


 Sign Out
Sign Out

Hypocalcaemia has very commonly been reported following XGEVA administration, mostly within the first 2 weeks. Hypocalcaemia can be severe and symptomatic (see Description of selected adverse reactions as follows). The decreases in serum calcium were generally appropriately managed by calcium and vitamin D supplementation. The most common adverse reactions with XGEVA are musculoskeletal pain. Cases of osteonecrosis of the jaw (see Precautions and Description of selected adverse reactions as follows) have been commonly observed in patients taking XGEVA.
Tabulated list of adverse reactions: The following convention has been used for the classification of the adverse reactions based on incidence rates in four phase III, two phase II clinical studies and post-marketing experience (see table 3): very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000) and not known (cannot be estimated from the available data). Within each frequency grouping and system organ class, adverse reactions are presented in order of decreasing seriousness. (See Table 3.)
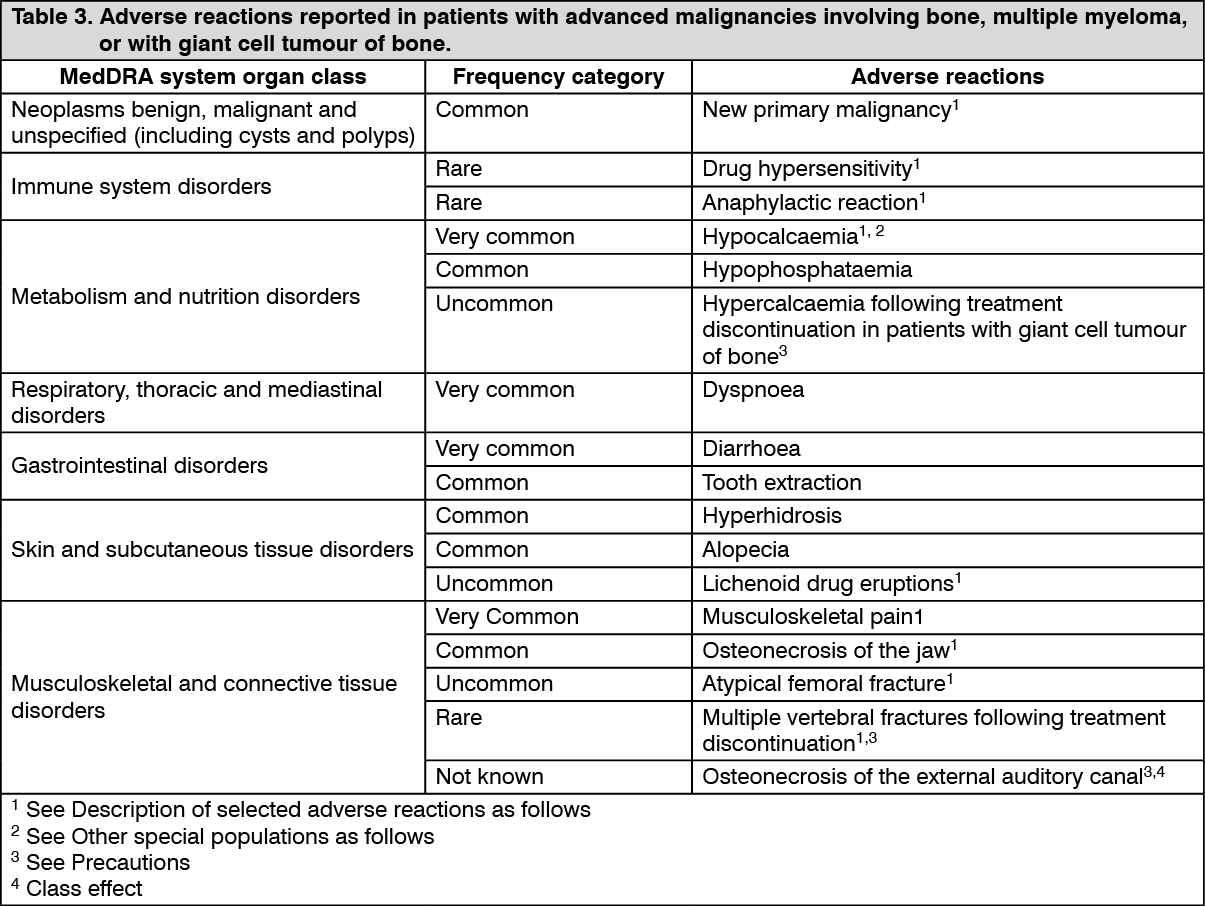 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Hypocalcaemia: A higher incidence of hypocalcaemia among subjects treated with denosumab compared to zoledronic acid has been observed in SRE prevention clinical trials.
The highest incidence of hypocalcaemia was observed in a phase III trial in patients with multiple myeloma. Hypocalcaemia was reported in 16.9% of patients treated with XGEVA and 12.4% of patients treated with zoledronic acid. A grade 3 decrease in serum calcium levels was experienced in 1.4% of patients treated with XGEVA and 0.6% of patients treated with zoledronic acid. A grade 4 decrease in serum calcium levels was experienced in 0.4% of patients treated with XGEVA and 0.1% of patients treated with zoledronic acid.
In three phase III active-controlled clinical trials in patients with advanced malignancies involving bone, hypocalcaemia was reported in 9.6% of patients treated with XGEVA and 5.0% of patients treated with zoledronic acid.
A grade 3 decrease in serum calcium levels was experienced in 2.5% of patients treated with XGEVA and 1.2% of patients treated with zoledronic acid. A grade 4 decrease in serum calcium levels was experienced in 0.6% of patients treated with XGEVA and 0.2% of patients treated with zoledronic acid (see Precautions).
In two phase II single-arm clinical trials in patients with giant cell tumour of bone, hypocalcaemia was reported in 5.7% of patients. None of the adverse events was considered serious.
In the post-marketing setting, severe symptomatic hypocalcaemia (including fatal cases) has been reported, with most cases occurring in the first weeks of initiating therapy. Examples of clinical manifestations of severe symptomatic hypocalcaemia have included QT interval prolongation, tetany, seizures and altered mental status (including coma) (see Precautions). Symptoms of hypocalcaemia in clinical studies included paraesthesias or muscle stiffness, twitching, spasms and muscle cramps.
Osteonecrosis of the Jaw (ONJ): In clinical trials, the incidence of ONJ was higher with longer duration of exposure; ONJ has also been diagnosed after stopping treatment with XGEVA with the majority of cases occurring within 5 months after the last dose. Patients with prior history of ONJ or osteomyelitis of the jaw, an active dental or jaw condition requiring oral surgery, non-healed dental/oral surgery, or any planned invasive dental procedure were excluded from the clinical trials.
A higher incidence of ONJ among subjects treated with denosumab compared to zoledronic acid has been observed in SRE prevention clinical trials. The highest incidence of ONJ was observed in a phase III trial in patients with multiple myeloma. In the double-blind treatment phase of this trial, ONJ was confirmed in 5.9% of patients treated with XGEVA (median exposure of 19.4 months; range 1 - 52) and in 3.2% of patients treated with zoledronic acid. At the completion of the double-blind treatment phase of this trial, the patient-year adjusted incidence of confirmed ONJ in the XGEVA group (median exposure of 19.4 months; range 1 - 52), was 2.0 per 100 patient-years during the first year of treatment, 5.0 in the second year, and 4.5 thereafter. The median time to ONJ was 18.7 months (range: 1 - 44).
In the primary treatment phases of three phase III active-controlled clinical trials in patients with advanced malignancies involving bone, ONJ was confirmed in 1.8% of patients treated with XGEVA (median exposure of 12.0 months; range 0.1 - 40.5) and 1.3% of patients in the zoledronic acid. Clinical characteristics of these cases were similar between treatment groups. Among subjects with confirmed ONJ, most (81% in both treatment groups) had a history of tooth extraction, poor oral hygiene, and/or use of a dental appliance. Most subjects were receiving or had received chemotherapy.
The trials in patients with breast or prostate cancer included an XGEVA extension treatment phase (median overall exposure of 14.9 months; range 0.1 - 67.2). ONJ was confirmed in 6.9% of patients with breast cancer and prostate cancer during the extension treatment phase.
The patient-year adjusted overall incidence of confirmed ONJ was 1.1 per 100 patient-years during the first year of treatment, 3.7 in the second year and 4.6 thereafter. The median time to ONJ was 20.6 months (range: 4 - 53).
In a phase III trial in patients with non-metastatic prostate cancer (a patient population for which XGEVA is not indicated), with longer treatment exposure of up to 7 years, the patient-year adjusted incidence of confirmed ONJ was 1.1 per 100 patient-years during the first year of treatment, 3.0 in the second year and 7.1 thereafter.
In a long-term phase II open-label clinical trial in patients with giant cell tumour of bone (Study 6, see Pharmacology: Pharmacodynamics under Actions), ONJ was confirmed in 6.8% of patients, including one adolescent (median number of 34 doses; range 4 - 116). At the completion of the trial, median time on trial including safety follow-up phase was 60.9 months (range: 0 - 112.6). The patient-year adjusted incidence of confirmed ONJ was 1.5 per 100 patient-years overall (0.2 per 100 patient-years during the first year of treatment, 1.5 in the second year, 1.8 in the third year, 2.1 in the fourth year, 1.4 in the fifth year, and 2.2 thereafter). The median time to ONJ was 41 months (range: 11 - 96).
Drug related hypersensitivity reactions: In the post-marketing setting, events of hypersensitivity, including rare events of anaphylactic reactions, have been reported in patients receiving XGEVA.
Atypical fractures of the femur: In the clinical trial programme, atypical femoral fractures have been reported uncommonly in patients treated with XGEVA and the risk increased with longer duration of treatment. Events have occurred during treatment and up to 9 months after the treatment was discontinued (see Precautions).
Multiple vertebral fractures: In the clinical trial program, multiple vertebral fractures, (not due to bone metastases), were reported rarely, following discontinuation of treatment with XGEVA, in patients with risk factors such as osteoporosis or prior (non-vertebral or vertebral) fractures (see Precautions).
Musculoskeletal Pain: In the post-marketing setting, musculoskeletal pain, including severe cases, has been reported in patients receiving XGEVA. In clinical trials, musculoskeletal pain was very common in both the denosumab and zoledronic acid treatment groups. Musculoskeletal pain leading to discontinuation of study treatment was uncommon.
New primary malignancy: In the primary double-blind treatment phases of four phase III active-controlled clinical trials in patients with advanced malignancies involving bone, new primary malignancy was reported in 54/3691 (1.5%) of patients treated with XGEVA (median exposure of 13.8 months; range: 1.0-51.7) and 33/3688 (0.9%) of patients treated with zoledronic acid (median exposure of 12.9 months; range: 1.0-50.8).
The cumulative incidence at one year was 1.1% for denosumab and 0.6% for zoledronic acid, respectively.
No treatment-related pattern in individual cancers or cancer groupings was apparent.
Lichenoid Drug Eruptions: In the post-marketing experience, lichenoid drug eruptions (e.g., lichen planus-like reactions) have been observed.
Paediatric population: XGEVA was studied in an open label trial that enrolled 28 skeletally mature adolescents with giant cell tumour of bone. Based on these limited data, the adverse event profile appeared to be similar to adults.
Clinically significant hypercalcaemia after treatment discontinuation has been reported in the post-marketing setting in paediatric patients (see Precautions).
Other special populations: Renal Impairment: In a clinical study of patients without advanced cancer with severe renal impairment (creatinine clearance < 30 mL/min) or receiving dialysis, there was a greater risk of developing hypocalcaemia in the absence of calcium supplementation. The risk of developing hypocalcaemia during XGEVA treatment is greater with increasing degree of renal impairment. In a clinical study in patients without advanced cancer, 19% of patients with severe renal impairment (creatinine clearance < 30 mL/min) and 63% of patients receiving dialysis developed hypocalcaemia despite calcium supplementation. The overall incidence of clinically significant hypocalcaemia was 9%.
Accompanying increases in parathyroid hormone have also been observed in patients receiving XGEVA with severe renal impairment or receiving dialysis. Monitoring of calcium levels and adequate intake of calcium and vitamin D is especially important in patients with renal impairment (see Precautions).
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions as per local regulations.
View ADR Monitoring Form