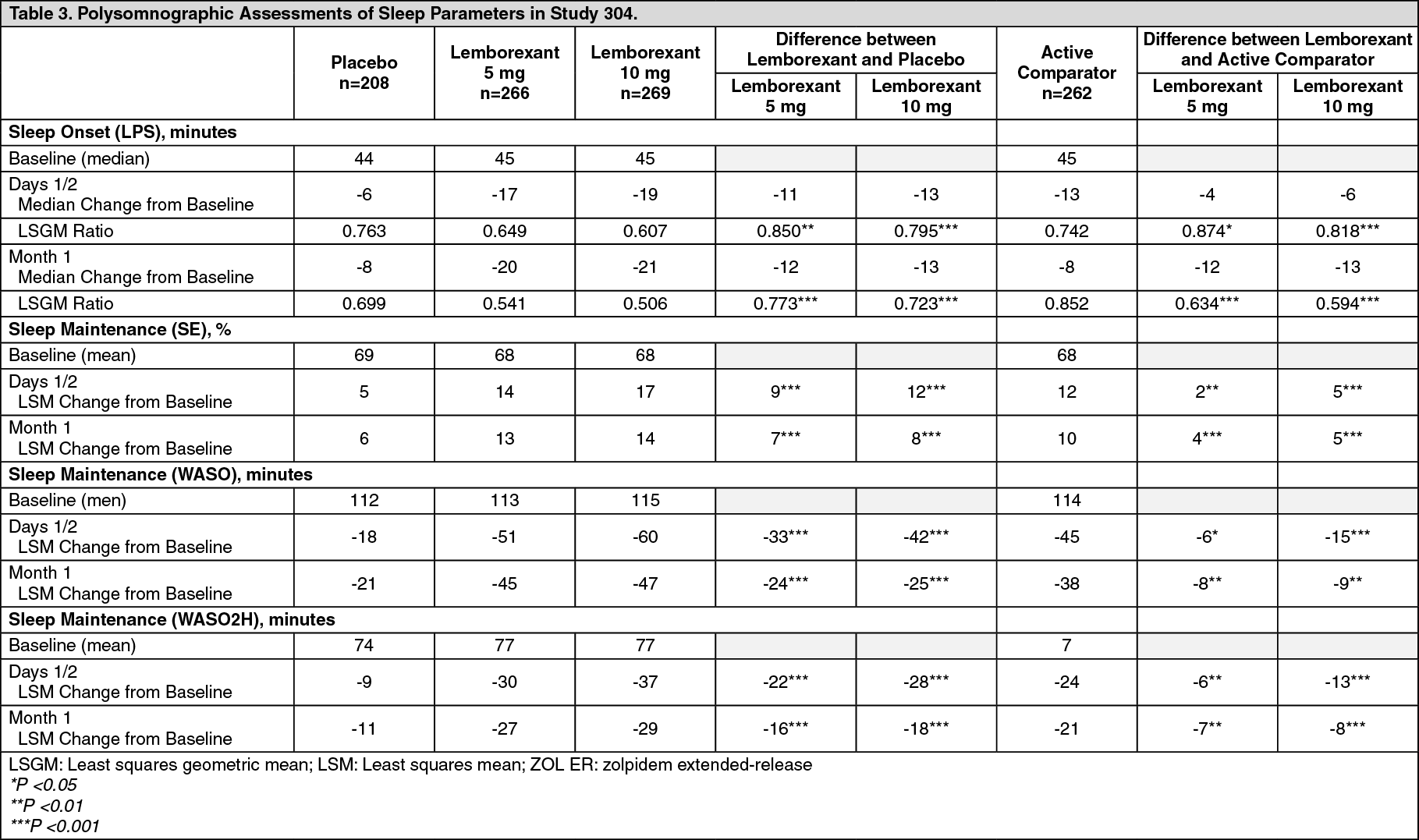 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image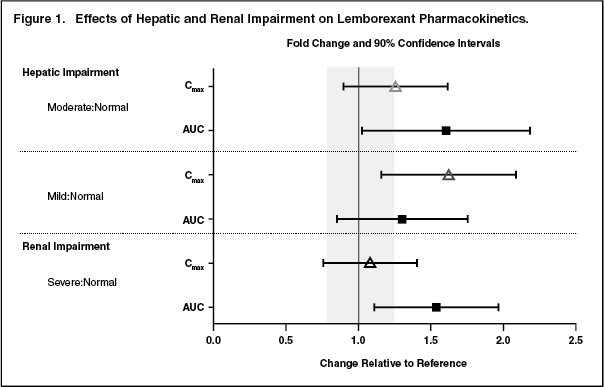 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image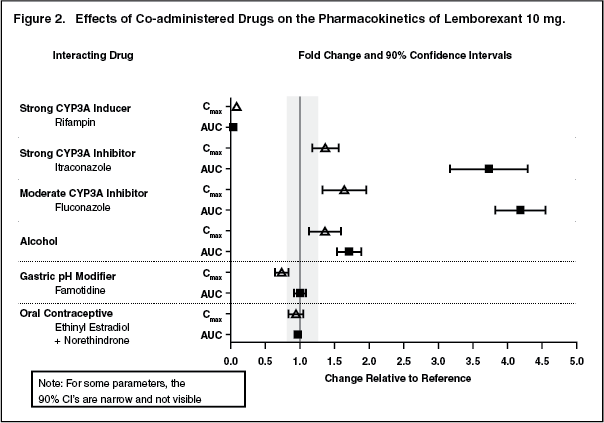 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image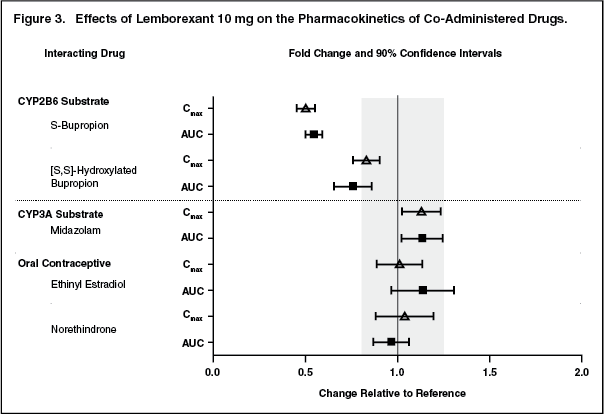 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image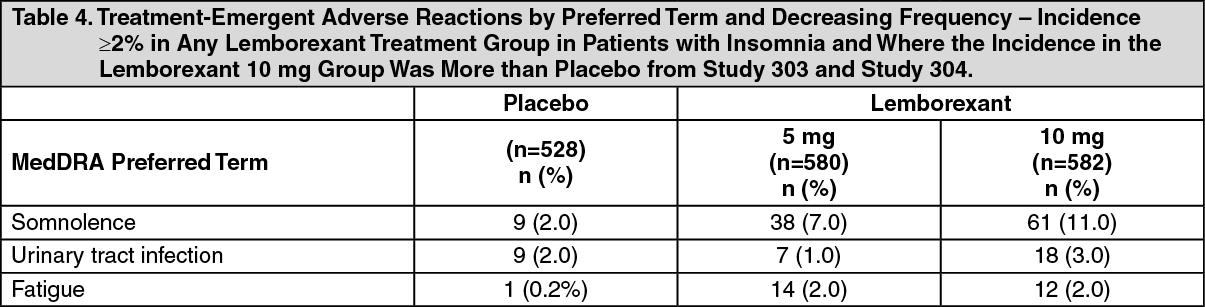 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
