The most common drug-related adverse event reported during therapy with Aggrastat when used concomitantly with heparin and aspirin was bleeding (usually reported by the investigators as oozing or mild). The incidences of major and minor bleeding using the Thrombolysis in Myocardial Infarction (TIMI) criteria in the Platelet Receptor Inhibition for Ischemic Syndrome Management - Patients Limited by Unstable Signs and Symptoms (PRISM PLUS) and Randomized Efficacy Study of Tirofiban for Outcomes and Restenosis (RESTORE) studies are shown as follows: See Table 3.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
There were no reports of intracranial bleeding in the PRISM PLUS study for Aggrastat in combination with heparin or in the control group (which received heparin). The incidence of intracranial bleeding in the RESTORE study was 0.1% for Aggrastat in combination with heparin and 0.3% for the control group (which received heparin). In the PRISM PLUS study, the incidences of retroperitoneal bleeding reported for Aggrastat in combination with heparin, and for the control group were 0% and 0.1%, respectively. In the RESTORE study, the incidences of retroperitoneal bleeding reported for Aggrastat in combination with heparin and the control group were 0.6% and 0.3%, respectively.
Female patients and elderly patients receiving Aggrastat with heparin or heparin alone had a higher incidence of bleeding complications than male patients or younger patients, respectively. The incremental risk of bleeding in patients treated with Aggrastat in combination with heparin over the risk in patients treated with heparin alone was comparable regardless of age or gender. No dose adjustment is recommended for these populations (see Other Patient Populations under Dosage & Administration).
Patients treated with Aggrastat, with heparin, were more likely to experience decreases in platelet counts than the control group. These decreases were reversible upon discontinuation of Aggrastat. The percentage of patients with a decrease of platelets to <90,000 cells/mm
3 was 1.5%. The percentage of patients with a decrease of platelets to <50,000 cells/mm
3 was 0.3%.
The most frequent drug-related nonbleeding side effects reported with Aggrastat, administered concomitantly with heparin, occurring at an incidence of >1% were nausea (1.7%), fever (1.5%) and headache (1.1%); nausea, fever and headache occurred at an incidence of 1.4%, 1.1% and 1.2%, respectively, in the control group.
In clinical studies, the incidences of adverse events were generally similar among different races, patients with or without hypertension, patients with or without diabetes mellitus, and patients with or without hypercholesteremia.
The overall incidence of nonbleeding adverse events was higher in female patients (compared to male patients) and older patients (compared to younger patients). However, the incidences of nonbleeding adverse events in these patients were comparable between the Aggrastat with heparin and the heparin alone groups. (See previous text for bleeding adverse events.)
The following additional adverse reactions have been reported in post-marketing experience:
Body as a Whole: Decreased platelet counts (see previous text) associated with chills and low-grade fever.
Laboratory Test Findings: The most frequently observed laboratory adverse events in patients receiving Aggrastat concomitantly with heparin were related to bleeding. Decreases in hemoglobin and hematocrit, and platelet count were observed. Increases in the presence of urine and fecal occult blood were also observed.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image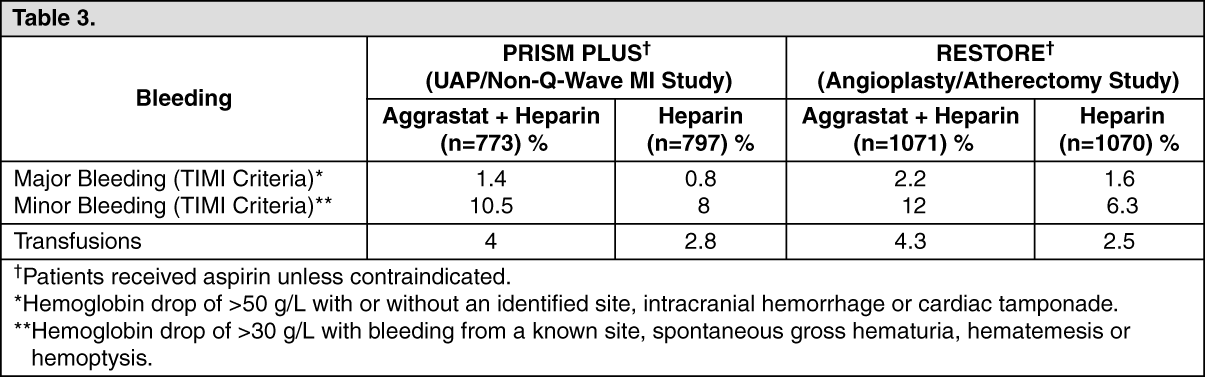 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
