Pharmacology: Mechanism of Action: Ceritinib is a kinase inhibitor. Targets of ceritinib inhibition identified in either biochemical or cellular assays at clinically relevant concentrations include ALK, insulin-like growth factor 1 receptor (IGF-1R), insulin receptor (InsR), and ROS1. Among these, ceritinib is most active against ALK. Ceritinib inhibited autophosphorylation of ALK, ALK-mediated phosphorylation of the downstream signaling protein STAT3, and proliferation of ALK-dependent cancer cells in in vitro and in vivo assays.
Ceritinib inhibited the in vitro proliferation of cell lines expressing EML4-ALK and NPM-ALK fusion proteins and demonstrated dose-dependent inhibition of EML4-ALK-positive NSCLC xenograft growth in mice and rats. Ceritinib exhibited dose-dependent anti-tumor activity in mice bearing EML4-ALK-positive NSCLC xenografts with demonstrated resistance to crizotinib, at concentrations within a clinically relevant range.
Pharmacodynamics: Cardiac Electrophysiology: Twelve of 919 patients (1.3%) treated with ZYKADIA 750 mg once daily under fasted conditions with at least one post-baseline ECG assessment were found to have a QTc >500 msec and 58 patients (6%) had an increase from baseline QTc >60 msec. In ASCEND-4, a central tendency analysis of the QTc data at average steady-state concentrations demonstrated that the upper bound of the 2-sided 90% CI for QTc was 15.3 msec at ZYKADIA 750 mg once daily under fasted conditions. A pharmacokinetic/pharmacodynamic analysis suggested concentration-dependent QTc interval prolongation [see QT Interval Prolongation under Precautions].
Ten of 925 patients (1.1%) had bradycardia defined as <50 beats per minute [see Bradycardia under Precautions].
Clinical Studies: Previously Untreated ALK-Positive Metastatic NSCLC: The efficacy of ZYKADIA for the treatment of patients with ALK-positive NSCLC who had not received prior systemic therapy for metastatic disease was evaluated in an open-label, randomized, active-controlled, multicenter study (ASCEND-4, NCT01828099). Patients were required to have World Health Organization (WHO) performance status 0-2 and ALK-positive NSCLC as identified by the VENTANA ALK (D5F3) CDx Assay. Neurologically stable patients with central nervous system (CNS) metastases that did not require increasing doses of steroids to manage CNS symptoms were permitted to enroll. Patients with uncontrolled diabetes mellitus; a history of ILD or interstitial pneumonitis; or a history of pancreatitis, or increased amylase, or lipase that was due to pancreatic disease were not eligible.
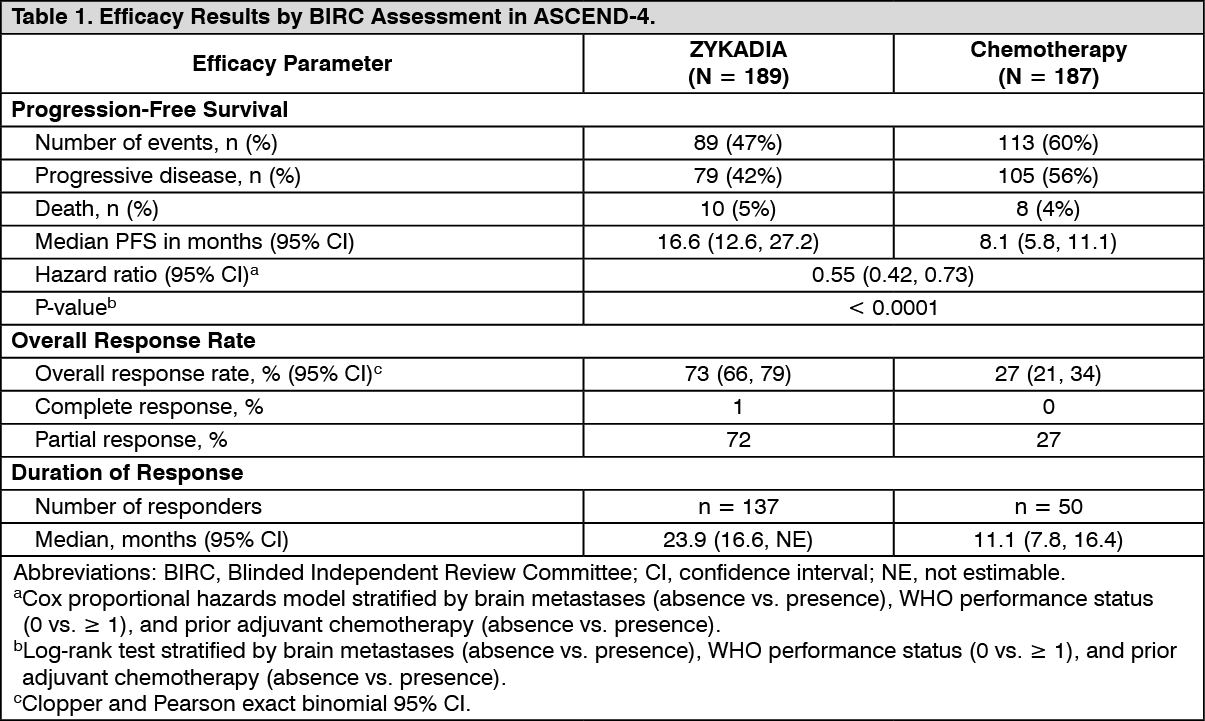
The major efficacy outcome measure was progression-free survival (PFS) as determined by Blinded Independent Review Committee (BIRC) according to RECIST v1.1. Additional efficacy outcome measures were overall survival (OS), overall response rate (ORR) and duration of response (DOR) determined by BIRC, overall intracranial response rate (OIRR), duration of intracranial response (DOIR) determined by BIRC neuro-radiologist, and patient-reported outcomes.
Patients were randomized 1:1 to receive ZYKADIA 750 mg orally daily under fasted conditions or chemotherapy and maintenance chemotherapy. Randomization was stratified by WHO performance status, prior adjuvant/neoadjuvant chemotherapy and presence or absence of brain metastases. Patients randomized to chemotherapy received pemetrexed (500 mg/m
2) and investigator's choice of cisplatin (75 mg/m
2) or carboplatin (AUC of 5 - 6 mg*min/mL) administered on Day 1 of each 21-day cycle for a maximum of 4 cycles followed by pemetrexed (500 mg/m
2) every 21 days. Treatment in both arms was continued until disease progression or unacceptable toxicity.
The study population characteristics were: 57% female, median age 54 years (range, 22 to 81 years), 22% age 65 years or older, 54% white, 42% Asian, 2% black, and 2% other races. The majority of patients had adenocarcinoma (97%) and never smoked (61%). CNS metastases were present in 32% (n = 121) of patients. Approximately half (n = 55) had measurable CNS metastases as determined by BIRC neuro-radiologist and 71% (n = 39) of these patients received no prior intracranial radiotherapy. Of those randomized to chemotherapy, 43% received ZYKADIA as the next antineoplastic therapy after platinum-based chemotherapy.
Efficacy results from ASCEND-4 are summarized in Table 1 and Figure 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
There was no significant difference in OS in a pre-specified interim analysis conducted at 42% of the events required for the final analysis. (See figure.)
Click on icon to see table/diagram/image
Antitumor activity of ZYKADIA in the brain was assessed in patients with measurable disease as determined by the BIRC neuro-radiologist at baseline (N = 55) according to RECIST 1.1. (See Table 2.)
Click on icon to see table/diagram/image
Exploratory analyses of patient-reported outcome measures suggested a delay in time to development of or worsening of shortness of breath in patients treated with ZYKADIA as compared to chemotherapy. The patient-reported delay in onset or worsening of shortness of breath may be an overestimation, because patients were not blinded to treatment assignment.
Previously Treated ALK-Positive Metastatic NSCLC: The efficacy of ZYKADIA was evaluated in a multicenter, single-arm, open-label clinical trial (ASCEND-1, NCT01283516). A total of 163 patients with metastatic ALK-positive NSCLC who progressed while receiving or were intolerant to crizotinib were enrolled. The major efficacy outcome measure was objective response rate (ORR) according to RECIST v1.0 as evaluated by both investigators and BIRC. Duration of response was an additional outcome measure. All patients received ZYKADIA at a dose of 750 mg once daily under fasted conditions.
The study population characteristics were: median age 52 years, age less than 65 (87%), female (54%), white (66%), Asian (29%), never or former smoker (97%), ECOG PS 0 or 1 (87%), progression on previous crizotinib (91%), number of prior therapies 2 or more (84%), and adenocarcinoma histology (93%). Sites of extra-thoracic metastases included brain (60%), liver (42%), and bone (42%). ALK-positivity was verified retrospectively by review of local test results for 99% of patients.
Efficacy results from ASCEND-1 are summarized in Table 3. (See Table 3.)
Click on icon to see table/diagram/image
The analysis by the BIRC assessment was similar to the analysis by the investigator assessment.
Pharmacokinetics: After a single oral administration of ZYKADIA in patients, AUC and C
max increased dose proportionally over 50 mg to 750 mg under fasted conditions.
Following ZYKADIA 750 mg once daily under fasted conditions, steady state was reached by 15 days with a geometric mean accumulation ratio of 6.2 after 3 weeks. Systemic exposure increased in a greater than dose proportional manner after repeat doses of 50 mg to 750 mg once daily under fasted conditions.
Absorption: After a single oral administration of ZYKADIA in patients, peak plasma levels (C
max) of ceritinib were achieved around 4 to 6 hours.
Food Effect: A food effect study conducted in healthy subjects with a single 500 mg dose of ZYKADIA capsules showed that a high‐fat meal (containing approximately 1000 calories and 58 grams of fat) increased ceritinib AUC by 73% and C
max by 41% and a low‐fat meal (containing approximately 330 calories and 9 grams of fat) increased ceritinib AUC by 58% and C
max by 43% as compared with the fasted conditions.
Dose Optimization Study: Dosing Regimen of 450 mg Daily With Food: In a dose optimization study (ASCEND-8) in patients receiving 450 mg dose of ZYKADIA capsules daily with food (approximately 100 to 500 calories and 1.5 to 15 grams of fat) or 750 mg daily under fasted conditions, there was no clinically meaningful difference in the systemic steady-state exposure of ceritinib (AUC) between the 450 mg with food arm and the 750 mg fasted arm.
Distribution: Ceritinib is 97% bound to human plasma proteins, independent of drug concentration. The geometric mean apparent volume of distribution (V
d/F) is 4230 L following a single 750 mg ZYKADIA dose under fasted conditions in patients. Ceritinib also has a slight preferential distribution to red blood cells, relative to plasma, with a mean in vitro blood-to-plasma ratio of 1.35.
Elimination: Following a single 750 mg ZYKADIA dose under fasted conditions, the geometric mean apparent plasma terminal half-life (t
½) of ceritinib was 41 hours in patients. Ceritinib demonstrates nonlinear PK over time. The geometric mean apparent clearance (CL/F) of ceritinib was lower at steady state (33.2 L/h) after 750 mg daily dosing than after a single 750 mg dose (88.5 L/h).
Metabolism: In vitro studies demonstrated that CYP3A was the major enzyme involved in the metabolic clearance of ceritinib. Following oral administration of a single 750 mg radiolabeled dose under fasted conditions, ceritinib was the main circulating component (82%) in human plasma.
Excretion: Following oral administration of a single 750 mg radiolabeled dose under fasted conditions, 92% of the administered dose was recovered in the feces (with 68% as unchanged parent compound) while 1.3% of the administered dose was recovered in the urine.
Specific Populations: Age, sex, race, body weight, and mild-to-moderate renal impairment (CLcr 30 to <90 mL/min estimated with Cockcroft-Gault) has no clinically important effect on the systemic exposure of ceritinib based on population pharmacokinetic analyses. Patients with severe renal impairment (CLcr <30 mL/min) were not included in the clinical trial.
Patients with Hepatic Impairment: Following a single 750 mg ZYKADIA dose under fasted conditions, the geometric mean systemic exposure (AUC
0-INF) of ceritinib was increased by 66% and unbound ceritinib AUC
0-INF was increased by 108% in subjects with severe (Child-Pugh C) hepatic impairment compared to subjects with normal hepatic function [see Dosage Modification for Patients With Severe Hepatic Impairment under Dosage & Administration]. Total and unbound systemic exposure of ceritinib were similar in subjects with mild (Child-Pugh A) to moderate (Child-Pugh B) hepatic impairment compared to subjects with normal hepatic function.
Drug Interaction Studies: Effect of Strong CYP3A/P-gp Inhibitors on Ceritinib: Coadministration of a single 450 mg ZYKADIA dose under fasted conditions with ketoconazole (a strong CYP3A/P-gp inhibitor) for 14 days increased ceritinib AUC by 2.9-fold and C
max by 22%. The steady-state AUC of ceritinib at a dose of 450 mg once daily under fasted conditions with ketoconazole for 14 days was predicted to be similar to the steady-state AUC of ceritinib at a dose of 750 mg alone under fasted conditions.
Effect of Strong CYP3A/P-gp Inducers on Ceritinib: Coadministration of a single 750 mg ZYKADIA dose under fasted conditions with rifampin (a strong CYP3A/P-gp inducer) for 14 days decreased ceritinib AUC by 70% and C
max by 44%.
Effect of Ceritinib on CYP3A Substrates: Coadministration of a single dose of midazolam (a sensitive CYP3A substrate) following 3 weeks of ZYKADIA (750 mg daily under fasted conditions) increased the midazolam AUC by 5.4-fold and C
max by 1.8-fold compared to midazolam administered alone [see Effect of ZYKADIA on Other Drugs under Interactions].
Effect of Ceritinib on CYP2C9 Substrates: Coadministration of a single dose of warfarin (a CYP2C9 substrate) following 3 weeks of ZYKADIA (750 mg daily under fasted conditions) increased the S-warfarin AUC by 54% with no change in C
max compared to warfarin administered alone [see Effect of ZYKADIA on Other Drugs under Interactions].
Effect of Acid Reducing Agents on Ceritinib: Coadministration of a single 750 mg ZYKADIA dose under fasted conditions with a proton pump inhibitor (esomeprazole) for 6 days in healthy subjects decreased ceritinib AUC by 76% and C
max by 79%; however, coadministration of a single 750 mg ZYKADIA dose under fasted conditions with proton pump inhibitors for 6 days in a subgroup of patients from ASCEND-1 suggested less effect on ceritinib exposure than that observed in healthy subjects as AUC decreased by 30% and C
max decreased by 25% and no clinically meaningful effect on ceritinib exposure was observed at steady-state.
Effect of Transporters on Ceritinib Disposition: Ceritinib is a substrate of efflux transporter P-gp, but is not a substrate of BCRP, MRP2, OCT1, OAT2, or OATP1B1 in vitro.
Effect of Ceritinib on Transporters: Based on in vitro data, ceritinib is unlikely to inhibit P-gp, BCRP, MRP2, OATP1B1, OATP1B3, OAT1, OAT3, OCT1, or OCT2 at clinical concentrations.
Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: Carcinogenicity studies have not been performed with ceritinib.
Ceritinib was not mutagenic in vitro in the bacterial reverse mutation (Ames) assay but induced numerical aberrations (aneugenic) in the in vitro cytogenetic assay using human lymphocytes, and micronuclei in the in vitro micronucleus test using TK6 cells. Ceritinib was not clastogenic in the in vivo rat micronucleus assay.
There are no data on the effect of ceritinib on human fertility. Fertility/early embryonic development studies were not conducted with ceritinib. There were no adverse effects on male or female reproductive organs in general toxicology studies conducted in monkeys and rats at exposures ≥0.5- and 1.5-fold, respectively, of the human exposure by AUC at the recommended dose.
Animal Toxicology and/or Pharmacology: Target organs in nonclinical animal models included, but were not limited to, the pancreas, biliopancreatic/bile ducts, gastrointestinal tract, and liver. Pancreatic focal acinar cell atrophy was observed in rats at 1.5-fold the human exposure by AUC at the recommended dose. Biliopancreatic duct and bile duct necrosis was observed in rats at exposures ≥5% of the human exposure by AUC at the recommended dose. Bile duct inflammation and vacuolation were also noted in monkeys at exposures ≥0.5-fold the human exposure by AUC at the recommended dose. Frequent minimal necrosis and hemorrhage of the duodenum was exhibited in monkeys at 0.5-fold the human exposure by AUC, and in rats at an exposure similar to that observed clinically.
Ceritinib crossed the blood brain barrier in rats with a brain-to-blood exposure (AUC
inf) ratio of approximately 15%.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image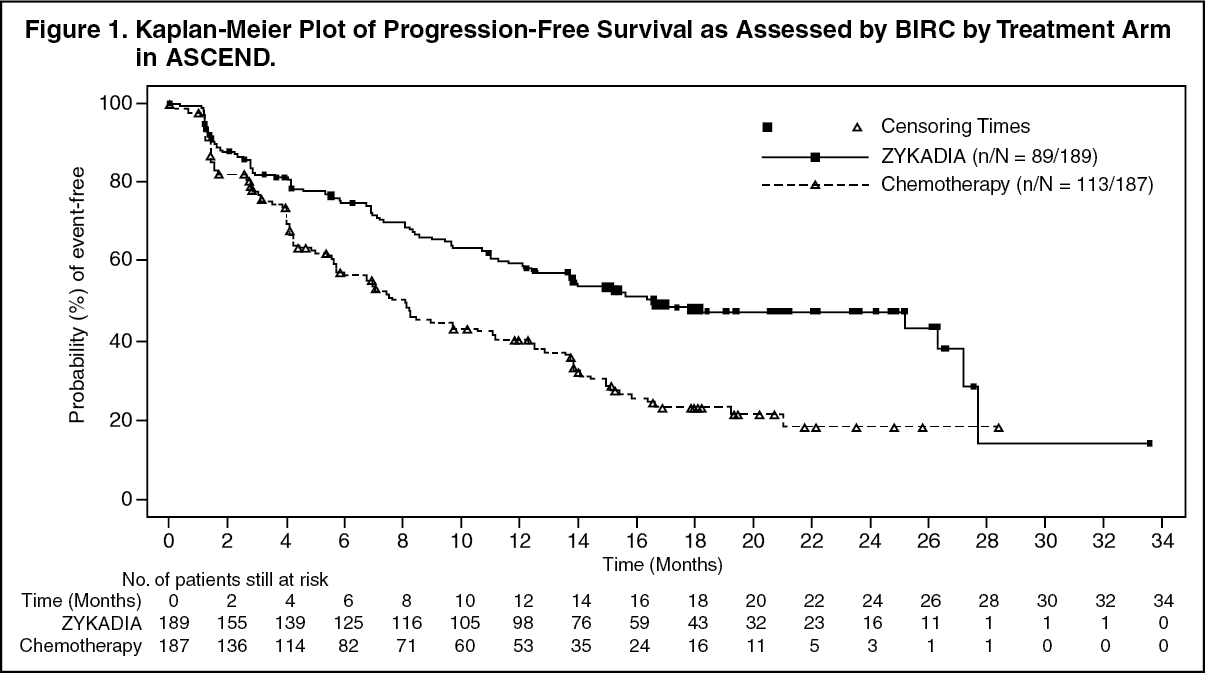 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image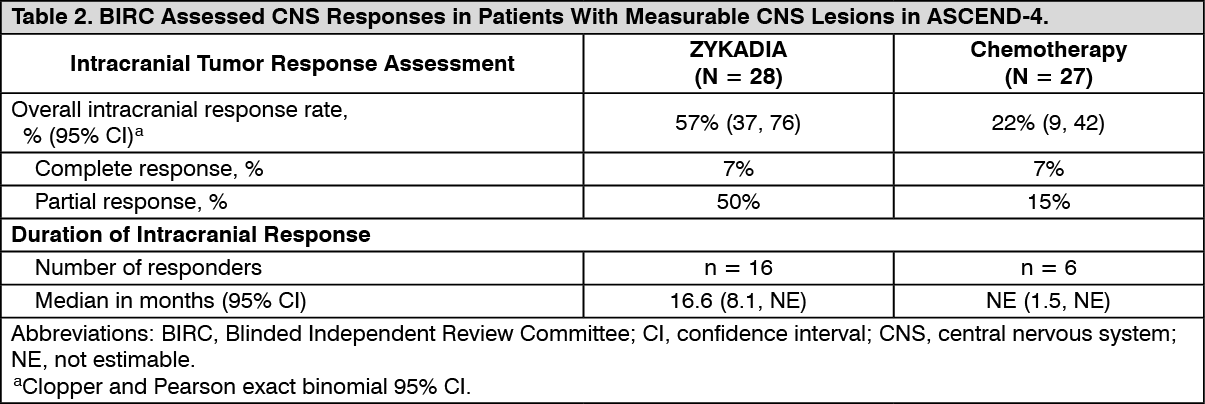 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image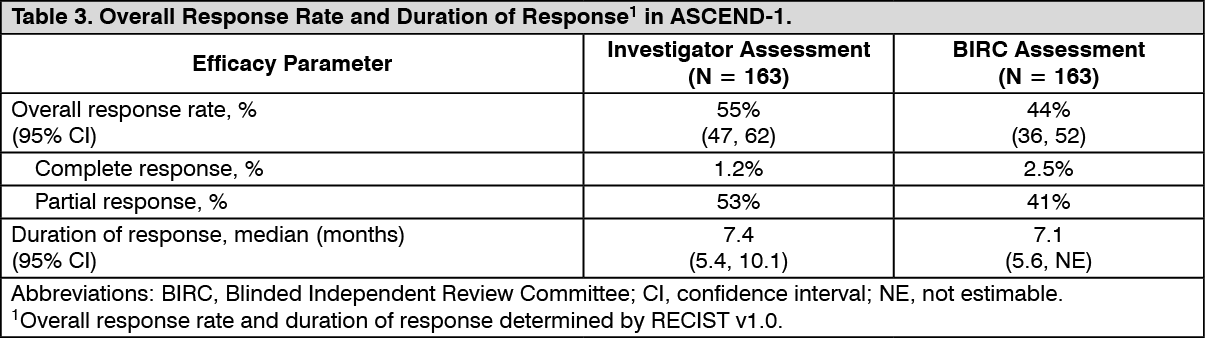 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image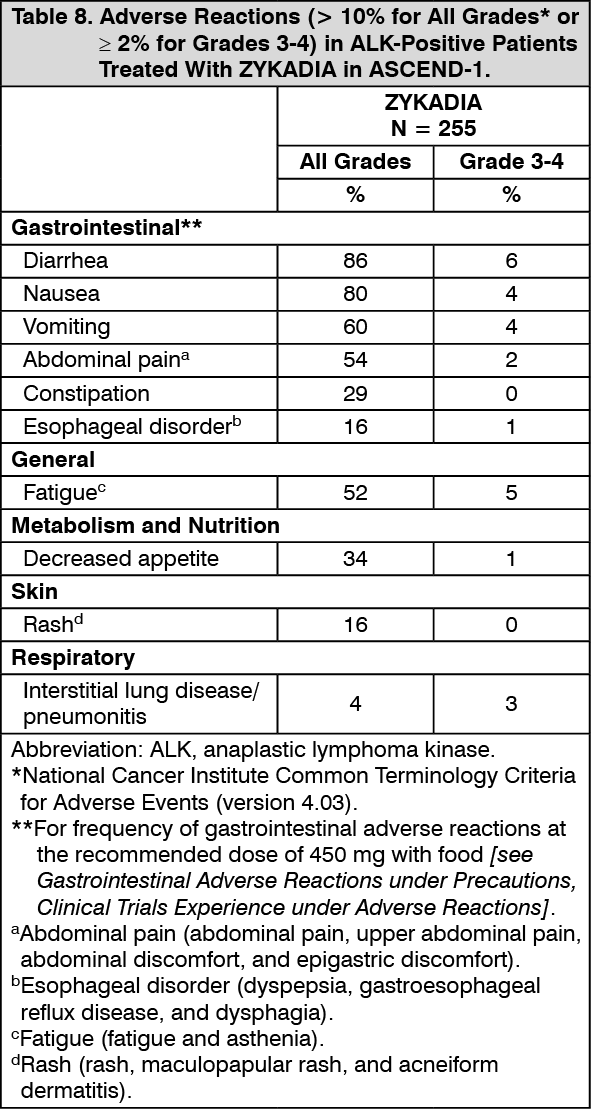 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image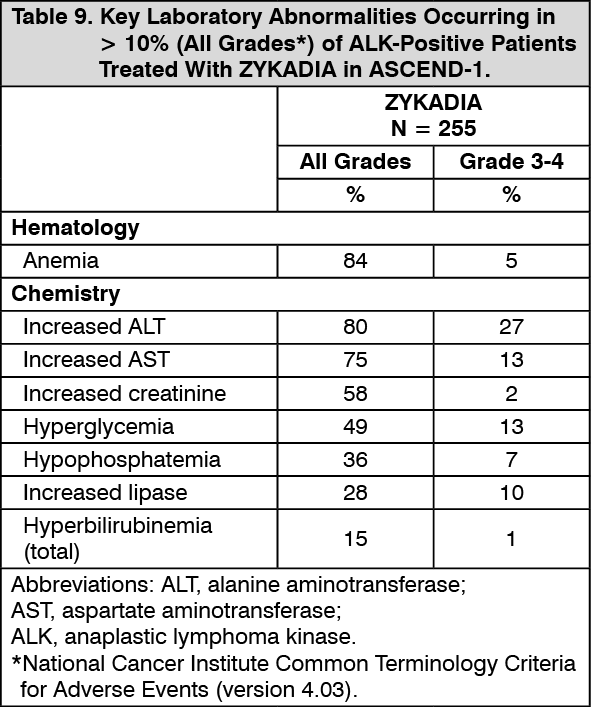 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
