Pharmacology: Mechanism of Action: Tofacitinib is a Janus kinase (JAK) inhibitor. JAKs are intracellular enzymes which transmit signals arising from cytokine or growth factor-receptor interactions on the cellular membrane to influence cellular processes of hematopoiesis and immune cell function. Within the signaling pathway, JAKs phosphorylate and activate Signal Transducers and Activators of Transcription (STATs) which modulate intracellular activity including gene expression. Tofacitinib modulates the signaling pathway at the point of JAKs, preventing the phosphorylation and activation of STATs. JAK enzymes transmit cytokine signaling through pairing of JAKs (e.g., JAK1/JAK3, JAK1/JAK2, JAK1/TyK2, JAK2/JAK2). Tofacitinib inhibited the
in vitro activities of JAK1/JAK2, JAK1/JAK3, and JAK2/JAK2 combinations with IC
50 of 406, 56, and 1377 nM, respectively. However, the relevance of specific JAK combinations to therapeutic effectiveness is not known.
Pharmacodynamics: Treatment with tofacitinib was associated with dose-dependent reductions of circulating CD16/56+ natural killer cells, with estimated maximum reductions occurring at approximately 8-10 weeks after initiation of therapy. These changes generally resolved within 2-6 weeks after discontinuation of treatment. Treatment with tofacitinib was associated with dose-dependent increases in B cell counts. Changes in circulating T-lymphocyte counts and T-lymphocyte subsets (CD3+, CD4+ and CD8+) were small and inconsistent. The clinical significance of these changes is unknown.
Total serum IgG, IgM, and IgA levels after 6-month dosing in patients with rheumatoid arthritis were lower than placebo; however, changes were small and not dose-dependent.
After treatment with tofacitinib in patients with rheumatoid arthritis, rapid decreases in serum C-reactive protein (CRP) were observed and maintained throughout dosing. Changes in CRP observed with tofacitinib treatment do not reverse fully within 2 weeks after discontinuation, indicating a longer duration of pharmacodynamic activity compared to the pharmacokinetic half-life.
Similar changes in T cells, B cells, and serum CRP have been observed in patients with active psoriatic arthritis although reversibility was not assessed. Total serum immunoglobulins were not assessed in patients with active psoriatic arthritis.
Clinical Studies: The tofacitinib clinical development program included two dose-ranging trials and five confirmatory trials. Although other doses have been studied, the recommended dose of tofacitinib is 5 mg twice daily. Tofacitinib 10 mg twice daily is not recommended for the treatment of rheumatoid arthritis (see Dosage & Administration).
Dose-Ranging Trials: Dose selection for tofacitinib was based on two pivotal dose-ranging trials.
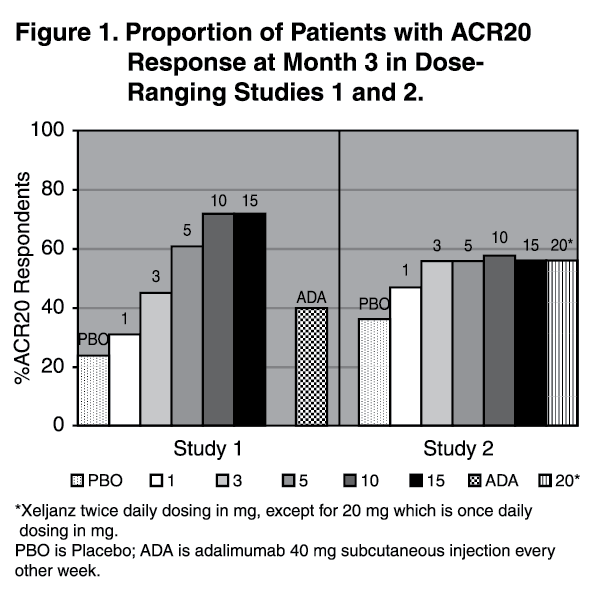
Dose-Ranging Study 1 was a 6-month monotherapy trial in 384 patients with active rheumatoid arthritis who had an inadequate response to a DMARD. Patients who previously received adalimumab therapy were excluded. Patients were randomized to 1 of 7 monotherapy treatments: tofacitinib 1, 3, 5, 10 or 15 mg twice daily, adalimumab 40 mg subcutaneously every other week for 10 weeks followed by tofacitinib 5 mg twice daily for 3 months, or placebo.
Dose-Ranging Study 2 was a 6-month trial in which 507 patients with active rheumatoid arthritis who had an inadequate response to MTX alone received one of 6 dose regimens of tofacitinib (20 mg once daily; 1, 3, 5, 10 or 15 mg twice daily), or placebo added to background MTX.
The results of tofacitinib-treated patients achieving ACR20 responses in Studies 1 and 2 are shown in Figure 1. Although a dose-response relationship was observed in Study 1, the proportion of patients with an ACR20 response did not clearly differ between the 10 mg and 15 mg doses. In Study 2, a smaller proportion of patients achieved an ACR20 response in the placebo and tofacitinib 1 mg groups compared to patients treated with the other tofacitinib doses. However, there was no difference in the proportion of responders among patients treated with tofacitinib 3, 5, 10, 15 mg twice daily or 20 mg once daily doses. (See Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Study 1 was a dose-ranging monotherapy trial not designed to provide comparative effectiveness data and should not be interpreted as evidence of superiority to adalimumab.
Confirmatory Trials: Study RA-I (NCT00814307) was a 6-month monotherapy trial in which 610 patients with moderate to severe active rheumatoid arthritis who had an inadequate response to a DMARD (nonbiologic or biologic) received tofacitinib 5 or 10 mg twice daily or placebo. At the Month 3 visit, all patients randomized to placebo treatment were advanced in a blinded fashion to a second predetermined treatment of tofacitinib 5 or 10 mg twice daily. The primary endpoints at Month 3 were the proportion of patients who achieved an ACR20 response, changes in Health Assessment Questionnaire - Disability Index (HAQ-DI), and rates of Disease Activity Score DAS28-4(ESR) less than 2.6.
Study RA-II (NCT00856544) was a 12-month trial in which 792 patients with moderate to severe active rheumatoid arthritis who had an inadequate response to a nonbiologic DMARD received tofacitinib 5 or 10 mg twice daily or placebo added to background DMARD treatment (excluding potent immunosuppressive treatments such as azathioprine or cyclosporine). At the Month 3 visit, nonresponding patients were advanced in a blinded fashion to a second predetermined treatment of tofacitinib 5 or 10 mg twice daily. At the end of Month 6, all placebo patients were advanced to their second predetermined treatment in a blinded fashion. The primary endpoints were the proportion of patients who achieved an ACR20 response at Month 6, changes in HAQ-DI at Month 3, and rates of DAS28-4(ESR) less than 2.6 at Month 6.
Study RA-III (NCT00853385) was a 12-month trial in 717 patients with moderate to severe active rheumatoid arthritis who had an inadequate response to MTX. Patients received tofacitinib 5 or 10 mg twice daily, adalimumab 40 mg subcutaneously every other week, or placebo added to background MTX. Placebo patients were advanced as in Study II. The primary endpoints were the proportion of patients who achieved an ACR20 response at Month 6, HAQ-DI at Month 3, and DAS28-4(ESR) less than 2.6 at Month 6.
Study RA-IV (NCT00847613) was a 2-year trial with a planned analysis at 1 year in which 797 patients with moderate to severe active rheumatoid arthritis who had an inadequate response to MTX received tofacitinib 5 or 10 mg twice daily or placebo added to background MTX. Placebo patients were advanced as in Study II. The primary endpoints were the proportion of patients who achieved an ACR20 response at Month 6, mean change from baseline in van der Heijde-modified total Sharp Score (mTSS) at Month 6, HAQ-DI at Month 3, and DAS28-4(ESR) less than 2.6 at Month 6.
Study RA-V (NCT00960440) was a 6-month trial in which 399 patients with moderate to severe active rheumatoid arthritis who had an inadequate response to at least one approved TNF-blocking biologic agent received tofacitinib 5 or 10 mg twice daily or placebo added to background MTX. At the Month 3 visit, all patients randomized to placebo treatment were advanced in a blinded fashion to a second predetermined treatment of tofacitinib 5 or 10 mg twice daily. The primary endpoints at Month 3 were the proportion of patients who achieved an ACR20 response, HAQ-DI, and DAS28-4(ESR) less than 2.6.
Clinical Response: The percentages of tofacitinib-treated patients achieving ACR20, ACR50, and ACR70 responses in Studies RA-I, IV, and V are shown in Table 1. Similar results were observed with Studies RA-II and III. In trials RA-I through V, patients treated with 5 mg twice daily tofacitinib had higher ACR20, ACR50, and ACR70 response rates versus placebo, with or without background DMARD treatment, at Month 3 and Month 6. Higher ACR20 response rates were observed within 2 weeks compared to placebo. In the 12-month trials, ACR response rates in tofacitinib-treated patients were consistent at 6 and 12 months. (See Table 1.)
Click on icon to see table/diagram/image
In Study RA-IV, a greater proportion of patients treated with tofacitinib 5 mg twice daily plus MTX achieved a low level of disease activity as measured by a DAS28-4(ESR) less than 2.6 at 6 months compared to those treated with MTX alone (Table 2). (See Table 2.)
Click on icon to see table/diagram/image
The results of the components of the ACR response criteria for Study RA-IV are shown in Table 3. Similar results were observed for tofacitinib in Studies RA-I, II, III and V. (See Table 3.)
Click on icon to see table/diagram/image
The percent of ACR20 responders by visit for Study RA-IV is shown in Figure 2. Similar responses were observed for tofacitinib in Studies RA-I, II, III and V. (See Figure 2.)
Click on icon to see table/diagram/image
Radiographic Response: One study was conducted to evaluate the effect of tofacitinib on structural joint damage. In Study RA-IV, progression of structural joint damage was assessed radiographically and expressed as change from baseline in mTSS and its components, the erosion score and joint space narrowing score, at Months 6 and 12. The proportion of patients with no radiographic progression (mTSS change less than or equal to 0) was also assessed.
In Study RA-IV, tofacitinib 5 mg twice daily reduced the mean progression of structural damage (not statistically significant) as shown in Table 4. Analyses of erosion and joint space narrowing scores were consistent with the overall results.
In the placebo plus MTX group, 74% of patients experienced no radiographic progression at Month 6 compared to 84% of patients treated with tofacitinib plus MTX 5 mg twice daily. (See Table 4.)
Click on icon to see table/diagram/image
Physical Function Response: Improvement in physical functioning was measured by the HAQ-DI. Patients receiving tofacitinib 5 mg twice daily demonstrated greater improvement from baseline in physical functioning compared to placebo at Month 3.
The mean (95% CI) difference from placebo in HAQ-DI improvement from baseline at Month 3 in Study RA-III was -0.22 (-0.35, -0.10) in patients receiving 5 mg tofacitinib twice daily. Similar results were obtained in Studies RA-I, II, IV and V. In the 12-month trials, HAQ-DI results in tofacitinib-treated patients were consistent at 6 and 12 months.
Other Health-Related Outcomes: General health status was assessed by the Short Form health survey (SF-36). In Studies RA-I, IV, and V, patients receiving tofacitinib 5 mg twice daily demonstrated greater improvement from baseline compared to placebo in physical component summary (PCS), mental component summary (MCS) scores and in all 8 domains of the SF-36 at Month 3.
Psoriatic Arthritis: The XELJANZ clinical development program to assess efficacy and safety included 2 multicenter, randomized, double-blind, placebo-controlled confirmatory trials in 816 patients 18 years of age and older (PsA-I and PsA-II). Although other doses have been studied, the recommended dose of XELJANZ is 5 mg twice daily. XELJANZ 10 mg twice daily is not recommended for the treatment of psoriatic arthritis [(see Dosage & Administration)]. All patients had active psoriatic arthritis for at least 6 months based upon the Classification Criteria for Psoriatic Arthritis (CASPAR), at least 3 tender/painful joints and at least 3 swollen joints, and active plaque psoriasis. Patients randomized and treated across the 2 clinical trials represented different psoriatic arthritis subtypes at screening, including <5 joints or asymmetric involvement (21%), ≥5 joints involved (90%), distal interphalangeal (DIP) joint involvement (61%), arthritis mutilans (8%), and spondylitis (19%). Patients in these clinical trials had a diagnosis of psoriatic arthritis for a mean (SD) of 7.7 (7.2) years. At baseline, 80% and 53% of patients had enthesitis and dactylitis, respectively. At baseline, all patients were required to receive treatment with a stable dose of a nonbiologic DMARD (79% received methotrexate, 13% received sulfasalazine, 7% received leflunomide, 1% received other nonbiologic DMARDs). In both clinical trials, the primary endpoints were the ACR20 response and the change from baseline in HAQ DI at Month 3.
Study PsA-I was a 12-month clinical trial in 422 patients who had an inadequate response to a nonbiologic DMARD (67% and 33% were inadequate responders to 1 nonbiologic DMARD and ≥2 nonbiologic DMARDs, respectively) and who were naïve to treatment with a TNF blocker. Patients were randomized in a 2:2:2:1:1 ratio to receive XELJANZ 5 mg twice daily, XELJANZ 10 mg twice daily, adalimumab 40 mg subcutaneously once every 2 weeks, placebo to XELJANZ 5 mg twice daily treatment sequence, or placebo to XELJANZ 10 mg twice daily treatment sequence, respectively; study drug was added to background nonbiologic DMARD treatment. At the Month 3 visit, all patients randomized to placebo treatment were advanced in a blinded fashion to a predetermined XELJANZ dose of 5 mg or 10 mg twice daily. Study PsA-I was not designed to demonstrate noninferiority or superiority to adalimumab.
Study PsA-II was a 6-month clinical trial in 394 patients who had an inadequate response to at least 1 approved TNF blocker (66%, 19%, and 15% were inadequate responders to 1 TNF blocker, 2 TNF blockers and ≥3 TNF blockers, respectively). Patients were randomized in a 2:2:1:1 ratio to receive XELJANZ 5 mg twice daily, XELJANZ 10 mg twice daily, placebo to XELJANZ 5 mg twice daily treatment sequence, or placebo to XELJANZ 10 mg twice daily treatment sequence, respectively; study drug was added to background nonbiologic DMARD treatment. At the Month 3 visit, placebo patients were advanced in a blinded fashion to a predetermined XELJANZ dose of 5 mg or 10 mg twice daily as in Study PsA-I.
Clinical Response: At Month 3, patients treated with XELJANZ 5 mg twice daily had higher (p≤0.05) response rates versus placebo for ACR20, ACR50, and ACR70 in Study PsA I and for ACR20 and ACR50 in Study PsA II; ACR70 response rates were also higher for XELJANZ 5 mg twice daily versus placebo in Study PsA II, although the differences versus placebo were not statistically significant (p>0.05). (See Tables 5 and 6.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Improvements from baseline in the ACR response criteria components for both studies are shown in Table 7. (See Table 7.)
Click on icon to see table/diagram/image
The percentage of ACR20 responders by visit for Study PsA-I is shown in Figure 3. Similar responses were observed in Study PsA-II. In both studies, improvement in ACR20 response on XELJANZ was observed at the first visit after baseline (Week 2). (See Figure 3.)
Click on icon to see table/diagram/image
In patients with active psoriatic arthritis evidence of benefit in enthesitis and dactylitis was observed with XELJANZ treatment.
Physical Function: Improvement in physical functioning was measured by the HAQ-DI. Patients receiving XELJANZ 5 mg twice daily demonstrated significantly greater improvement (p≤0.05) from baseline in physical functioning compared to placebo at Month 3 (Table 8). (See Table 8.)
Click on icon to see table/diagram/image
In Study PsA-I, the HAQ-DI responder rate (response defined as having improvement from baseline of ≥0.35) at Month 3 was 53% in patients receiving XELJANZ 5 mg twice daily and 31% in patients receiving placebo. Similar responses were observed in Study PsA-II.
Other Health-Related Outcomes: General health status was assessed by the Short Form health survey (SF-36). In Studies PsA-I and PsAII, patients receiving XELJANZ 5 mg twice daily had greater improvement from baseline compared to placebo in Physical Component Summary (PCS) score, but not in Mental Component Summary (MCS) score at Month 3. Patients receiving XELJANZ 5 mg twice daily reported consistently greater improvement relative to placebo in the domains of Physical Functioning, Bodily Pain, Vitality, and Social Functioning, but not in Role Physical, General Health, Role Emotional, or Mental Health.
Radiographic Response: Treatment effect on inhibition of radiographic progression in psoriatic arthritis could not be established from the results of Study PsA-I.
Ulcerative Colitis: Induction Trials (Study UC-I [NCT01465763] and Study UC-II [NCT01458951]): In two identical induction trials (UC-I and UC-II), 1139 patients were randomized (598 and 541 patients, respectively) to XELJANZ 10 mg twice daily or placebo with a 4:1 treatment allocation ratio. These trials included adult patients with moderately to severely active UC (total Mayo score of 6 to 12, with an endoscopy subscore of at least 2, and rectal bleeding subscore of at least 1) and who had failed or were intolerant to at least 1 of the following treatments: oral or intravenous corticosteroids, azathioprine, 6-MP or TNF blocker. XELJANZ is indicated for patients who have an inadequate response or intolerance to one or more TNF blockers (see Indications/Uses).
The disease activity was assessed by Mayo scoring index (0 to 12) which consists of four subscores (0 to 3 for each subscore): stool frequency, rectal bleeding, findings on endoscopy, and physician global assessment. An endoscopy subscore of 2 was defined by marked erythema, absent vascular pattern, any friability, and erosions; an endoscopy subscore of 3 was defined by spontaneous bleeding and ulceration.
Patients were permitted to use stable doses of oral aminosalicylates and corticosteroids (prednisone daily dose up to 25 mg equivalent). Concomitant immunosuppressants (oral immunomodulators or biologic therapies) were not permitted for UC patients during these studies.
A total of 52%, 73% and 72% of patients had previously failed or were intolerant to TNF blockers (51% in Study UC-1 and 52% in Study UC-II), corticosteroids (75% in Study UC-I and 71% in Study UC-II), and/or immunosuppressants (74% in Study UC-I and 70% in Study UC-II), respectively.
Oral corticosteroids were received as concomitant treatment for UC by 47% of patients (45% in Study UC-I and 48% in Study UC-II) and 71% were receiving concomitant aminosalicylates as treatment for UC (71% in Study UC-I, and 72% in Study UC-II). The baseline clinical characteristics were generally similar between the XELJANZ treated patients and patients receiving placebo.
The primary endpoint of Study UC-I and Study UC-II was the proportion of patients in remission at Week 8, and the key secondary endpoint was the proportion of patients with improvement of endoscopic appearance of the mucosa at Week 8.
The efficacy results of Study UC-I and Study UC-II based on the centrally read endoscopy results are shown in Table 9. (See Table 9.)
Click on icon to see table/diagram/image
Clinical Response at Week 8: Clinical response was defined as a decrease from baseline in Mayo score of ≥3 points and ≥30%, with an accompanying decrease in the subscore for rectal bleeding of ≥1 point or absolute subscore for rectal bleeding of 0 or 1.
Clinical response was observed in 60% of patients treated with XELJANZ 10 mg twice daily compared to 33% of placebo patients in Study UC-I and 55% compared to 29% in Study UC-II.
Normalization of the Endoscopic Appearance of the Mucosa at Week 8: Normalization of endoscopic appearance of the mucosa was defined as a Mayo endoscopic subscore of 0 and was observed in 7% of patients treated with XELJANZ 10 mg twice daily compared to 2% of placebo patients in both Studies UC-I and UC-II.
Rectal Bleeding and Stool Frequency: Decreases in rectal bleeding and stool frequency subscores were observed as early as Week 2 in patients treated with XELJANZ.
Maintenance Trial (Study UC-III [NCT01458574]): A total of 593 patients who completed the induction trials (UC-I or UC-II) and achieved clinical response were re-randomized with 1:1:1 treatment allocation ratio to XELJANZ 5 mg twice daily, XELJANZ 10 mg twice daily, or placebo for 52 weeks in Study UC-III. XELJANZ 5 mg twice daily is the recommended dosage for maintenance therapy; limit use of XELJANZ 10 mg twice daily beyond induction to those with loss of response and should be used for the shortest duration [see Dosage & Administration]. As in the induction trials, patients were permitted to use stable doses of oral aminosalicylates; however, corticosteroid tapering was required upon entrance into this study for patients who were receiving corticosteroids at baseline. Concomitant immunosuppressants (oral immunomodulators or biologic therapies) were not permitted.
At baseline of Study UC-III: 179 (30%) patients were in remission; 289 (49%) patients were receiving oral corticosteroids; 265 (45%), 445 (75%), and 413 (70%) patients had previously failed or were intolerant to TNF blocker therapy, corticosteroids, and immunosuppressants, respectively.
The primary endpoint was the proportion of patients in remission at Week 52. There were 2 key secondary endpoints: the proportion of patients with improvement of endoscopic appearance at Week 52, and the proportion of patients with sustained corticosteroid-free remission at both Week 24 and Week 52 among patients in remission at baseline of Study UC-III.
The efficacy results of Study UC-III based on the centrally read endoscopy results are summarized in Table 10. (See Table 10.)
Click on icon to see table/diagram/image
Maintenance of Clinical Response: Maintenance of clinical response was defined as the proportion of patients who met the definition of clinical response (defined as a decrease from the induction study (UC-I, UC-II) baseline Mayo score of ≥3 points and ≥30%, with an accompanying decrease in the rectal bleeding subscore of ≥1 point or rectal bleeding subscore of 0 or 1) at both Baseline and Week 52 of Study UC-III.
Maintenance of clinical response was observed in 52% in the XELJANZ 5 mg twice daily group and 62% in the XELJANZ 10 mg twice daily group compared to 20% of placebo patients.
Maintenance of Remission (Among Patients in Remission at Baseline): In the 179 patients who were in remission at baseline of Study UC-III (N = 59 for placebo, N = 65 for XELJANZ 5 mg twice daily, N = 55 for XELJANZ 10 mg twice daily), 46% in the XELJANZ 5 mg twice daily group and 56% in the XELJANZ 10 mg twice daily group maintained remission at Week 52 compared to 10% of placebo patients.
Normalization of the Endoscopic Appearance of the Mucosa: Normalization of endoscopic appearance of the mucosa was defined as a Mayo endoscopic subscore of
0 and was observed at Week 52 in 15% of patients in the XELJANZ 5 mg twice daily group and 17% of patients in the XELJANZ 10 mg twice daily group compared to 4% of placebo patients.
Open-label Extension Study (Study UC-IV [NCT01470612]): In Study UC-IV, 914 patients were treated of which 156 received 5 mg twice daily and 758 received 10 mg twice daily.
Of the 905 patients who were assigned to XELJANZ 10 mg twice daily in the 8-week induction studies (Study UC-I or Study UC-II), 322 patients completed the induction studies but did not achieve clinical response. Of these 322 patients, 291 continued to receive XELJANZ 10 mg twice daily (unblinded) and had available data after an additional 8 weeks in Study UC-IV. After 8 additional weeks (a total of 16 weeks treatment), 148 patients achieved clinical response, and 25 patients achieved remission (based on central endoscopy read). Among those 143 patients who achieved clinical response by 16 weeks and had available data at Week 52, 66 patients achieved remission (based on local endoscopy read) after continued treatment with XELJANZ 10 mg twice daily for 52 weeks.
Pharmacokinetics: XELJANZ: Following oral administration of tofacitinib, peak plasma concentrations are reached within 0.5-1 hour, elimination half-life is about 3 hours and a dose-proportional increase in systemic exposure was observed in the therapeutic dose range. Steady state concentrations are achieved in 24-48 hours with negligible accumulation after twice daily administration. (See Table 11.)
Click on icon to see table/diagram/image
Absorption: The absolute oral bioavailability of tofacitinib is 74%. Co-administration of tofacitinib with a high-fat meal resulted in no changes in AUC while C
max was reduced by 32%. In clinical trials, tofacitinib was administered without regard to meals (see Dosage & Administration).
Distribution: After intravenous administration, the volume of distribution is 87 L. The protein binding of tofacitinib is approximately 40%. Tofacitinib binds predominantly to albumin and does not appear to bind to α1-acid glycoprotein. Tofacitinib distributes equally between red blood cells and plasma.
Metabolism and Excretion: Clearance mechanisms for tofacitinib are approximately 70% hepatic metabolism and 30% renal excretion of the parent drug. The metabolism of tofacitinib is primarily mediated by CYP3A4 with minor contribution from CYP2C19. In a human radiolabeled study, more than 65% of the total circulating radioactivity was accounted for by unchanged tofacitinib, with the remaining 35% attributed to 8 metabolites, each accounting for less than 8% of total radioactivity. The pharmacologic activity of tofacitinib is attributed to the parent molecule.
Population Pharmacokinetics in Rheumatoid Arthritis Patients: Population pharmacokinetic analyses indicated that the coefficient of variation (%) in AUC of tofacitinib for patients with rheumatoid arthritis was 22.0% and psoriatic arthritis was 34% (Table 12). (See Table 12.)
Click on icon to see table/diagram/image
Specific Populations: Covariate evaluation as part of population PK analyses in patient populations indicated no clinically relevant change in tofacitinib exposure, after accounting for differences in renal function (i.e., creatinine clearance) between patients, based on age, weight, gender and race (Figure 4). An approximately linear relationship between body weight and volume of distribution was observed, resulting in higher peak (C
max) and lower trough (C
min) concentrations in lighter patients. However, this difference is not considered to be clinically relevant.
The effect of renal and hepatic impairment and other intrinsic factors on the pharmacokinetics of tofacitinib is shown in Figure 4. (See Figure 4.)
Click on icon to see table/diagram/image
In subjects with ESRD maintained on hemodialysis, mean AUC was approximately 40% higher compared with historical healthy subject data, consistent with approximately 30% contribution of renal clearance to the total clearance of tofacitinib. Dose adjustment is recommended in RA, PsA patients with ESRD maintained on hemodialysis (see Dosage & Administration, Contraindications and Precautions).
Pharmacokinetics in Patients with Active Ulcerative Colitis: Population PK analysis in ulcerative colitis patients indicated that there were no clinically relevant differences in tofacitinib exposure (AUC), based on age, weight, gender, and race. Exposure in women was 15% higher than in men, and Asian patients had 7.3% higher exposure than non Asian. Volume of distribution increased with body weight resulting in higher peak (Cmax) and lower trough (Cmin) concentrations in lighter patients. However, this difference is not considered to be clinically relevant. The between-subject variability (% coefficient of variation) in AUC of tofacitinib is estimated to be approximately 23% and 25% at the 5 mg twice daily dose and 10 mg twice daily dose, respectively, in ulcerative colitis patients.
Drug Interaction Studies: Potential for Tofacitinib to Influence the Pharmacokinetics of Other Drugs:
In vitro studies indicate that tofacitinib does not significantly inhibit or induce the activity of the major human drug-metabolizing CYPs (CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, and CYP3A4) at concentrations exceeding 160 times the steady state C
max of a 5 mg twice daily dose. These
in vitro results were confirmed by a human drug interaction study showing no changes in the pharmacokinetics of midazolam, a highly sensitive CYP3A4 substrate, when co-administered with tofacitinib.
In rheumatoid arthritis patients, the oral clearance of tofacitinib does not vary with time, indicating that tofacitinib does not normalize CYP enzyme activity in rheumatoid arthritis patients. Therefore, co-administration with tofacitinib is not expected to result in clinically relevant increases in the metabolism of CYP substrates in rheumatoid arthritis patients.
In vitro data indicate that the potential for tofacitinib to inhibit transporters such as P-glycoprotein, organic anionic or cationic transporters at therapeutic concentrations is low.
Dosing recommendations for co-administered drugs following administration with tofacitinib are shown in Figure 5. (See Figure 5.)
Click on icon to see table/diagram/image
Potential for Other Drugs to Influence the Pharmacokinetics of Tofacitinib: Since tofacitinib is metabolized by CYP3A4, interaction with drugs that inhibit or induce CYP3A4 is likely. Inhibitors of CYP2C19 alone or P-glycoprotein are unlikely to substantially alter the pharmacokinetics of tofacitinib (see Figure 6).
Click on icon to see table/diagram/image
Non-Clinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: In a 39-week toxicology study in monkeys, tofacitinib at exposure levels approximately 6 times the recommended dose of 5 mg twice daily (on an AUC basis at oral doses of 5 mg/kg twice daily) produced lymphomas. No lymphomas were observed in this study at exposure levels 1 times the recommended dose of 5 mg twice daily (on an AUC basis at oral doses of 1 mg/kg twice daily).
The carcinogenic potential of tofacitinib was assessed in 6-month rasH2 transgenic mouse carcinogenicity and 2-year rat carcinogenicity studies. Tofacitinib, at exposure levels approximately 34 times the recommended dose of 5 mg twice daily (on an AUC basis at oral doses of 200 mg/kg/day) was not carcinogenic in mice.
In the 24-month oral carcinogenicity study in Sprague-Dawley rats, tofacitinib caused benign Leydig cell tumors, hibernomas (malignancy of brown adipose tissue), and benign thymomas at doses greater than or equal to 30 mg/kg/day (approximately 42 times the exposure levels at the recommended dose of 5 mg twice daily on an AUC basis). The relevance of benign Leydig cell tumors to human risk is not known.
Tofacitinib was not mutagenic in the bacterial reverse mutation assay. It was positive for clastogenicity in the
in vitro chromosome aberration assay with human lymphocytes in the presence of metabolic enzymes, but negative in the absence of metabolic enzymes. Tofacitinib was negative in the
in vivo rat micronucleus assay and in the
in vitro CHO-HGPRT assay and the
in vivo rat hepatocyte unscheduled DNA synthesis assay.
In rats, tofacitinib at exposure levels approximately 17 times the recommended dose of 5 mg twice daily (on an AUC basis at oral doses of 10 mg/kg/day) reduced female fertility due to increased post-implantation loss. There was no impairment of female rat fertility at exposure levels of tofacitinib equal to the recommended dose of 5 mg twice daily (on an AUC basis at oral doses of 1 mg/kg/day). Tofacitinib exposure levels at approximately 133 times the recommended dose of 5 mg twice daily (on an AUC basis at oral doses of 100 mg/kg/day) had no effect on male fertility, sperm motility, or sperm concentration.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image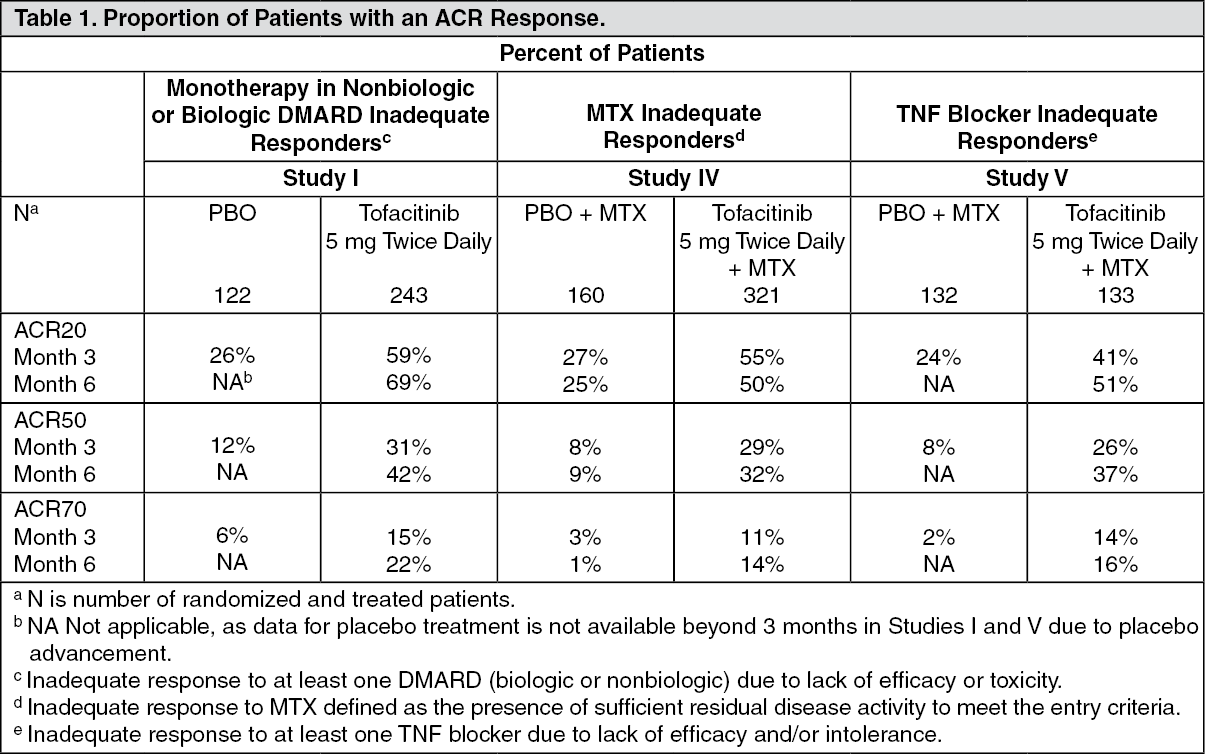 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image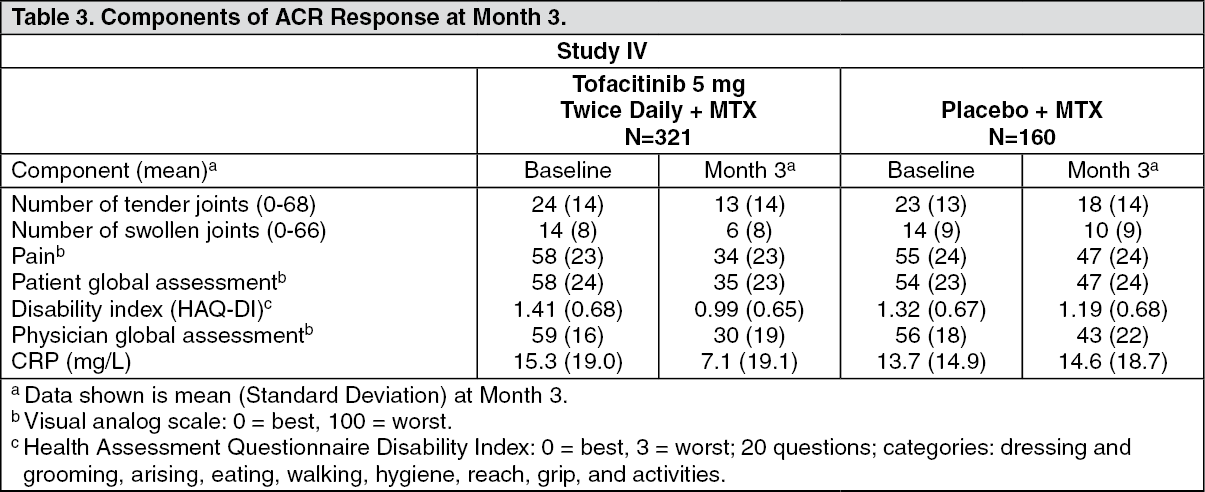 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image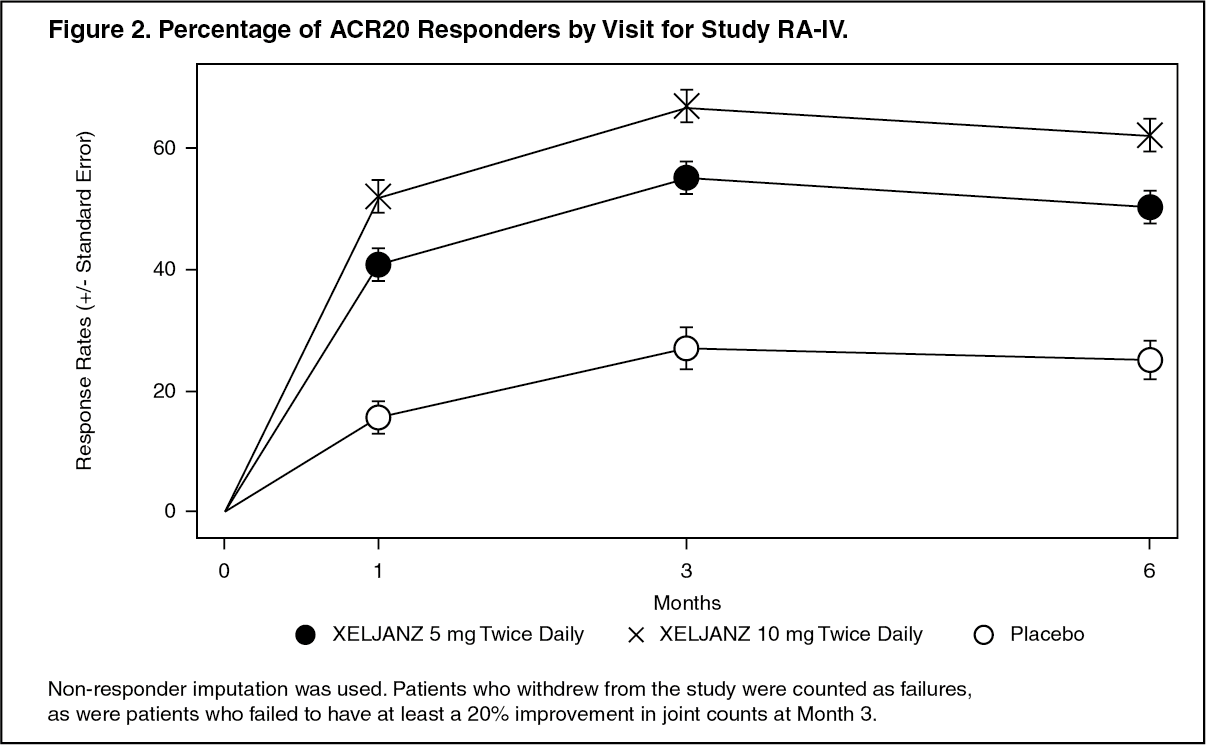 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image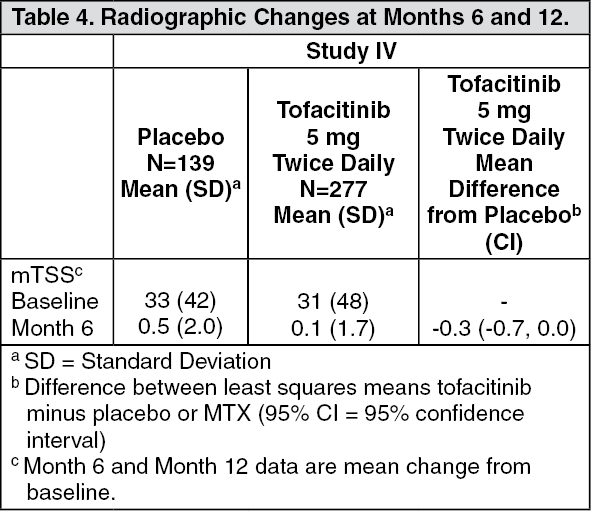 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image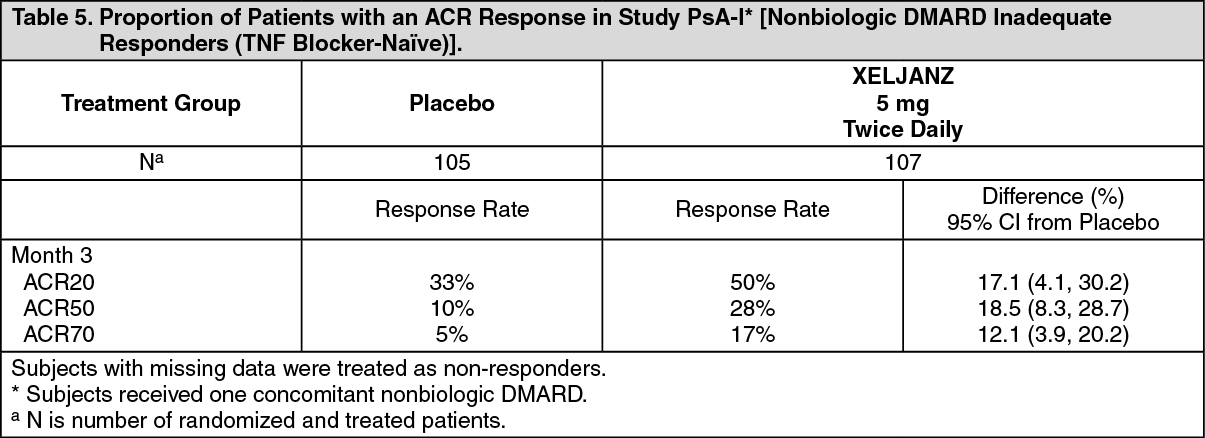 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image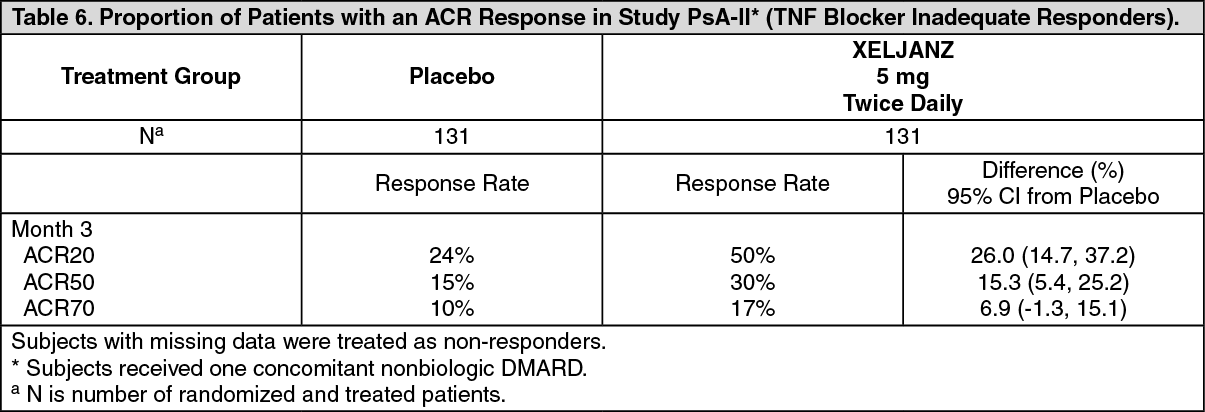 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image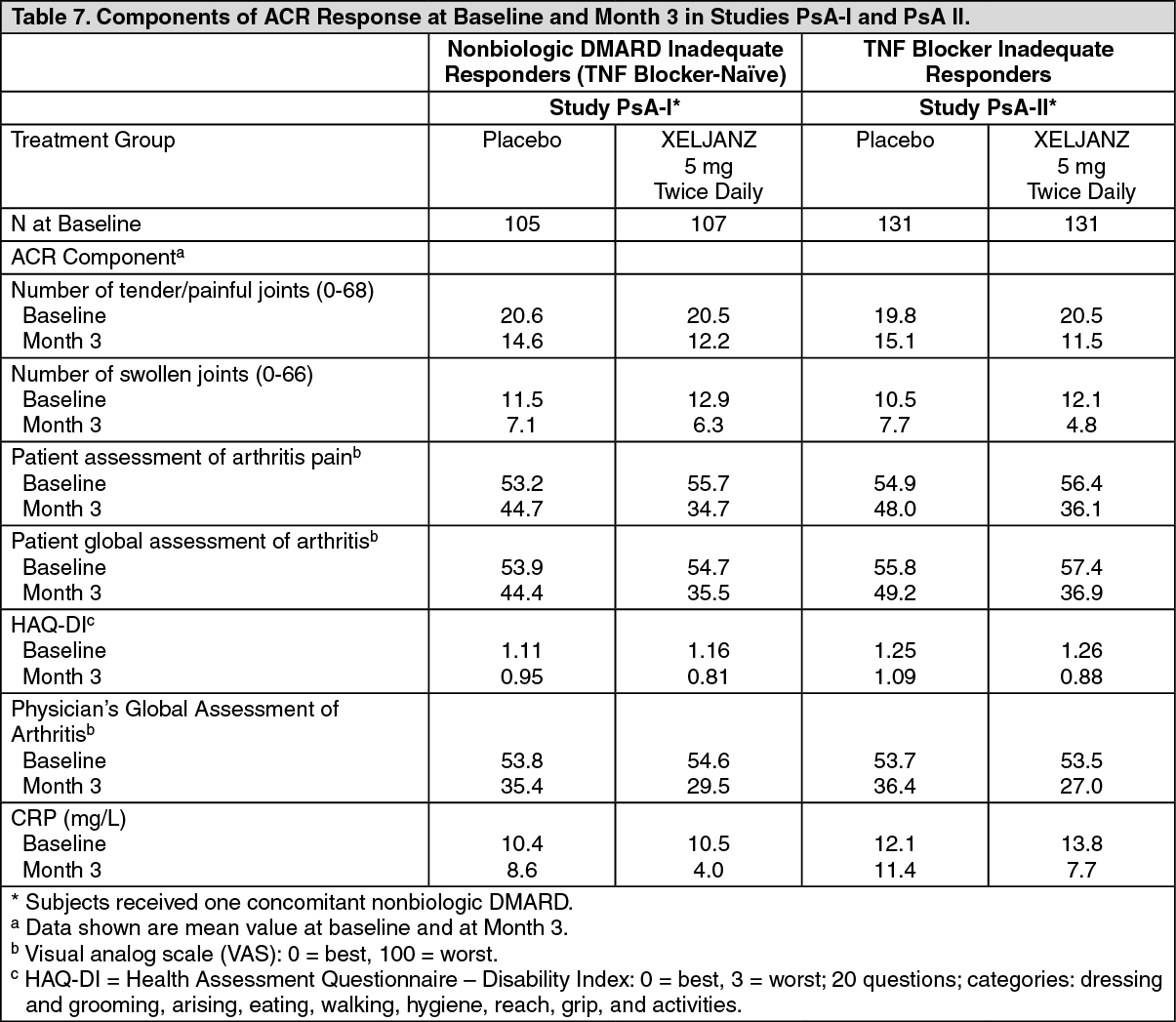 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image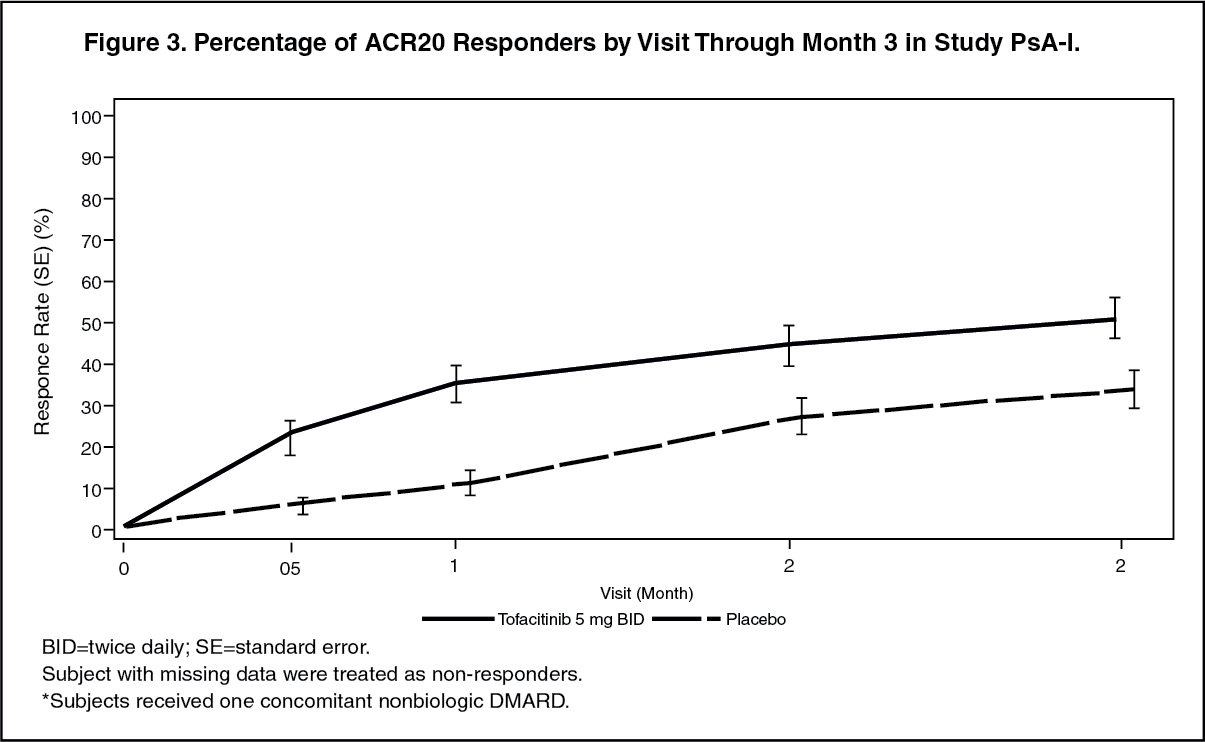 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image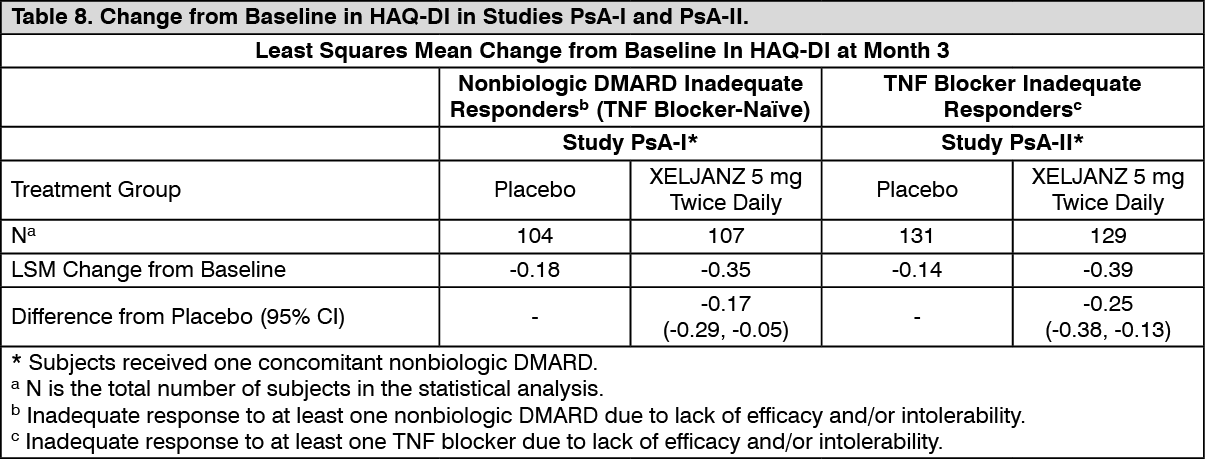 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image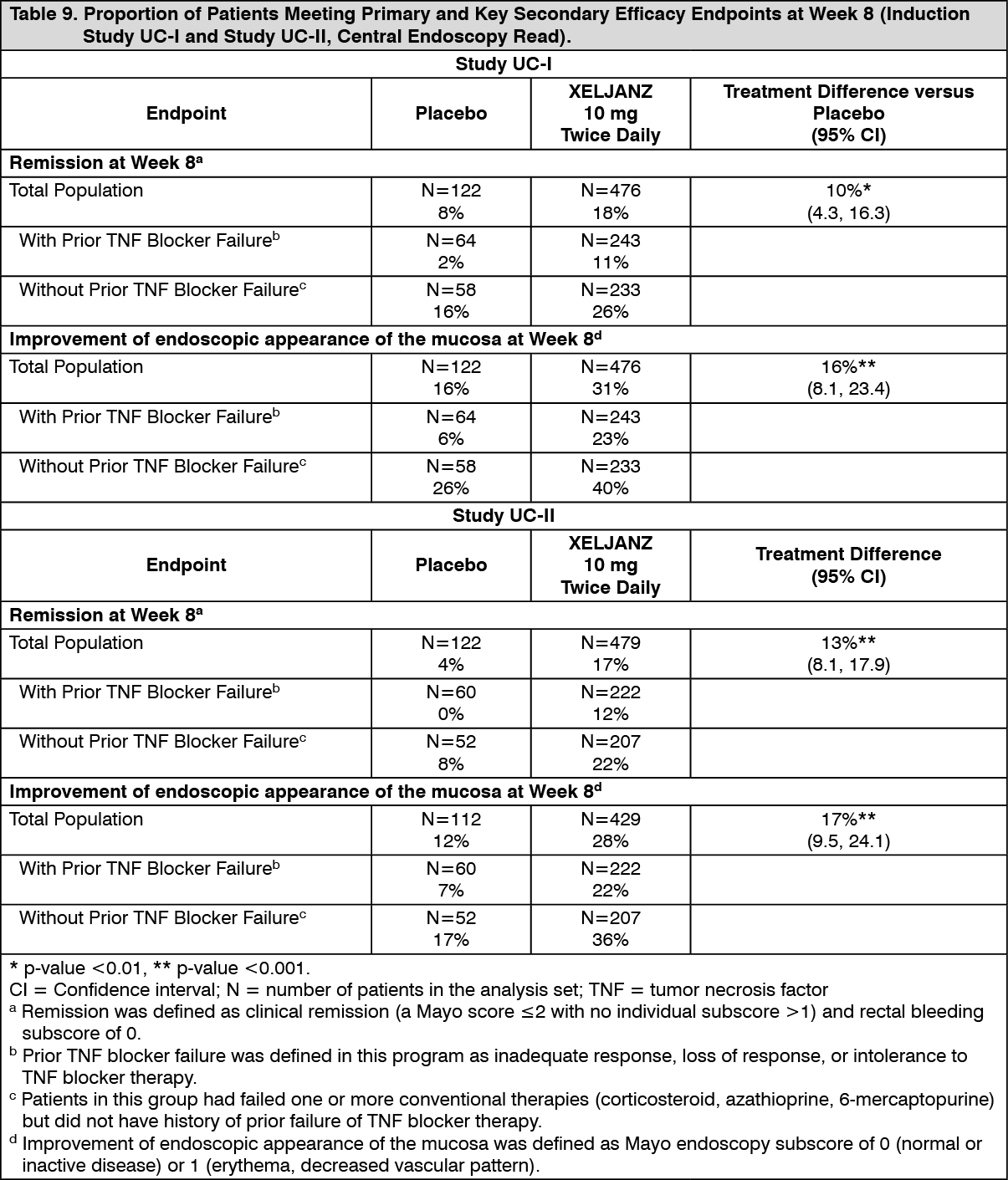 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image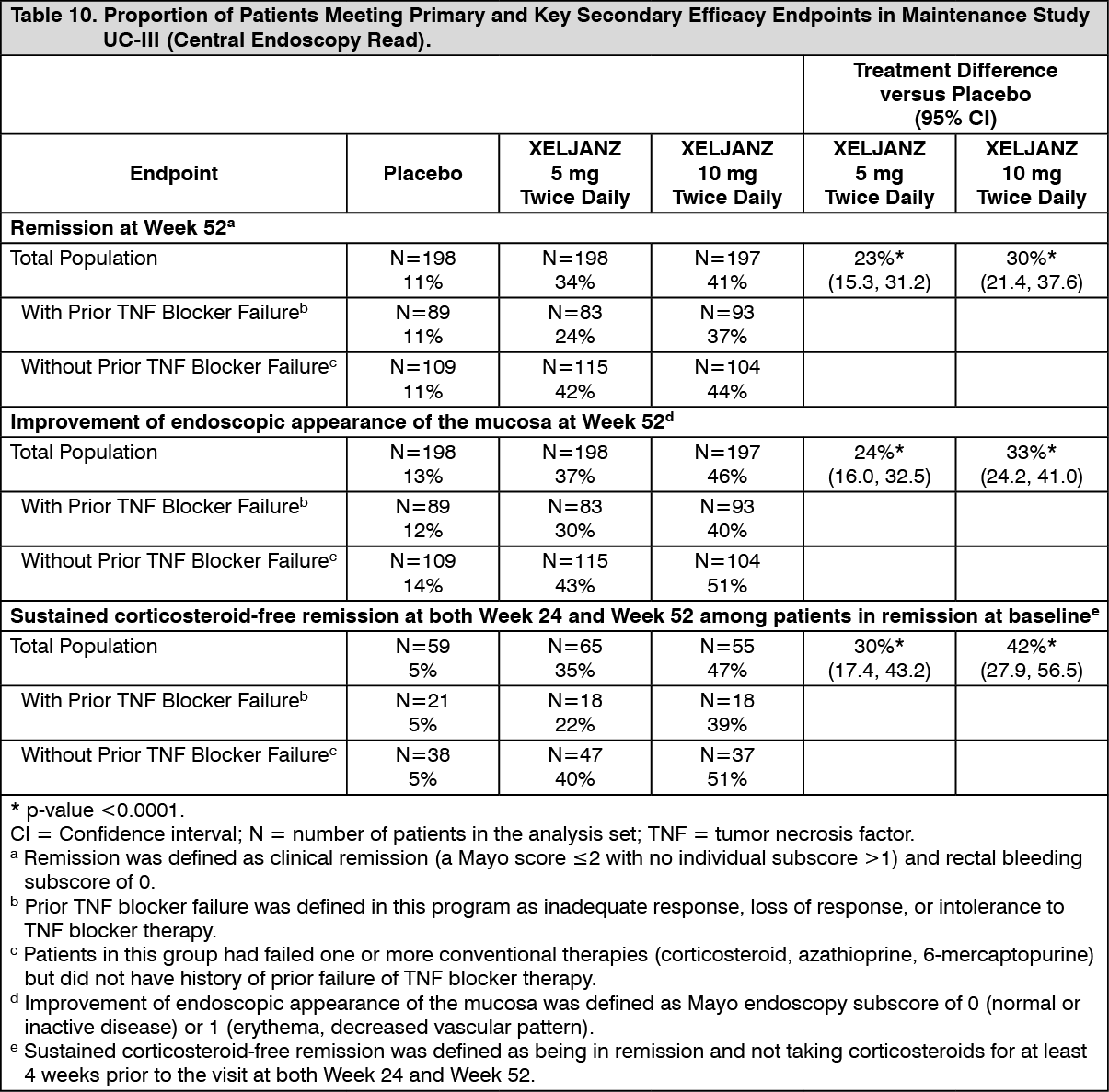 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image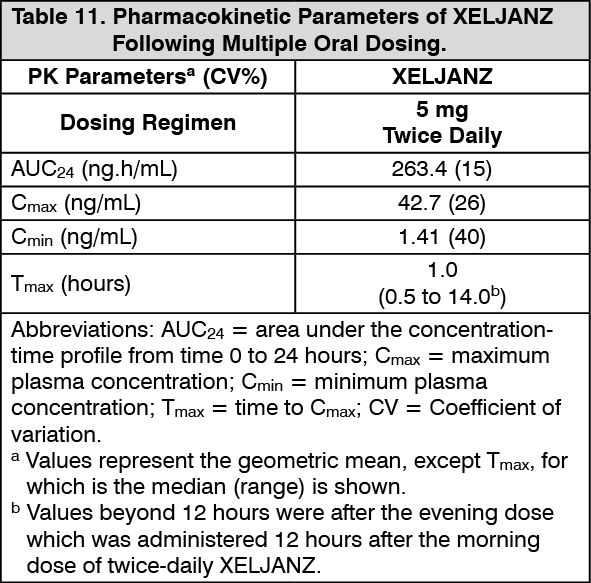 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image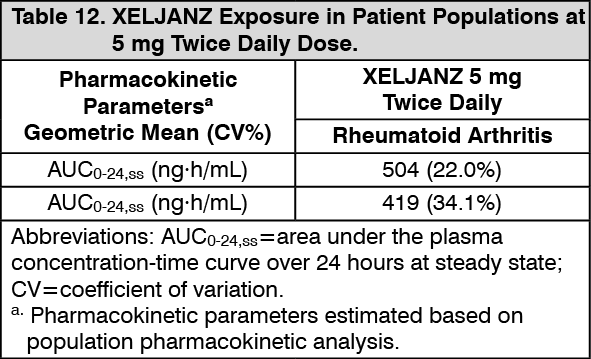 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image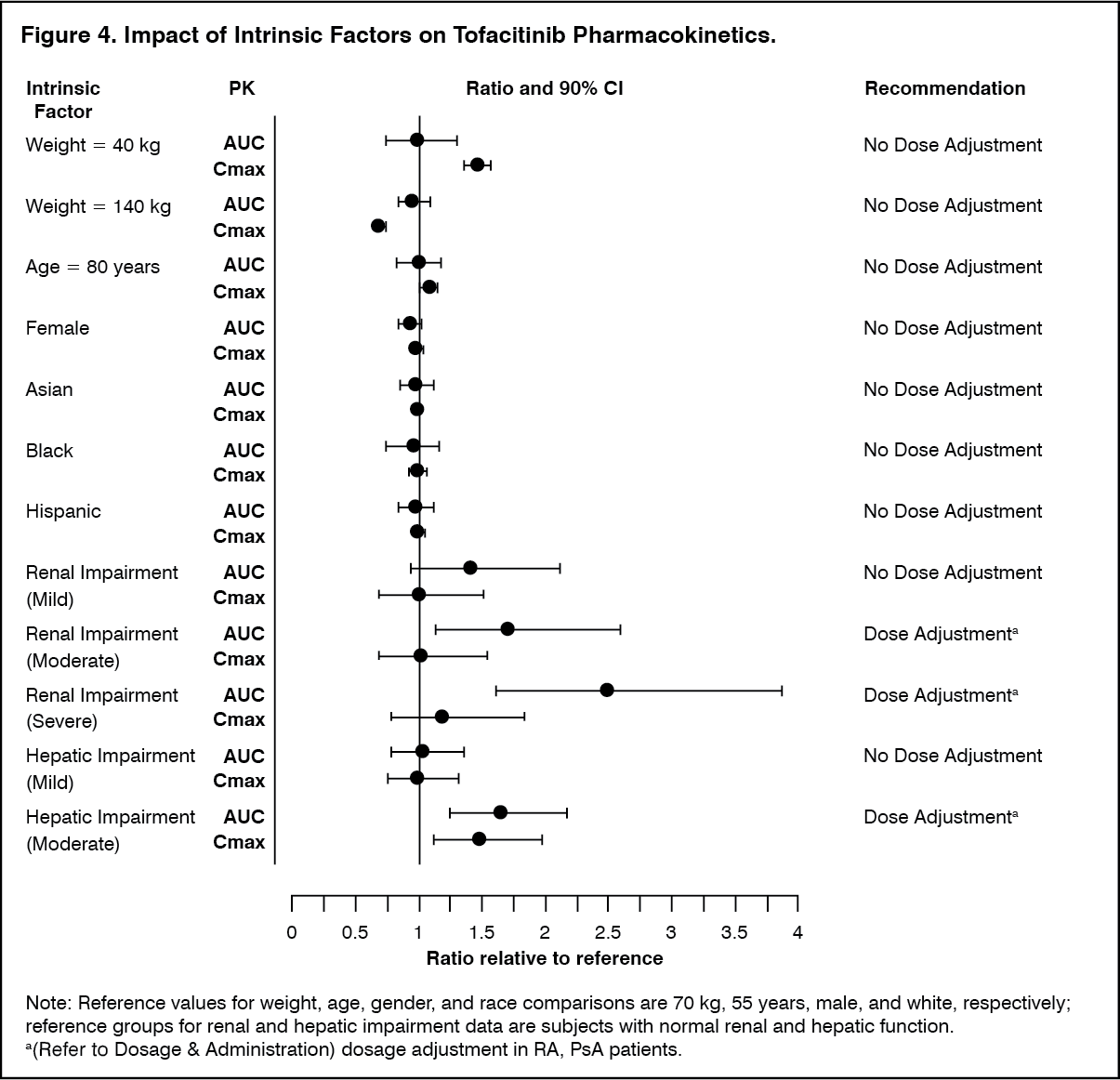 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image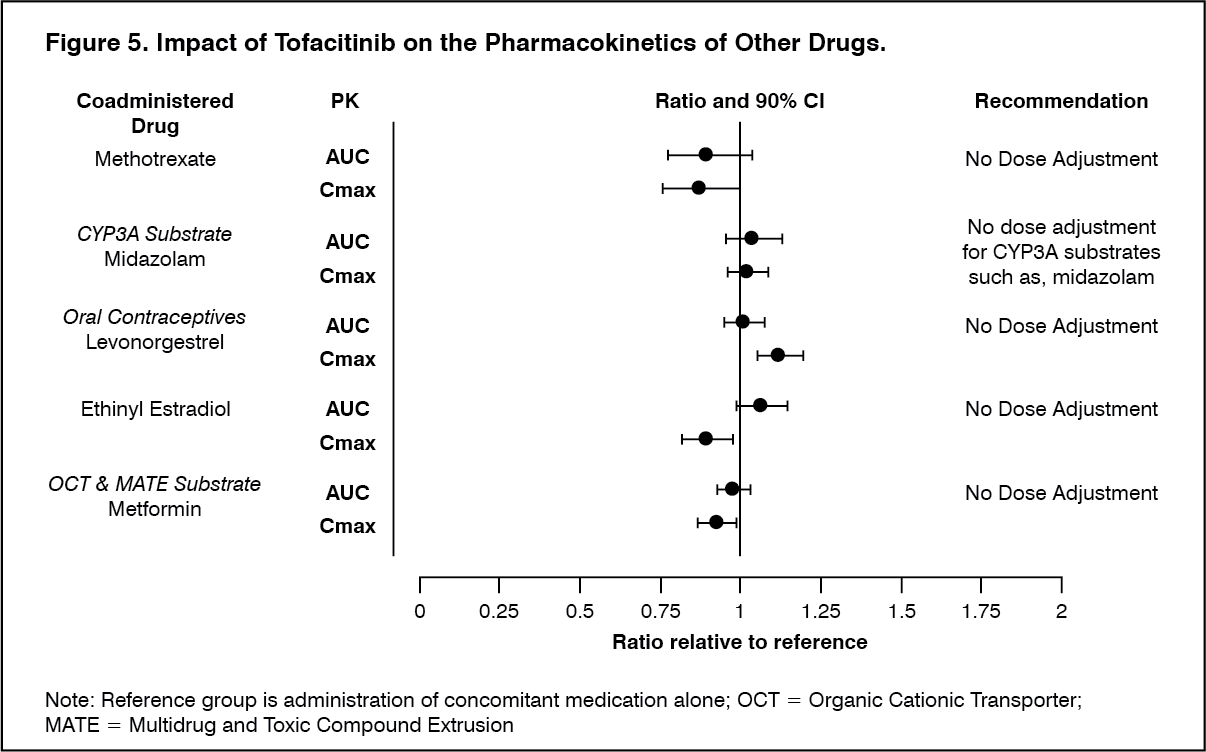 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image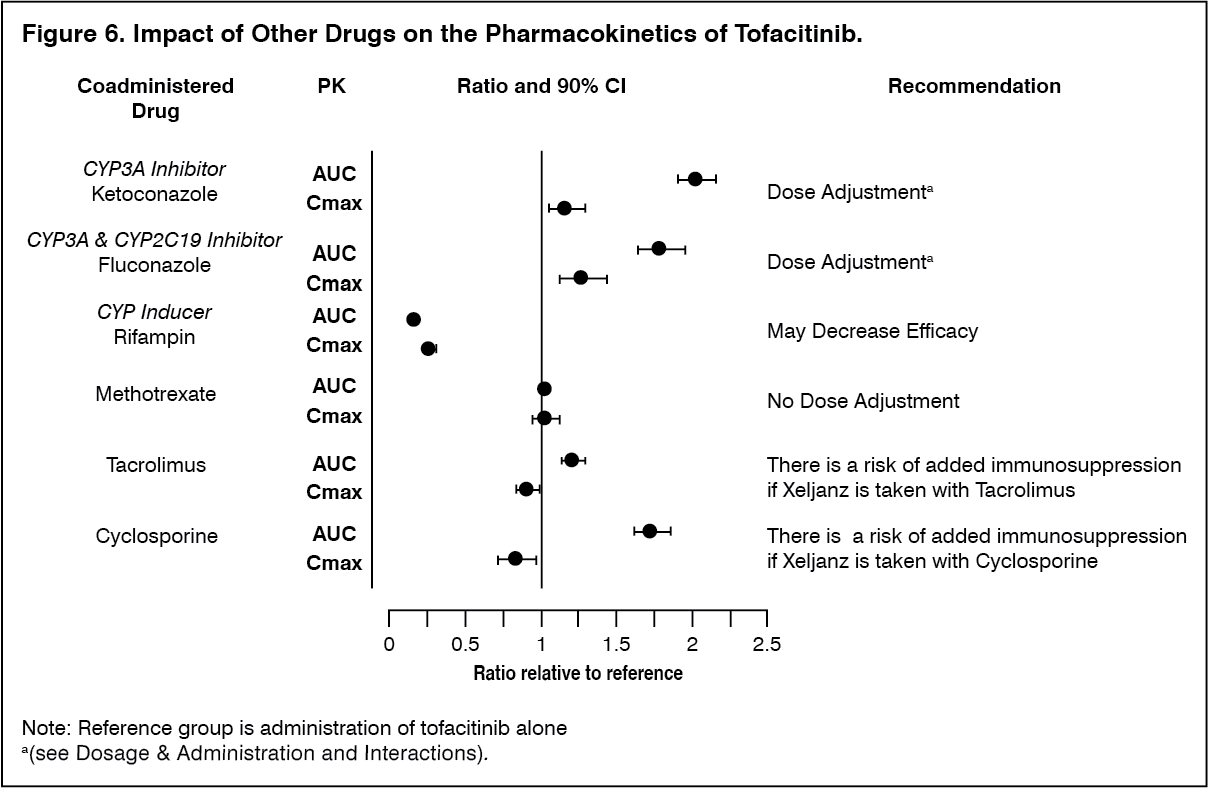 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image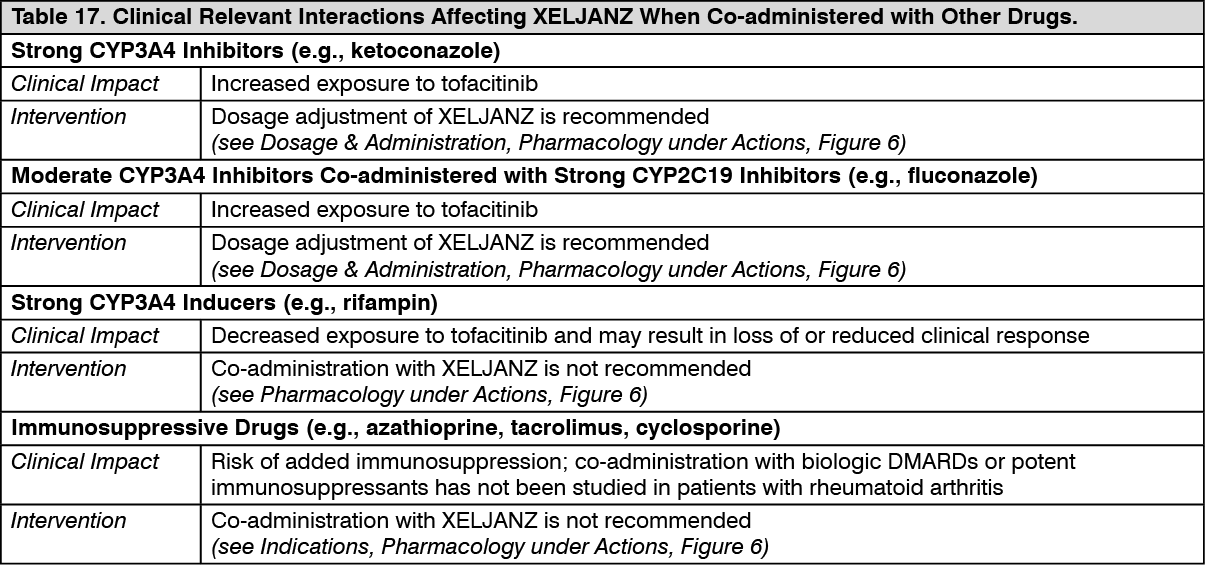 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
