


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Abacavir is a nucleoside analogue reverse transcriptase inhibitor. It is a potent selective inhibitor of HIV-1 and HIV-2 including HIV-1 isolates with reduced susceptibility to zidovudine, lamivudine, zalcitabine, didanosine or nevirapine. Abacavir is metabolised intracellularly to the active moiety, carbovir 5'- triphosphate (TP). In vitro studies have demonstrated that its mechanism of action in relation to HIV is inhibition of the HIV reverse transcriptase enzyme, an event which results in chain termination and interruption of the viral replication cycle. The antiviral activity of abacavir in cell culture was not antagonized when combined with the nucleoside reverse transcriptase inhibitors (NRTIs) didanosine, emtricitabine, lamivudine, stavudine, tenofovir, zalcitabine or zidovudine, the non-nucleoside reverse transcriptase inhibitor (NNRTI) nevirapine, or the protease inhibitor (PI) amprenavir.
In a study of 20 HIV-infected patients receiving ZIAGEN 300 mg twice daily, with only one 300 mg dose taken prior to the 24 hours sampling period, the geometric mean terminal carbovir-TP intracellular half-life at steady-state was 20.6 hours, compared to the geometric mean abacavir plasma half-life in this study of 2.6 hours. The steady state pharmacokinetic properties of ZIAGEN 600 mg once daily was compared to ZIAGEN 300 mg twice daily in a crossover study in 27 HIV-infected patients. Intracellular carbovir triphosphate exposures in peripheral blood mononuclear cells were higher for ZIAGEN 600 mg once daily with respect to AUC24,ss (32 %, higher), Cmax 24,ss (99% higher) and trough values (18% higher), compared to the 300 mg twice daily regimen. These data support the use of ZIAGEN 600 mg once daily for the treatment of HIV infected patients. Additionally, the efficacy and safety of ZIAGEN given once daily has been demonstrated in a pivotal clinical study (CNA30021- see Pharmacology: Pharmacodynamics: Clinical Studies under Actions).
Abacavir-resistant isolates of HIV-1 have been selected in vitro and are associated with specific genotypic changes in the reverse transcriptase (RT) codon region (codons M184V, K65R, L74V and Y115F). Viral resistance to abacavir develops relatively slowly in vitro and in vivo, requiring multiple mutations to reach an eight-fold increase in IC50 over wild-type virus, which may be a clinically relevant level.
Isolates resistant to abacavir may also show reduced sensitivity to lamivudine, zalcitabine and/or didanosine, but remain sensitive to zidovudine and stavudine. Cross resistance between abacavir and protease inhibitors or non nucleoside reverse transcriptase inhibitors is unlikely. Treatment failure following initial therapy with abacavir, lamivudine and zidovudine is mainly associated with the M184V alone, thus maintaining many therapeutic options for a second line regimen.
Abacavir penetrates the cerebrospinal fluid (CSF) (see Pharmacology: Pharmacokinetics under Actions), and has been shown to reduce HIV-1 RNA levels in the CSF. In combination with other antiretrovirals it may have a role in the prevention of HIV related neurological complications, and may delay the development of resistance in this sanctuary site.
Clinical Studies: In a double-blind clinical study over 48 weeks in treatment naive adult patients, the combination of abacavir, lamivudine and zidovudine showed an equivalent antiviral effect to the combination with indinavir, lamivudine and zidovudine in the primary analysis of efficacy. In a secondary analysis of patients with baseline plasma HIV-1 RNA levels above 100,000 copies per ml, patients receiving the combination containing indinavir had a superior response. Patients with baseline plasma HIV-1 RNA below 100,000 copies per ml had an equivalent response to both treatments.
A once daily regimen of abacavir and lamivudine was investigated in a multicentre, double-blind, controlled study (CNA30021) of 770 HIV-infected, therapy-naive adults. They were randomised to receive either ZIAGEN 600 mg once daily or 300 mg twice daily, both in combination with lamivudine 300 mg once daily and efavirenz 600 mg once daily. Patients were stratified at baseline based on plasma HIV-1 RNA less than or equal to100,000 copies/ml or greater than 100,000 copies/ml. The duration of double-blind treatment was at least 48 weeks. The results are summarised in the table as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe abacavir once daily group was demonstrated to be non-inferior when compared to the twice daily group in the overall and base-line viral load sub-groups. The incidence of adverse events reported was similar in the two treatment groups.
Genotypic analysis was attempted for all subjects with virologic failure (confirmed HIV RNA greater than 50 copies/ml). There was a low overall incidence of virologic failure in both the once and twice daily treatment groups (10% and 8%, respectively). Additionally genotyping was restricted to samples with plasma HIV-1 RNA greater than 500 copies/ml. These factors resulted in a small sample size. Therefore no firm conclusions could be drawn regarding differences in treatment emergent mutations between the two treatment groups. Reverse transcriptase amino acid residue 184 was consistently the most frequent position for NRTI resistance-associated mutations (M184V or M184I). The second most frequent mutation was L74V. Mutations Y115F and K65R were uncommon.
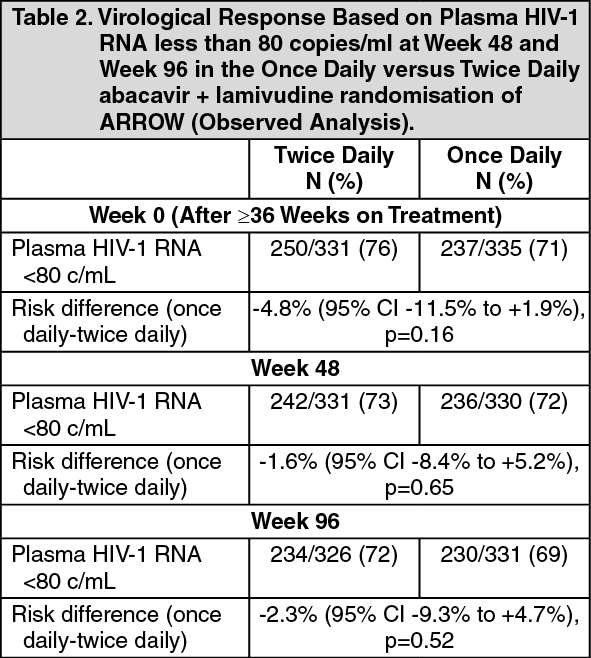
A randomised comparison of a regimen including once daily vs twice daily dosing of abacavir and lamivudine was undertaken within a randomised, multicentre, controlled study of HIV-infected, paediatric patients. 1206 paediatric patients aged 3 months to 17 years enrolled in the ARROW Trial (COL105677) and were dosed according to the weight - band dosing recommendations in the World Health Organisation treatment guidelines (Antiretroviral therapy of HIV infection in infants and children, 2006). After 36 weeks on a regimen including twice daily abacavir and lamivudine, 669 eligible subjects were randomised to either continue twice daily dosing or switch to once daily abacavir and lamivudine for at least 96 weeks. The results are summarised in the table as follows: (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe abacavir/lamivudine once daily dosing group was demonstrated to be non-inferior to the twice daily group according to the pre-specified non-inferiority margin of -12%, for the primary endpoint of <80 c/mL at Week 48 as well as at Week 96 (secondary endpoint) and all other thresholds tested (<200c/mL, <400c/mL, <1000c/mL), which all fell well within this non-inferiority margin. Subgroup analyses testing for heterogeneity of once vs twice daily demonstrated no significant effect of sex, age, or viral load at randomisation. Conclusions supported non-inferiority regardless of analysis method.
In a study comparing unblinded NRTI combinations (with or without blinded nelfinavir) in children, a significantly greater proportion treated with abacavir and lamivudine (73%) or abacavir and zidovudine (70%) had HIV-1 RNA less than or equal to 400 copies/ml at 24 weeks, compared with those treated with lamivudine and zidovudine (44%). In children with extensive antiretroviral exposure, a modest but sustained effect of the combination of abacavir, lamivudine and zidovudine was observed.
In therapy experienced patients, the degree of benefit from the addition of abacavir will depend on the nature and duration of prior therapy which may have selected for cross resistance to abacavir.
Antiretroviral Pregnancy Registry: The Antiretroviral Pregnancy Registry has received prospective reports of over 2,000 exposures to abacavir during pregnancy resulting in live birth. These consist of over 800 exposures during the first trimester, over 1,100 exposures during the second/third trimester and included 27 and 32 birth defects respectively. The prevalence (95% CI) of defects in the first trimester was 3.1% (2.0, 4.4%) and in the second/third trimester, 2.7% (1.9, 3.9%). Among pregnant women in the reference population, the background rate of birth defects is 2.7%. There was no association between abacavir and overall birth defects observed in the Antiretroviral Pregnancy Registry.
Pharmacokinetics: Absorption: Abacavir is rapidly and well absorbed following oral administration. The absolute bioavailability of oral abacavir in adults is about 83%. Following oral administration, the mean time (tmax) to maximal serum concentrations of abacavir is about 1.5 hours for the tablet formulation and about 1 hour for the solution formulation.
There are no differences observed between the AUC for the tablet or solution. At a dosage of 300 mg twice daily, the mean steady state Cmax of abacavir from tablet administration was 3.00 micrograms/ml, and the mean AUC over a dosing interval of 12 h was 6.02 micrograms.h/ml (daily AUC of approximately 12.0 micrograms.h/ml). The Cmax value for the oral solution is slightly higher than the tablet. After a 600 mg ZIAGEN tablet dose, the mean abacavir Cmax was approximately 4.26 micrograms/ml and the mean AUC∞ was 11.95 micrograms.h/ml.
Food delayed absorption and decreased Cmax but did not affect overall plasma concentrations (AUC). Therefore ZIAGEN can be taken with or without food.
Administration of crushed tablets with a small amount of semi-solid food or liquid would not be expected to have an impact on the pharmaceutical quality, and would therefore not be expected to alter the clinical effect. This conclusion is based on the physiochemical and pharmacokinetic characteristics of the active ingredient and the in vitro dissolution behaviour of abacavir tablets in water, assuming that the patient crushes and transfers 100% of the tablet and ingests immediately.
Distribution: Following i.v. administration, the apparent volume of distribution was about 0.8 l/kg, indicating that abacavir penetrates freely into body tissues.
Studies in HIV infected patients have shown good penetration of abacavir into the cerebrospinal fluid (CSF), with a CSF to plasma AUC ratio of between 30 to 44%. In a Phase I pharmacokinetic study, the penetration of abacavir into the CSF was investigated following administration of ZIAGEN 300 mg twice a day. The mean concentration of abacavir achieved in the CSF 1.5 hours post dose was 0.14 micrograms/ml. In a further pharmacokinetic study of 600 mg twice a day, the CSF concentration of abacavir increased over time, from approximately 0.13 micrograms/ml at 0.5 to 1 hour after dosing, to approximately 0.74 micrograms/ml after 3 to 4 hours. While peak concentrations may not have been attained by 4 hours, the observed values are 9-fold greater than the IC50 of abacavir of 0.08 micrograms/ml or 0.26 micromoles.
Plasma protein binding studies in vitro indicate that abacavir binds only low to moderately (circa 49%) to human plasma proteins at therapeutic concentrations. This indicates a low likelihood for drug interactions through plasma protein binding displacement.
Metabolism: Abacavir is primarily metabolised by the liver with less than 2% of the administered dose being renally excreted, as unchanged compound. The primary pathways of metabolism in man are by alcohol dehydrogenase and by glucuronidation to produce the 5'-carboxylic acid and 5'-glucuronide which account for about 66% of the administered dose. These metabolites are excreted in the urine.
Elimination: The mean half-life of abacavir is about 1.5 hours. Following multiple oral doses of ZIAGEN 300 mg twice a day there is no significant drug accumulation. Elimination of abacavir is via hepatic metabolism with subsequent excretion of metabolites primarily in the urine. The metabolites and unchanged abacavir account for about 83% of the administered ZIAGEN dose in the urine the remainder is eliminated in the faeces.
Special Patient Populations: Children: Abacavir is rapidly and well absorbed from oral solution and tablet formulations administered to children. Plasma abacavir exposure has been shown to be the same for both formulations when administered at the same dose. Children receiving abacavir oral solution according to the recommended dosage regimen achieve plasma abacavir exposure similar to adults. Children receiving abacavir oral tablets according to the recommended dosage regimen achieve higher plasma abacavir exposure than children receiving oral solution because higher mg/kg doses are administered with the tablet formulation (see Dosage & Administration). Paediatric pharmacokinetic studies have demonstrated that once daily dosing provides equivalent AUC0-24 to twice daily dosing of the same total daily dose for both oral solution and tablet formulations.
There are insufficient safety data to recommend the use of ZIAGEN in infants less than 3 months old. The limited data available indicate that a dose of 2 mg/kg in neonates less than 30 days old provides similar or greater AUCs, compared to the 8 mg/kg dose administered to older children.
Elderly: The pharmacokinetics of abacavir have not been studied in patients over 65 years of age. When treating elderly patients consideration needs to be given to the greater frequency of decreased hepatic, renal and cardiac function, and concomitant disease or other drug therapy.
Renally impaired: Abacavir is primarily metabolised by the liver with approximately 2% of abacavir excreted unchanged in the urine. The pharmacokinetics of abacavir in patients with end-stage renal disease is similar to patients with normal renal function. Therefore no dosage reduction is required in patients with renal impairment.
Hepatically impaired: Abacavir is metabolised primarily by the liver. The pharmacokinetics of abacavir have been studied in patients with mild hepatic impairment (Child-Pugh score 5 to 6). The results showed that there was a mean increase of 1.89 fold in the abacavir AUC, and 1.58 fold in the half-life of abacavir. The AUCs of the metabolites were not modified by the liver disease. However, the rates of formation and elimination of these were decreased.
In order to achieve exposures that are within the therapeutic range of patients without liver disease, patients with mild hepatic impairment should receive 200 mg ZIAGEN twice daily. The pharmacokinetics have not been studied in patients with moderate or severe hepatic impairment, therefore ZIAGEN is not recommended in these patient groups.
Toxicology: Pre-clinical Safety Data: Carcinogenesis, mutagenesis: Abacavir was not mutagenic in bacterial tests but showed activity in vitro in the human lymphocyte chromosome aberration assay, the mouse lymphoma assay, and the in vivo micronucleus test. This is consistent with the known activity of other nucleoside analogues. These results indicate that abacavir is a weak clastogen both in vitro and in vivo at high test concentrations.
Carcinogenicity studies with orally administered abacavir in mice and rats showed an increase in the incidence of malignant and non-malignant tumours. Malignant tumours occurred in the preputial gland of males and the clitoral gland of females of both species, and in the liver, urinary bladder, lymph nodes and the subcutis of female rats.
The majority of these tumours occurred at the highest abacavir dose of 330 mg/kg/day in mice and 600 mg/kg/day in rats. These dose levels were equivalent to 24 to 32 times the expected systemic exposure in humans. The exception was the preputial gland tumour which occurred at a dose of 110 mg/kg. This is equivalent to six times the expected human systemic exposure. There is no structural counterpart for this gland in humans. While the carcinogenic potential in humans is unknown, these data suggest that a carcinogenic risk to humans is outweighed by the potential clinical benefit.
Reproductive toxicology: Placental transfer of abacavir and/or its related metabolites has been shown to occur in animals. Evidence of toxicity to the developing embryo and foetuses occurred only in rats at maternally toxic doses of 500 mg/kg/day and above. This dose is equivalent to 32 to 35 times human therapeutic exposure based on AUC. The findings included foetal oedema, variations and malformations, resorptions, decreased foetal body weight and an increase in still births. The dose at which there were no effects on pre or post natal development was 160 mg/kg/day. This dose is equivalent to an exposure of about 10 times that in humans. Similar findings were not observed in rabbits.
A fertility study in the rat has shown that doses up to 500 mg/kg of abacavir had no effect on male or female fertility.
Animal toxicology and/or pharmacology: Mild myocardial degeneration in the heart of mice and rats was observed following administration of abacavir for two years. The systemic exposures were equivalent to 7 to 24 times the expected systemic exposure in humans. The clinical relevance of this finding has not been determined.