Pharmacotherapeutic group: Antibacterials for systemic use, other cephalosporins.
ATC code: J01DI02.
The active moiety after ceftaroline fosamil administration is ceftaroline.
Pharmacology: Pharmacodynamics: Mechanism of action: Ceftaroline is a cephalosporin with activity against Gram-positive and Gram-negative bacteria.
In-vitro studies have shown that ceftaroline is bactericidal, due to inhibition of bacterial cell wall synthesis by binding to penicillin binding proteins (PBPs). Ceftaroline is also active against methicillin-resistant
Staphylococcus aureus (MRSA) and penicillin non-susceptible
Streptococcus pneumoniae (PNSP) due to its high affinity for the altered PBPs found in these organisms.
Pharmacokinetic/pharmacodynamic relationship: As with other beta-lactam antimicrobial agents, the percent time above the minimum inhibitory concentration (MIC) of the infecting organism over the dosing interval (%T >MIC) has been shown to best correlate with the antimicrobial activities for ceftaroline.
Resistance: Ceftaroline is not active against strains of
Enterobacterales producing extended-spectrum beta-lactamases (ESBLs) from the TEM, SHV or CTX-M families, serine carbapenemases (such as KPC), class B metallo-beta-lactamases or class C (AmpC cephalosporinases).
Organisms that express these enzymes and which are therefore resistant to ceftaroline occur at very variable rates between countries and between healthcare facilities within countries. If ceftaroline is commenced before susceptibility test results are available then local information on the risk of encountering organisms that express these enzymes should be taken into consideration. Resistance may also be mediated by bacterial impermeability or drug efflux pump mechanisms. One or more of these mechanisms may co-exist in a single bacterial isolate.
Cross-resistance: Unlike other cephalosporins, ceftaroline is active against most MRSA and PNSP due to its ability to bind to the altered PBPs in these organisms that commonly confer insusceptibility to other beta-lactam agents.
Interaction with other antibacterial agents: In vitro studies have not demonstrated any antagonism between ceftaroline in combination with other commonly used antibacterial agents (e.g. amikacin, azithromycin, aztreonam, daptomycin, levofloxacin, linezolid, meropenem, tigecycline, and vancomycin).
Susceptibility testing: The prevalence of acquired resistance may vary geographically and with time for selected species. Local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent is questionable.
The susceptibility to ceftaroline of a given clinical isolate should be determined by standard methods. Interpretations of test results should be made in accordance with local infectious diseases and clinical microbiology guidelines.
Clinical efficacy against specific pathogens: Efficacy has been demonstrated in clinical studies against the pathogens listed under each indication that were susceptible to ceftaroline
in vitro.
Complicated skin and soft tissue infections: Gram-positive organisms:
Staphylococcus aureus (including methicillin-resistant strains),
Streptococcus pyogenes, Streptococcus agalactiae, Streptococcus anginosus (includes
S. anginosus, S. intermedius, and
S. constellatus),
Streptococcus dysgalactiae.
Gram-negative organisms:
Escherichia coli, Klebsiella pneumoniae, Klebsiella oxytoca, Morganella morganii.
Community-acquired pneumonia: Gram-positive organisms:
Streptococcus pneumoniae, Staphylococcus aureus (methicillin-susceptible strains only).
Gram-negative organisms:
Escherichia coli, Haemophilus influenzae, Haemophilus parainfluenzae, Klebsiella pneumoniae.
Antibacterial activity against other relevant pathogens: Clinical efficacy has not been established against the following pathogens although
in vitro studies suggest that they would be susceptible to ceftaroline in the absence of acquired mechanisms of resistance: Anaerobic Gram-positive organisms:
Peptostreptococcus species.
Anaerobic Gram-negative organisms:
Fusobacterium species.
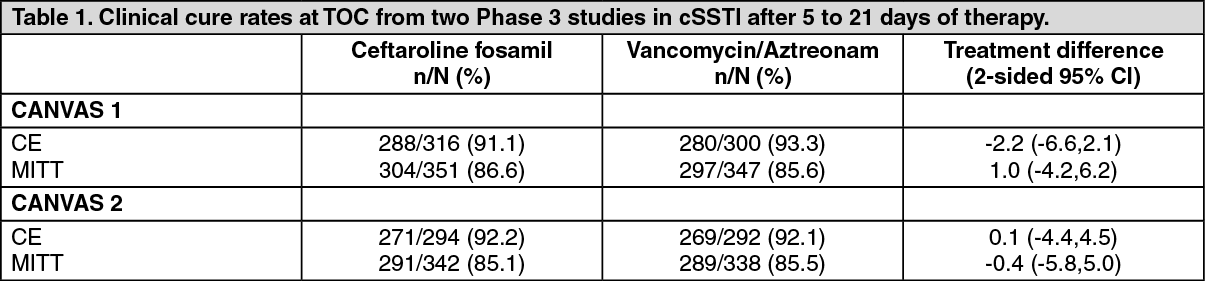
Clinical efficacy and safety: Complicated skin and soft tissue infections: A total of 1396 adults with documented complicated skin and soft tissue infections were enrolled in two identical randomised, multi-centre, multinational, double-blind studies (CANVAS 1 and CANVAS 2) comparing ceftaroline fosamil (600 mg administered intravenously over 60 minutes every 12 hours) to vancomycin plus aztreonam (1 g vancomycin administered intravenously over 60 minutes followed by 1 g aztreonam administered intravenously over 60 minutes every 12 hours). Patients with deep/extensive cellulitis, a major abscess, a wound infection (surgical or traumatic), infected bites, burns or ulcers, or any lower extremity infection in patients with either pre-existing diabetes mellitus or peripheral vascular disease, were eligible for the studies. Treatment duration was 5 to 21 days. The modified intent-to-treat (MITT) population included all patients who received any amount of study drug according to their randomised treatment group. The clinically evaluable (CE) population included patients in the MITT population with sufficient adherence to the protocol.
The primary efficacy endpoint was the clinical response at the Test of Cure (TOC) visit in the co-primary populations of the CE and MITT patients in the table as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Clinical cure rates at TOC by pathogen in the microbiologically evaluable patients are presented as follows. (See Table 2.)
Click on icon to see table/diagram/image
Complicated skin and soft tissue infections with systemic inflammatory response or underlying comorbidities (COVERS): A total of 772 adults with cSSTI with evidence of systemic inflammation and/or underlying comorbidities were enrolled in a randomised, multi-centre, double-blind study (COVERS) comparing ceftaroline fosamil (600 mg administered intravenously over 120 minutes every 8 hours) to vancomycin plus aztreonam. The MITT population included all patients who received any amount of study drug according to their randomised treatment group; patients had an average area of lesion size of 400 cm
2, 40% had SIRS, and 61% had elevated CRP (>50 mg/L). Treatment duration was 5 to 14 days. The CE population included patients in the MITT population with sufficient adherence to the protocol. The primary endpoint was clinical cure rate at the TOC visit in both the MITT and CE populations. (See Table 3.)
Click on icon to see table/diagram/image
Clinical cure rates at TOC by pathogen in the microbiologically evaluable patients are presented as follows. (See Table 4.)
Click on icon to see table/diagram/image
Paediatric studies: The cSSTI paediatric trial was a randomized, parallel-group, active-controlled trial in paediatric patients 2 months to < 18 years of age.
A total of 163 children from 2 months to < 18 years of age with clinically documented cSSTI were enrolled in a randomized, multi-centre, multinational, parallel-group, active controlled trial comparing ceftaroline fosamil to vancomycin or cefazolin (each with optional aztreonam). Treatment duration was 5 to 14 days. A switch to oral therapy with either cephalexin, clindamycin, or linezolid after Study Day 3 was allowed. The MITT population included all patients who received any amount of study drug with a confirmed diagnosis of cSSTI.
The primary objective was to evaluate the safety and tolerability of ceftaroline fosamil. The study was not powered for comparative inferential efficacy analysis, and no efficacy endpoint was identified as primary.
Clinical cure rates at test of cure (8 to 15 days after the end of therapy) in the MITT population were 94.4% (101/107) for ceftaroline fosamil and 86.5% (45/52) for the comparator, with a treatment difference of 7.9 (95% CI -1.2, 20.2).
Community-acquired pneumonia: A total of 1240 adults with a diagnosis of CAP were enrolled in two randomized, multi-centre, multinational, double-blind studies (FOCUS 1 and FOCUS 2) comparing ceftaroline fosamil (600 mg administered intravenously over 60 minutes every 12 hours) to ceftriaxone (1 g ceftriaxone administered intravenously over 30 minutes every 24 hours). The studies were identical except in one respect, in FOCUS 1 both treatment groups received 2 doses of oral clarithromycin (500 mg every 12 hours) as adjunctive therapy starting on Day 1. No adjunctive macrolide therapy was used in FOCUS 2. Patients with new or progressive pulmonary infiltrate(s) on chest radiography with clinical signs and symptoms consistent with CAP with the need for hospitalisation and intravenous therapy were enrolled in the studies. Treatment duration was 5 to 7 days. The modified intent-to-treat efficacy (MITTE) population included all patients who received any amount of study drug according to their randomized treatment group and were in PORT Risk Class III or IV. The clinically evaluable (CE) population included patients in the MITTE population with sufficient adherence to the protocol.
The primary efficacy endpoint was the clinical response at the Test of Cure (TOC) visit in the co-primary populations of the CE and MITTE populations in the table as follows. (See Table 5.)
Click on icon to see table/diagram/image
Clinical cure rates at TOC by pathogens in the microbiologically evaluable patients are presented in the table as follows. (See Table 6.)
Click on icon to see table/diagram/image
Asia CAP study: A total of 771 adults with a diagnosis of CAP were enrolled in a randomized, multi-centre, double-blind study in Asia comparing ceftaroline fosamil (600 mg administered intravenously over 60 minutes every 12 hours) to ceftriaxone (2 g administered intravenously over 30 minutes every 24 hours). Treatment duration was 5 to 7 days. The primary objective was to determine the non-inferiority in the clinical cure rate of ceftaroline treatment compared with that of ceftriaxone treatment at the TOC visit in the CE population of adult hospitalized patients with CAP (lower boundary of the 95% confidence interval for the difference in response rate [ceftaroline - ceftriaxone] greater than -10%).
The non-inferiority of ceftaroline 600 mg versus ceftriaxone 2 g was demonstrated in both the CE and MITT populations (Tables 7 and 8). Furthermore, based on the pre-defined criteria (lower boundary of the 95% confidence interval for the difference in response rate greater than 0%), the superiority of ceftaroline 600 mg versus ceftriaxone 2 g was demonstrated in adult patients with PORT Risk Class III/IV CAP in Asia. (See Tables 7, 8 and 9.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Paediatric studies: The CAP paediatric trial was a randomized, parallel-group, active controlled trial in paediatric patients 2 months to <18 years of age.
A total of 161 children with a diagnosis of CAP were enrolled in a randomized, multi-centre, multinational, active controlled trial comparing ceftaroline fosamil with ceftriaxone. Patients with new or progressive pulmonary infiltrate(s) on chest radiography and signs and symptoms consistent with CAP including acute onset or worsening symptoms of cough, tachypnoea, sputum production, grunting, chest pain, cyanosis, or increased work of breathing with the need for hospitalization and IV therapy were enrolled in the trial. Treatment duration was 5 to 14 days. A switch to oral therapy with amoxicillin clavulanate was allowed after Study Day 3. The MITT population included all randomized patients who received any amount of study drug with a confirmed diagnosis of CAP.
The primary objective was to evaluate the safety and tolerability of ceftaroline fosamil. The study was not powered for comparative inferential efficacy analysis, and no efficacy endpoint was identified as primary.
Clinical cure rates at test of cure (8 to 15 days after final dose of study drug) in the MITT population were 87.9% (94/107) for ceftaroline fosamil and 88.9% (32/36) for the comparator, with a treatment difference of -1.0 (95% CI -11.5, 14.1).
Pharmacokinetics: The C
max and AUC of ceftaroline increase approximately in proportion to dose within the single dose range of 50 to 1000 mg. No appreciable accumulation of ceftaroline is observed following multiple intravenous infusions of 600 mg every 8 or 12 hours in healthy adults with normal renal function.
The systemic exposure (AUC), T
½, and clearance of ceftaroline were similar following administration of 600 mg ceftaroline fosamil in a volume of 50 mL to healthy adult subjects every 8 hours for 5 days as 5 minute or 60 minute infusions, and the T
max of ceftaroline occurred about 5 minutes after the end of the ceftaroline fosamil infusion for both infusion durations. The mean (SD) C
max of ceftaroline was 32.5 (4.82) mg/L for the 5 minute infusion duration (n = 11) and 17.4 (3.87) mg/L for the 60 minute infusion duration (n = 12).
Distribution: The plasma protein binding of ceftaroline is low (approximately 20%) and ceftaroline is not distributed into erythrocytes. The median steady-state volume of distribution of ceftaroline in healthy adult males following a single 600 mg intravenous dose of radiolabeled ceftaroline fosamil was 20.3 L, similar to the volume of extracellular fluid.
Metabolism: Ceftaroline fosamil (prodrug) is converted into the active ceftaroline in plasma by phosphatase enzymes and concentrations of the prodrug are measurable in plasma primarily during intravenous infusion. Hydrolysis of the beta-lactam ring of ceftaroline occurs to form the microbiologically inactive, open-ring metabolite, ceftaroline M-1. The mean plasma ceftaroline M-1 to ceftaroline AUC ratio following a single 600 mg intravenous infusion of ceftaroline fosamil in healthy subjects is approximately 20-30%.
In pooled human liver microsomes, metabolic turnover was low for ceftaroline, indicating that ceftaroline is not metabolised by hepatic CYP450 enzymes.
Excretion: Ceftaroline is primarily eliminated by the kidneys. Renal clearance of ceftaroline is approximately equal, or slightly lower than the glomerular filtration rate in the kidney, and
in vitro transporter studies indicate that active secretion does not contribute to the renal elimination of ceftaroline.
The mean terminal elimination half-life of ceftaroline in healthy adults is approximately 2.5 hours.
Following the administration of a single 600 mg intravenous dose of radiolabeled ceftaroline fosamil to healthy male adults, approximately 88% of radioactivity was recovered in urine and 6% in faeces.
Special populations: Patients with renal impairment: Dosage adjustment is required in adults, adolescents and children with CrCL ≤50 mL/min (see Dosage & Administration).
There is insufficient information to recommend dosage adjustments in adolescents with ESRD aged from 12 to <18 years and with bodyweight <33 kg and in children with ESRD aged from 2 to <12 years. There is insufficient information to recommend dosage adjustments in paediatric patients aged <2 years with moderate or severe renal impairment or ESRD.
Patients with hepatic impairment: The pharmacokinetics of ceftaroline in patients with hepatic impairment have not been established. As ceftaroline does not appear to undergo significant hepatic metabolism, the systemic clearance of ceftaroline is not expected to be significantly affected by hepatic impairment. Therefore, no dosage adjustment is recommended for patients with hepatic impairment.
Elderly patients: Following administration of a single 600 mg intravenous dose of ceftaroline fosamil, the pharmacokinetics of ceftaroline was similar between healthy elderly subjects (≥65 years of age), and healthy young adult subjects (18-45 years of age). There was a 33% increase in AUC
0-∞ in the elderly that was mainly attributable to age-related changes in renal function. Ceftaroline fosamil dose adjustment is not required in elderly patients with creatinine clearance above 50 mL/min.
Paediatric patients: Dose adjustments are required for
neonates, infants, children and adolescents with bodyweight <33 kg (see Dosage & Administration).
Gender: The pharmacokinetics of ceftaroline was similar between males and females. No dose adjustment is required based on gender.
Race: Race was evaluated as a covariate in a population pharmacokinetic analysis on data from the clinical studies. No significant differences in ceftaroline pharmacokinetics were observed in Caucasian, Hispanic, Black, Asian or other subjects. No dosage adjustment is recommended based on race.
Toxicology: Preclinical safety data: The kidney was the primary target organ of toxicity in both the monkey and rat. Histopathologic findings included pigment deposition and inflammation of the tubular epithelium. Renal changes were not reversible but were reduced in severity following a 4 week recovery period.
Convulsions have been observed at relatively high exposures during single and multi-dose studies in both the rat and monkey (≥7 times to the estimated C
max level of a 600 mg twice a day).
Other important toxicologic findings noted in the rat and monkey included histopathologic changes in the bladder and spleen.
Genetic toxicology: Ceftaroline fosamil and ceftaroline were clastogenic in an
in vitro chromosomal aberration assay, however there was no evidence of mutagenic activity in an Ames, mouse lymphoma and unscheduled DNA synthesis assay. Furthermore,
in vivo micronucleus assays in rat and mouse were negative. Carcinogenicity studies have not been conducted.
Reproductive toxicology: Reproductive studies in pregnant rabbits resulted in an increased foetal incidence of angulated hyoid alae, a common skeletal variation in rabbit foetuses, at exposures similar to 600 mg twice daily in humans. In the rat, no adverse effects were observed on embryofoetal development, fertility or postnatal development.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image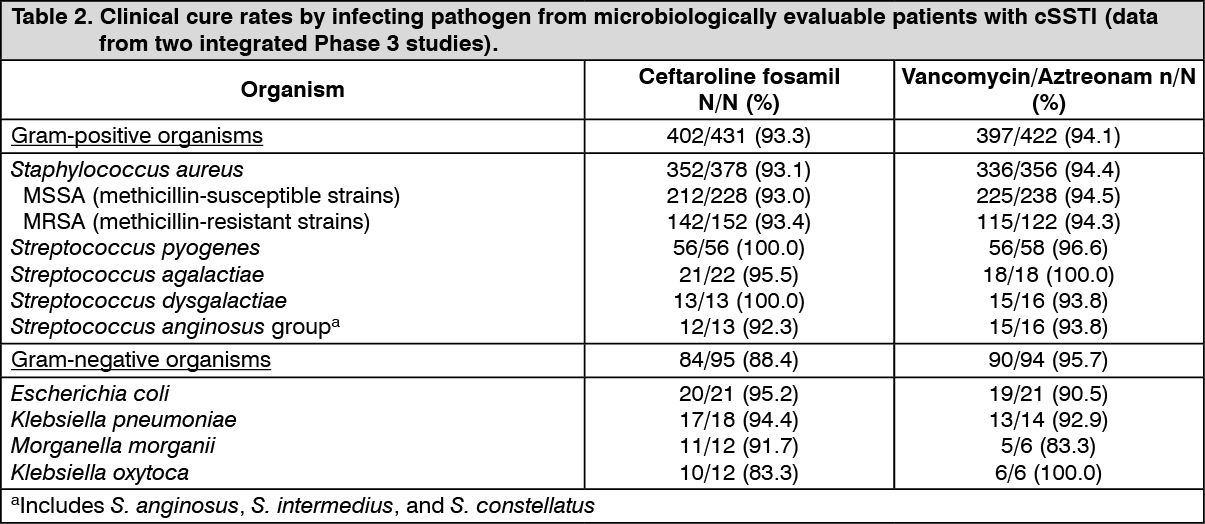 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image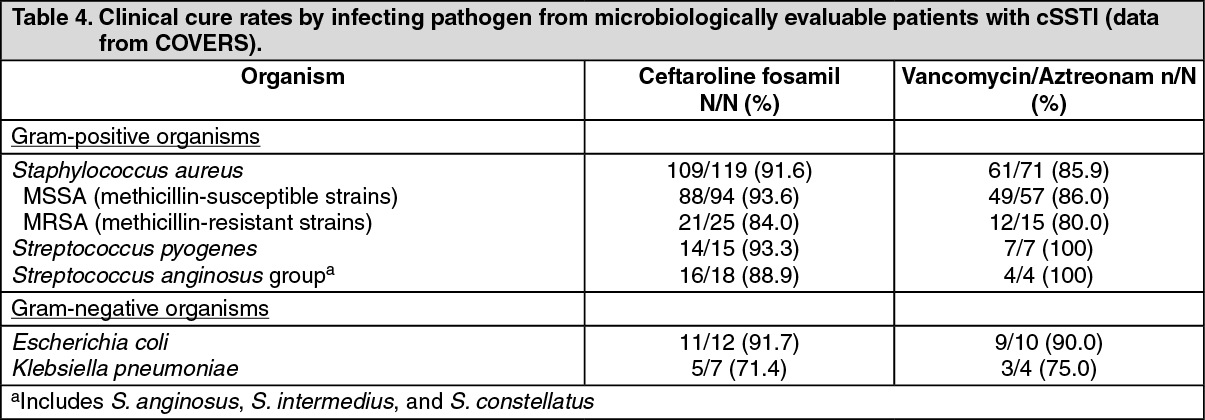 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image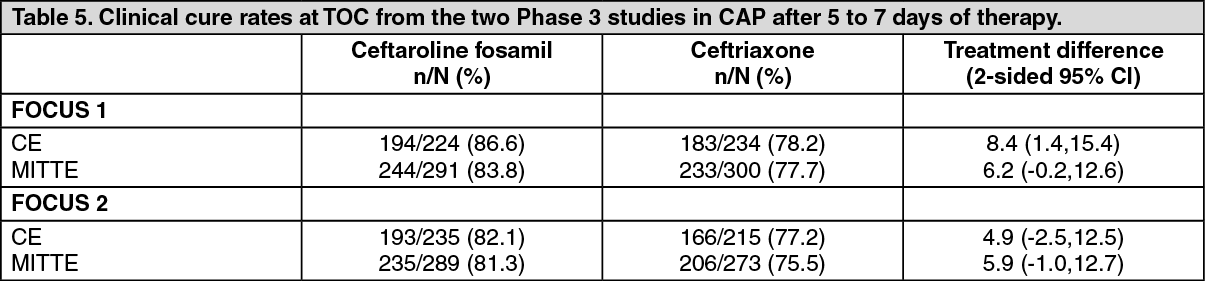 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image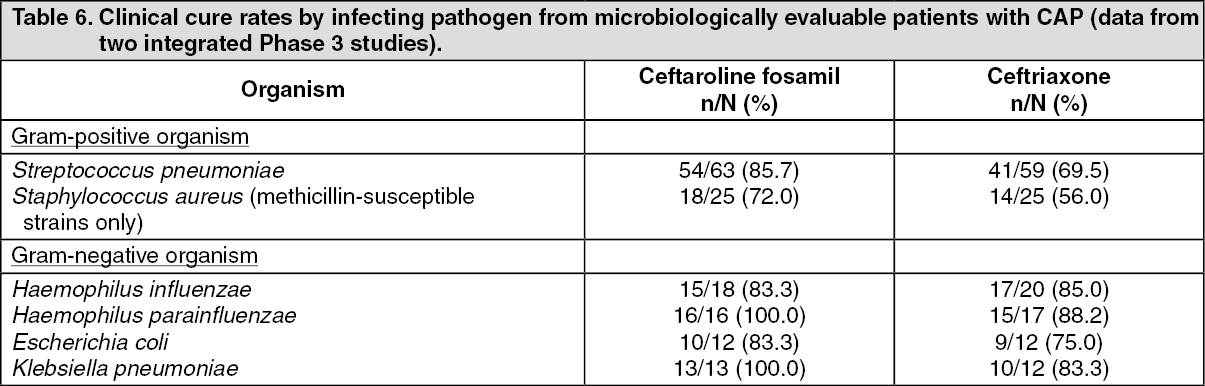 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image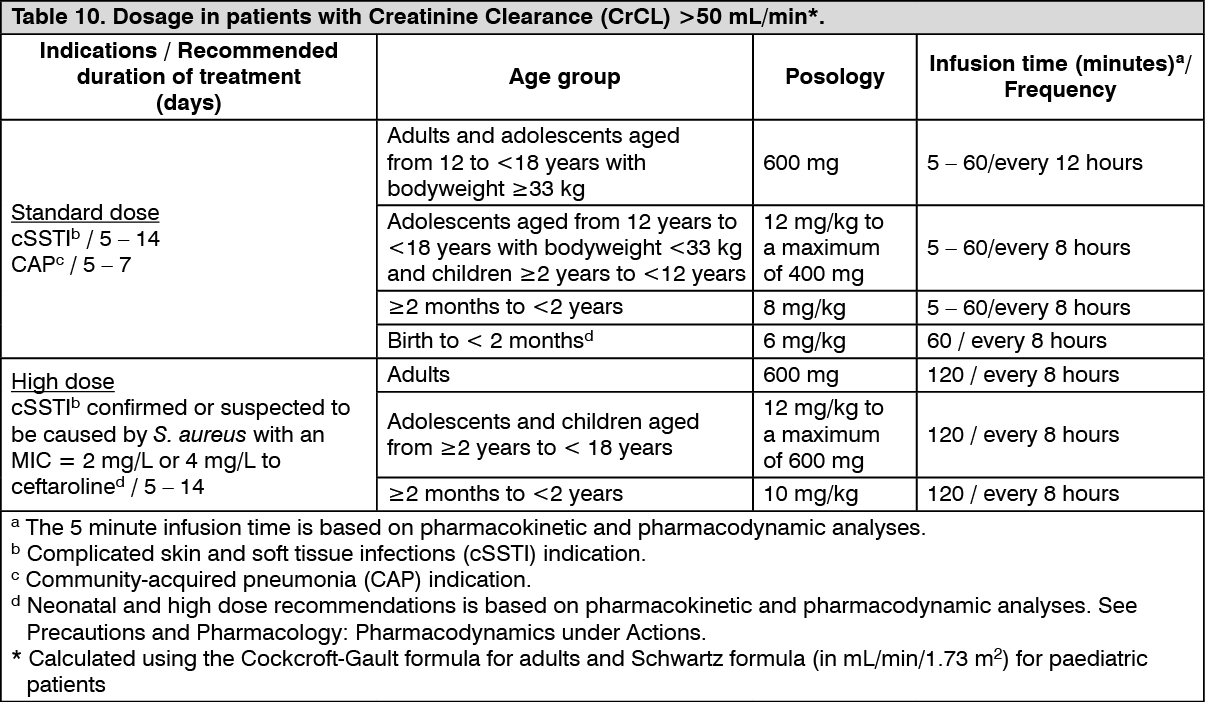 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image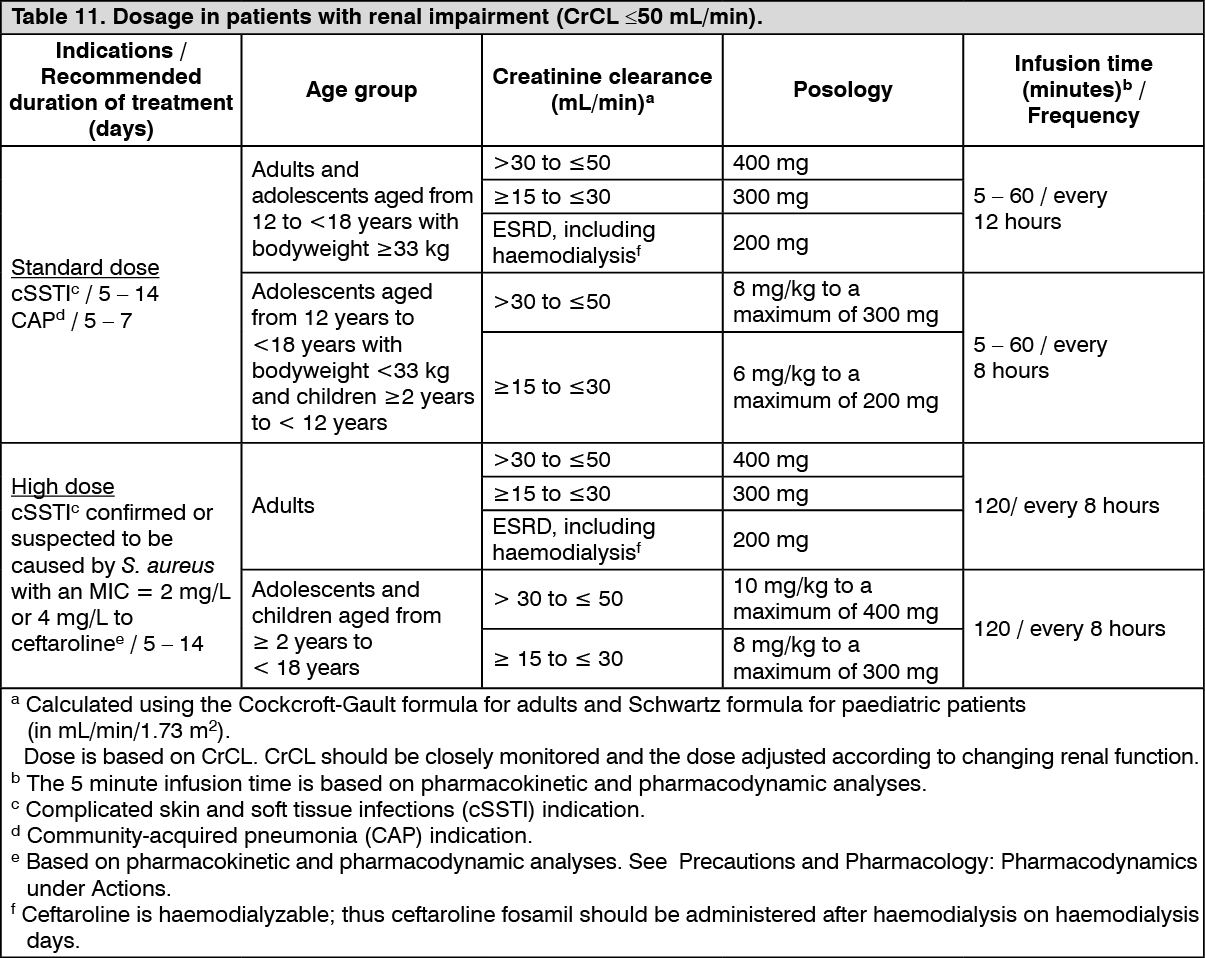 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image 600 mgc466b0d5-5aa4-403d-872e-ae2a00cc6238.GIF)

 Sign Out
Sign Out
