Goserelin acetate (equivalent to 3.6 mg goserelin).
Excipients/Inactive Ingredients: Lactide/glycolide copolymer.
Pharmacotherapeutic Group: Gonadotropin releasing hormone analogues. ATC Code: L02AE03.
Pharmacology: Pharmacodynamics: Zoladex (D-Ser(But)6 Azgly10 LHRH) is a synthetic analogue of naturally occurring LHRH. On chronic administration Zoladex results in inhibition of pituitary LH secretion leading to a fall in serum testosterone concentrations in males and serum oestradiol concentrations in females. This effect is reversible on discontinuation of therapy. Initially, Zoladex, like other LHRH agonists, may transiently increase serum testosterone concentration in men and serum oestradiol concentration in women.
In men by around 21 days after the first depot injection, testosterone concentrations have fallen to within the castrate range and remain suppressed with continuous treatment every 28 days. This inhibition leads to prostate tumour regression and symptomatic improvement in the majority of patients.
In the management of patients with metastatic prostate cancer, Zoladex has been shown in comparative clinical trials to give similar survival outcomes to those obtained with surgical castrations.
In a combined analysis of 2 randomised controlled trials comparing bicalutamide 150 mg monotherapy versus castration (predominantly in the form of Zoladex), there was no significant difference in overall survival between bicalutamide-treated patients and castration-treated patients (hazard ratio = 1.05 [CI 0.81 to 1.36]) with locally advanced prostate cancer. However, equivalence of the two treatments could not be concluded statistically.
In comparative trials, Zoladex has been shown to improve disease-free survival and overall survival when used as an adjuvant therapy to radiotherapy in patients with high-risk localised (T1-T2 and PSA of at least 10 ng/mL or a Gleason score of at least 7), or locally advanced (T3-T4) prostate cancer. The optimum duration of adjuvant therapy has not been established; a comparative trial has shown that 3 years of adjuvant Zoladex gives significant survival improvement compared with radiotherapy alone. Neo-adjuvant Zoladex prior to radiotherapy has been shown to improve disease-free survival in patients with high risk localised or locally advanced prostate cancer.
After prostatectomy, in patients found to have extra-prostatic tumour spread, adjuvant Zoladex may improve disease-free survival periods, but there is no significant survival improvement unless patients have evidence of nodal involvement at time of surgery. Patients with pathologically staged locally advanced disease should have additional risk factors such as PSA of at least 10 ng/mL or a Gleason score of at least 7 before adjuvant Zoladex should be considered. There is no evidence of improved clinical outcomes with use of neoadjuvant Zoladex before radical prostatectomy.
In women serum oestradiol concentrations are suppressed by around 21 days after the first depot injection and, with continuous treatment every 28 days, remain suppressed at levels comparable with those observed in postmenopausal women. This suppression is associated with a response in hormone-dependent advanced breast cancer, uterine fibroids, endometriosis and suppression of follicular development within the ovary. It will produce endometrial thinning and will result in amenorrhoea in the majority of patients.
During treatment with LHRH analogues patients may enter the menopause. Rarely, some women do not resume menses on cessation of therapy.
Zoladex in combination with iron has been shown to induce amenorrhoea and improve haemoglobin concentrations and related haematological parameters in women with fibroids who are anaemic. The combination produced a mean haemoglobin concentration 1 g/dl above that achieved by iron therapy alone.
Pharmacokinetics: The bioavailability of Zoladex is almost complete. Administration of a depot every four weeks ensures that effective concentrations are maintained with no tissue accumulation. Zoladex is poorly protein bound and has a serum elimination half-life of two to four hours in subjects with normal renal function. The half-life is increased in patients with impaired renal function. For the compound given monthly in a depot formulation, this change will have minimal effect. Hence, no change in dosing is necessary in these patients. There is no significant change in pharmacokinetics in patients with hepatic failure.
Toxicology: Preclinical safety data: Following long-term repeated dosing with Zoladex, an increased incidence of benign pituitary tumours has been observed in male rats. Whilst this finding is similar to that previously noted in this species following surgical castration, any relevance to humans has not been established.
In mice, long term repeated dosing with multiples of the human dose produced histological changes in some regions of the digestive system manifested by pancreatic islet cell hyperplasia and a benign proliferative condition in the pyloric region of the stomach, also reported as a spontaneous lesion in this species. The clinical relevance of these findings is unknown.
Prostate cancer: Zoladex 3.6 mg is indicated in the management of prostate cancer suitable for hormonal manipulation.
Breast cancer: Zoladex 3.6 mg is indicated in the management of breast cancer in premenopausal and perimenopausal women suitable for hormonal manipulation.
Endometriosis: In the management of endometriosis, Zoladex 3.6 mg alleviates symptoms, including pain, and reduces the size and number of endometrial lesions.
Endometrial thinning: Zoladex 3.6 mg is indicated for the prethinning of the uterine endometrium prior to endometrial ablation or resection.
Uterine fibroids: In conjunction with iron therapy in the haematological improvement of anaemic patients with fibroids, prior to surgery.
Assisted reproduction: Pituitary downregulation in preparation for superovulation.
Posology: Adults: One 3.6 mg depot of Zoladex injected subcutaneously into the anterior abdominal wall every 28 days. No dosage adjustment is necessary for patients with renal or hepatic impairment, or in older people.
Endometriosis should be treated for a period of six months only, since at present there are no clinical data for longer treatment periods. Repeat courses should not be given due to concern about loss of bone mineral density. In patients receiving Zoladex for the treatment of endometriosis, the addition of hormone replacement therapy (a daily oestrogenic agent and a progestogenic agent) has been shown to reduce bone mineral density loss and vasomotor symptoms.
For use in endometrial thinning; four or eight weeks of treatment. The second depot may be required for the patient with a large uterus or to allow flexible surgical timing.
For women who are anaemic as a result of uterine fibroids: Zoladex 3.6 mg depot with supplementary iron may be administered for up to three months before surgery.
Assisted reproduction: Zoladex 3.6 mg is administered to downregulate the pituitary gland, as defined by serum oestradiol levels similar to those observed in the early follicular phase (approximately 150 pmol/l). This will usually take between 7 and 21 days.
When downregulation is achieved, superovulation (controlled ovarian stimulation) with gonadotrophin is commenced. The downregulation achieved with a depot agonist is more consistent suggesting that, in some cases, there may be an increased requirement for gonadotrophin. At the appropriate stage of follicular development, gonadotrophin is stopped and human chorionic gonadotrophin (hCG) is administered to induce ovulation. Treatment monitoring, oocyte retrieval and fertilisation techniques are performed according to the normal practice of the individual clinic.
Paediatric Population: Zoladex is not indicated for use in children.
Method of administration: For correct administration of Zoladex, see Patient Counselling Information.
The instruction card has to be read prior to administration.
Caution is needed when administering Zoladex into anterior abdominal wall due to the proximity of underlying inferior epigastric artery and its branches.
Extra care to be given to patients with a low BMI or who are receiving anticoagulation medication (see Precautions.)
Care should be taken to ensure injection is given subcutaneously, using the technique described in the instruction card. Do not penetrate into a blood vessel, muscle or peritoneum.
In the event of the need to surgically remove a Zoladex implant, it may be localised by ultrasound.
For special precautions for disposal and other handling see Special precautions for disposal and other handling under Cautions for Usage.
There is not much experience of overdosage in humans. In cases where Zoladex has been given before the planned time of administration, or when a bigger dose of Zoladex than originally planned has been given, no clinically significant undesirable effects have been observed.
Animal tests suggest that no effect other than the intended therapeutic effects on sex hormone concentrations and on the reproductive tract will be evident with higher doses of Zoladex. In case of overdosage, this condition should be managed symptomatically.
Hypersensitivity to the active substance, or to any excipients listed in Description.
Pregnancy and lactation (see Use in Pregnancy & Lactation).
There is an increased risk of incident depression (which may be severe) in patients undergoing treatment with GnRH agonists, such as Goserelin. Patients should be informed accordingly and treated as appropriate if symptoms occur.
Androgen deprivation therapy may prolong the QT interval.
In patients with a history of or risk factors for QT prolongation and in patients receiving concomitant medicinal products that might prolong the QT interval (see Interactions) physicians should assess the benefit risk ratio including the potential for Torsade de pointes prior to initiating Zoladex.
Injection site injury has been reported with Zoladex, including events of pain, haematoma, haemorrhage and vascular injury. Monitor affected patients for signs or symptoms of abdominal haemorrhage. In very rare cases, administration error resulted in vascular injury and haemorrhagic shock requiring blood transfusions and surgical intervention. Extra care should be taken when administering Zoladex to patients with a low BMI and/or receiving full anticoagulation medications (see Dosage & Administration).
Males: The use of Zoladex in men at particular risk of developing ureteric obstruction or spinal cord compression should be considered carefully, and the patients monitored closely during the first month of therapy. If spinal cord compression or renal impairment due to ureteric obstruction are present or develop, specific standard treatment of these complications should be instituted.
Consideration should be given to the initial use of an anti-androgen (e.g. cyproterone acetate 300 mg daily for three days before and three weeks after commencement of Zoladex) at the start of LHRH analogue therapy since this has been reported to prevent the possible sequelae of the initial rise in serum testosterone.
The use of LHRH agonists may cause a reduction in bone mineral density. In men, preliminary data suggest that the use of a bisphosphonate in combination with an LHRH agonist may reduce bone mineral loss. Particular caution is necessary in patients with additional risk factors for osteoporosis (e.g. chronic alcohol abusers, smokers, long-term therapy with anticonvulsants or corticosteroids, family history of osteoporosis).
Patients with known depression and patients with hypertension should be monitored carefully.
Reduction in glucose tolerance has been observed in men receiving LHRH agonists. This may manifest as diabetes or loss of glycaemic control in patients with pre-existing diabetes mellitus. Thus, monitoring blood glucose levels should be considered.
Myocardial infarction and cardiac failure were observed in a pharmacoepidemiology study of LHRH agonists used in the treatment of prostate cancer. The risk appears to be increased when used in combination with anti-androgens.
Females: Breast cancer indication: Reduced bone mineral density: The use of LHRH agonists may cause reduction in bone mineral density. Following two years treatment for early breast cancer, the average loss of bone mineral density was 6.2% and 11.5% at the femoral neck and lumbar spine respectively. This loss has been shown to be partially reversible at the one year off treatment follow-up with recovery to 3.4% and 6.4% relative to baseline at the femoral neck and lumbar spine respectively, although this recovery is based on very limited data. In the majority of women, currently available data suggest that recovery of bone loss occurs after cessation of therapy.
Preliminary data suggest that the use of Zoladex in combination with tamoxifen in patients with breast cancer may reduce bone mineral loss.
Benign indication: Loss of bone mineral density: The use of LHRH agonists is likely to cause reduction in bone mineral density averaging 1% per month during a six month treatment period. Every 10% reduction in bone mineral density is linked with about a two to three times increased fracture risk. In the majority of women, currently available data suggest that recovery of bone loss occurs after cessation of therapy.
In patients receiving Zoladex for the treatment of endometriosis, the addition of hormone replacement therapy has been shown to reduce bone mineral density loss and vasomotor symptoms.
No specific data is available for patients with established osteoporosis or with risk factors for osteoporosis (e.g. chronic alcohol abusers, smokers, long-term therapy with drugs that reduce bone mineral density, e.g. anticonvulsants or corticosteroids, family history of osteoporosis, malnutrition, e.g. anorexia nervosa). Since reduction in bone mineral density is likely to be more detrimental in these patients, treatment with Zoladex should be considered on an individual basis and only be initiated if the benefits of treatment outweigh the risks following a very careful appraisal.
Consideration should be given to additional measures in order to counteract loss of bone mineral density.
Withdrawal bleeding: During early treatment with Zoladex some women may experience vaginal bleeding of variable duration and intensity. If vaginal bleeding occurs it is usually in the first month after starting treatment. Such bleeding probably represents oestrogen withdrawal bleeding and is expected to stop spontaneously. If bleeding continues, the reason should be investigated.
There are no clinical data on the effects of treating benign gynaecological conditions with Zoladex for periods in excess of six months.
The use of Zoladex may cause an increase in cervical resistance and care should be taken when dilating the cervix.
Zoladex should only be administered as part of a regimen for assisted reproduction under the supervision of a specialist experienced in the area.
As with other LHRH agonists, there have been reports of ovarian hyperstimulation syndrome (OHSS), associated with the use of Zoladex 3.6 mg in combination with gonadotrophin. The stimulation cycle should be monitored carefully to identify patients at risk of developing OHSS. If OHSS risk is present, human chorionic gonadotrophin (hCG) should be withheld, if possible.
It is recommended that Zoladex is used with caution in fertilisation treatment of patients with polycystic ovarian syndrome as follicle recruitment may be increased.
Fertile women should use non-hormonal contraceptive methods during treatment with Zoladex and until reset of menstruation following discontinuation of treatment with Zoladex.
Patients with known depression and patients with hypertension should be monitored carefully.
Treatment with Zoladex may lead to positive reactions in anti-doping tests.
Effect on ability to drive or operate machinery: Zoladex has no or negligible influence on the ability to drive and use machines.
Use in Children: Zoladex is not indicated for use in children, as safety and efficacy have not been established in this patient group.
Pregnancy: Zoladex should not be used during pregnancy since concurrent use of LHRH agonists is associated with a theoretical risk of abortion or foetal abnormality. Prior to treatment, potentially fertile women should be examined carefully to exclude pregnancy. Non-hormonal methods of contraception should be employed during therapy until menses resume (see also warning concerning the time to return of menses in Precautions).
Pregnancy should be excluded before Zoladex is used for fertilisation treatment. When Zoladex is used in this setting, there is no clinical evidence to suggest a causal connection between Zoladex and any subsequent abnormalities of oocyte development or pregnancy or outcome.
Breast-feeding: The use of Zoladex during breast-feeding is not recommended.
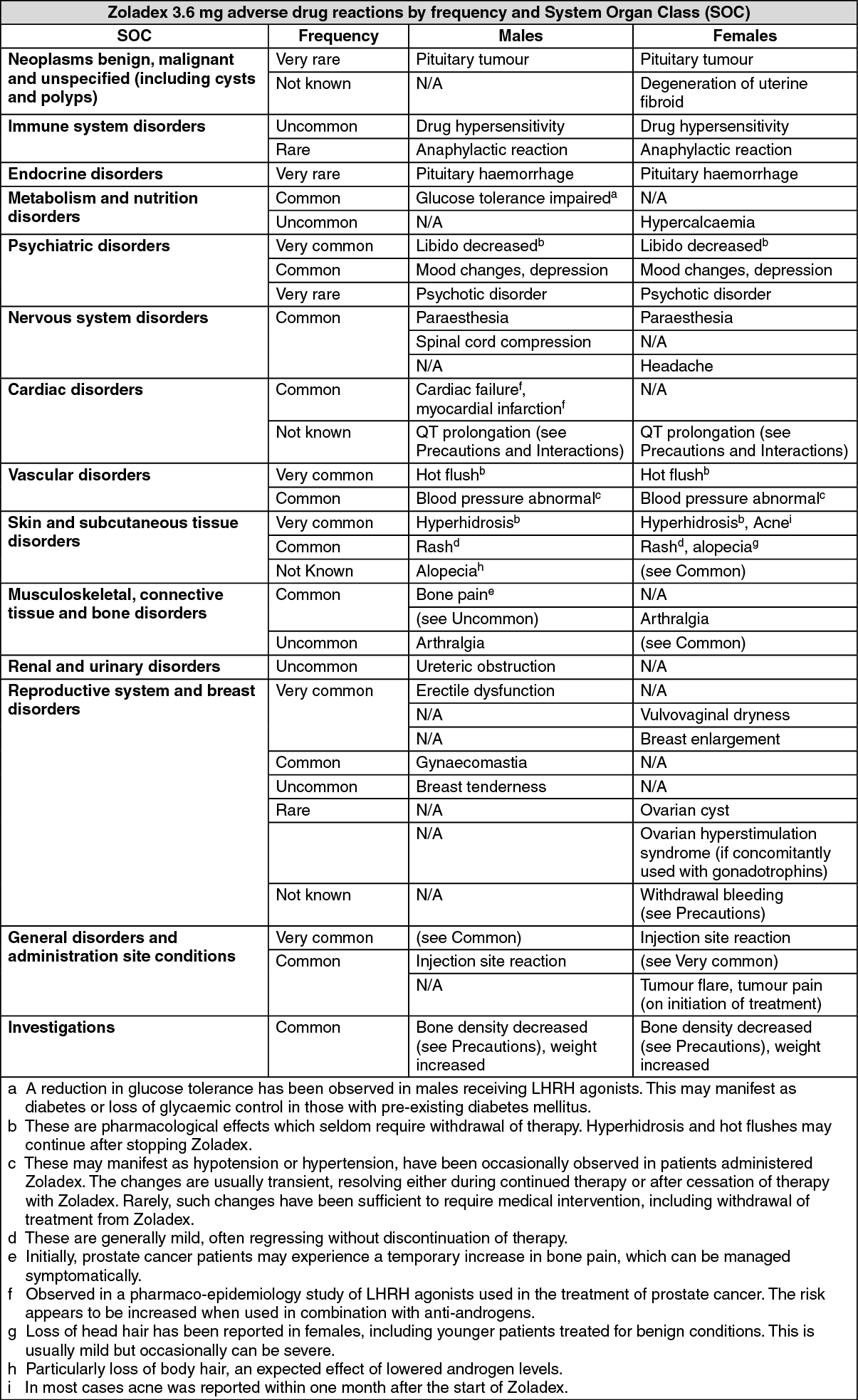
The following frequency categories for adverse drug reactions (ADRs) were calculated based on reports from Zoladex clinical trials and post-marketing sources.
The most commonly observed adverse reactions include hot flushes, sweating and injection site reactions.
The following convention has been used for classification of frequency: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1/1,000), Very rare (<1/10,000) and Not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Post-marketing experience:
Click on icon to see table/diagram/image
Post-marketing experience: A small number of cases of changes in blood count, hepatic dysfunction, pulmonary embolism and interstitial pneumonia have been reported in connection with Zoladex.
In addition, the following adverse drug reactions have been reported in women treated for benign gynaecological indications: Acne, change of body hairs, dry skin, weight gain, increase in serum cholesterol, ovarian hyperstimulation syndrome (if concomitantly used with gonadotropins), vaginitis, vaginal discharge, nervousness, sleep disorder, tiredness, peripheral oedema, myalgias, cramp in the calves, nausea, vomiting, diarrhoea, constipation, abdominal complaints, alterations of voice. Initially, breast cancer patients may experience a temporary increase in signs and symptoms, which can be managed symptomatically.
Rarely, breast cancer patients with metastases have developed hypercalcaemia on initiation of therapy. In the presence of symptoms indicative of hypercalcaemia (e.g. thirst), hypercalcaemia should be excluded.
Rarely, some women may enter the menopause during treatment with LHRH analogues and not resume menses on cessation of therapy. Whether this is an effect of Zoladex treatment or a reflection of their gynaecological condition is not known.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product.
Since androgen deprivation treatment may prolong the QT interval, the concomitant use of Zoladex with medicinal products known to prolong the QT interval or medicinal products able to induce Torsade de pointes such as class IA (e.g. quinidine, disopyramide) or class III (e.g. amiodarone, sotalol, dofetilide, ibutilide) antiarrhythmic medicinal products, methadone, moxifloxacin, antipsychotics, etc. should be carefully evaluated (see Precautions).
Incompatibilities: None known.
Special precautions for disposal and other handling: Use as directed by the prescriber. Use only if pouch is undamaged. Use immediately after opening pouch. Dispose of the syringe in an approved sharps collector.
L02AE03 - goserelin ; Belongs to the class of gonadotropin releasing hormone analogues. Used in endocrine therapy.
Zoladex depot inj 3.6 mg
1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
