Each immediate-release (IR) tablet contains 0.25 mg, 0.5 mg or 1 mg of alprazolam.
Excipients/Inactive Ingredients: Lactose Monohydrate NF, Docusate Sodium (85%) + Sodium Benzoate (15%), Colloidal Anhydrous Silica NF, Microcrystalline Cellulose NF, Corn Starch NF, Magnesium Stearate NF.
Colouring: Erythrosine Sodium Aluminium Lake (for Xanax Tablets 0.5 mg, 1 mg), FD & C Blue No. 2 Aluminium Lake (for Xanax Tablets 1 mg).
Pharmacotherapeutic group: Benzodiazepine derivatives. ATC code: N05BA12.
Pharmacology: Pharmacodynamics: Alprazolam, like other benzodiazepines, has a high affinity for the benzodiazepine binding site in the brain. It facilitates the inhibitory neurotransmitter action of gamma-aminobutyric acid, which mediates both pre- and post-synaptic inhibition in the central nervous system (CNS).
Pharmacokinetics: Alprazolam is readily absorbed. Following oral administration, peak concentration in the plasma occurs after 1 - 2 hours.
The mean half-life is 12-15 hours. Repeated dosage may lead to accumulation and this should be borne in mind in elderly patients and those with impaired renal or hepatic function. Alprazolam and its metabolites are excreted primarily in the urine.
In vitro, alprazolam is bound (80%) to human serum protein.
Toxicology: Preclinical Safety Data: Mutagenesis: Alprazolam was not mutagenic in the in vitro Ames test. Alprazolam did not produce chromosomal aberrations in the in vivo micronucleus assay in rats up to the highest dose tested of 100 mg/kg, which is 500 times greater than the maximum recommended daily human dose of 10 mg/day.
Carcinogenesis: No evidence of carcinogenic potential was observed during 2-year bioassay studies of alprazolam in rats at doses up to 30 mg/kg/day (150 times the maximum recommended daily human dose of 10 mg/day) and in mice at doses up to 10 mg/kg/day (50 times the maximum recommended daily human dose of 10 mg/day).
Fertility: Alprazolam did not impair fertility in rats up to the highest dose tested of 5 mg/kg/day, which is 25 times the maximum recommended daily human dose of 10 mg/day.
Ocular Effects: When rats were treated orally with alprazolam at 3, 10, and 30 mg/kg/day (15 to 150 times the maximum recommended daily human dose of 10 mg/day) for 2 years, a tendency for a dose related increase in the number of cataracts (females) and corneal vascularization (males) was observed. These lesions did not appear until after 11 months of treatment.
Effect of Anesthetic and Sedative Drugs: Nonclinical research has shown that administration of anesthetic and sedation drugs that block N-methyl-D-aspartate (NMDA) receptors and/or potentiate gamma-aminobutyric acid (GABA) activity can increase neuronal cell death in the brain and result in long term deficits in cognition and behavior of juvenile animals when administered during the period of peak brain development. Based on comparisons across nonclinical species, the window of vulnerability of the brain to these effects is believed to correlate with human exposures in the third trimester of pregnancy through the first year of life, but may extend to approximately 3 years of age. While there is limited information of this effect with alprazolam, since the mechanism of action includes potentiation of GABA activity, a similar effect may occur. The relevance of these nonclinical findings to human use is unknown.
Alprazolam is indicated for the treatment of: Anxiety states (anxiety neuroses): Symptoms which occur in such patients include anxiety, tension, agitation, insomnia, apprehension, irritability and/or autonomic hyperactivity resulting in a variety of somatic complaints.
Mixed anxiety-depression: Symptoms of both anxiety and depression occur simultaneously in such patients.
Neurotic or reactive depression: Such patients primarily exhibit a depressed mood or a pervasive loss of interest or pleasure. Symptoms of anxiety, psychomotor agitation and insomnia are usually present. Other characteristics include appetite disturbances, changes in weight, somatic complaints, cognitive disturbances, decreased energy, feeling of worthlessness or guilt, or thoughts of death or suicide.
Anxiety states, mixed anxiety-depression, or depression associated with other diseases: Such as the chronic phase of alcohol withdrawal and functional or organic disease, particularly certain gastrointestinal, cardiovascular or dermatological disorders.
Panic related disorders: Alprazolam is indicated in the treatment of panic disorder with or without some phobic avoidance. Alprazolam is also indicated for the blocking or attenuation of panic attacks and phobias in patients who have agoraphobia with panic attacks. The effectiveness of alprazolam in the treatment of anxiety, anxiety associated with depression and neurotic (reactive) depression for long-term use exceeding six months has not been established by systematic clinical trials; however, patients with panic-related disorders have been effectively treated for up to eight months. The physician should periodically reassess the usefulness of the drug for the individual patient.
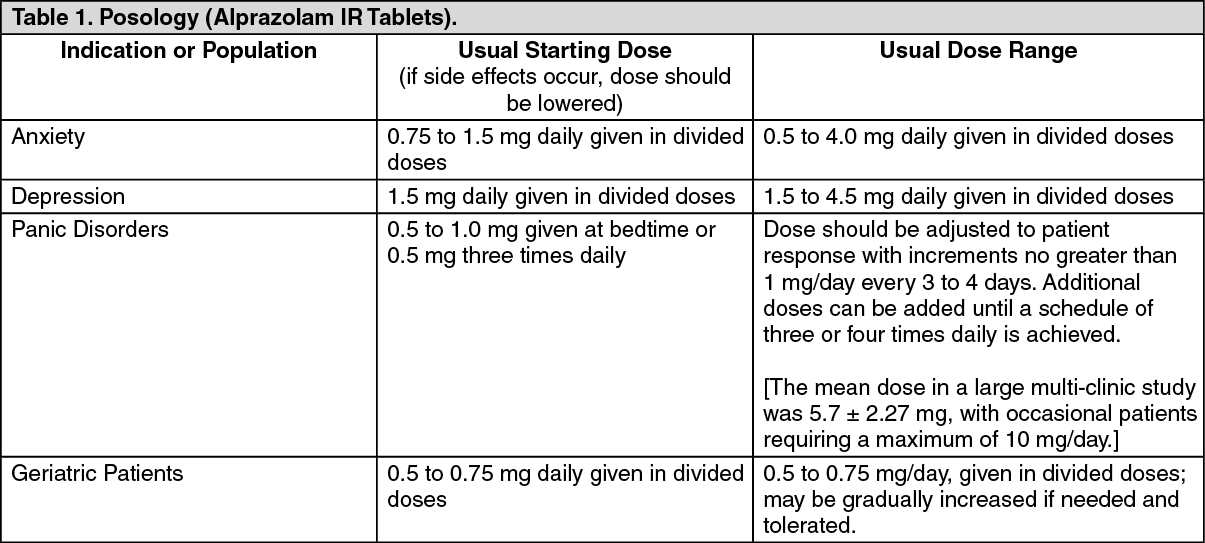
The optimum dose should be individualized based upon the severity of the symptoms and individual patient response. In patients who require higher doses, dosage should be increased cautiously to avoid adverse effects. In general, patients who have not previously received psychotropic medications will require somewhat lower doses than those previously treated with minor tranquilizers, antidepressants, or hypnotics. It is recommended that the general principle of using the lowest effective dose be followed, especially in elderly or debilitated patients to preclude the development of ataxia or oversedation.
Duration of Treatment: The overall duration of treatment should not be more than 8-12 weeks, including a tapering off process.
Discontinuation of Treatment: To discontinue alprazolam treatment, the dosage should be reduced slowly in keeping with good medical practice. It is suggested that the daily dosage of alprazolam be decreased by no more than 0.5 mg every 3 days. Some patients may require an even slower dosage reduction (see Precautions).
Pediatric Use: Safety and efficacy have not been established in children under 18 years of age. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Symptoms of overdose with alprazolam are extensions of its pharmacological action and include drowsiness, slurred speech, motor incoordination, coma and respiratory depression. Serious sequela are rare unless other drugs and/or ethanol are concomitantly ingested. Treatment of overdosage is primarily supportive of respiratory and cardiovascular function. The value of dialysis has not been determined. Flumazenil may be used as an adjunct to the management of respiratory and cardiovascular function associated with overdose.
Alprazolam is contraindicated in patients with known hypersensitivity to benzodiazepines, alprazolam, or to any component of these products' formulations.
Risks from Concomitant Use with Opioids: Profound sedation, respiratory depression, coma, and death may result from the concomitant use of Xanax with opioids. Observational studies have demonstrated that concomitant use of opioids and benzodiazepines increases the risk of drug-related mortality compared to use of opioids alone. Because of these risks, reserve concomitant prescribing of these drugs for use in patients for whom alternative treatment options are inadequate.
If the decision is made to newly prescribe a benzodiazepine and an opioid together, prescribe the lowest effective dosages and minimum durations of concomitant use.
If the decision is made to prescribe a benzodiazepine in a patient already receiving an opioid, prescribe a lower initial dose of the benzodiazepine than indicated in the absence of an opioid, and titrate based on clinical response.
If the decision is made to prescribe an opioid in a patient already taking a benzodiazepine, prescribe a lower initial dose of the opioid, and titrate based on clinical response.
Follow patients closely for signs and symptoms of respiratory depression and sedation. Advise both patients and caregivers about the risks of respiratory depression and sedation when Xanax is used with opioids. Advise patients not to drive or operate heavy machinery until the effects of concomitant use of the opioid have been determined. Screen patients for risk of substance use disorders, including opioid abuse and misuse, and warn them of the risk for overdose and death associated with the use of opioids (see Interactions).
Caution is recommended when treating patients with impaired renal or hepatic function.
Habituation and emotional/physical dependence may occur with benzodiazepines, including alprazolam. As with all benzodiazepines, the risk of dependence increases with higher doses and long-term use and is further increased in patients with a history of alcoholism or drug abuse. Drug abuse is a known risk for alprazolam and other benzodiazepines, and patients should be monitored accordingly when receiving alprazolam. Alprazolam may be subject to diversion. There have been reports of overdose-related deaths when alprazolam is abused with other central nervous system (CNS) depressants including opioids, other benzodiazepines, and alcohol. These risks should be considered when prescribing or dispensing alprazolam. To reduce these risks the smallest appropriate quantity should be used and patients should be advised on the proper storage and disposal of unused drug (see Dosage & Administration, Adverse Reactions and Overdosage).
Withdrawal symptoms have occurred following rapid decrease or abrupt discontinuance of benzodiazepines including alprazolam. These can range from mild dysphoria and insomnia to a major syndrome which may include abdominal and muscle cramps, vomiting, sweating, tremor, and convulsions. In addition, withdrawal seizures have occurred upon rapid decrease or abrupt discontinuation of therapy with alprazolam (see Discontinuation of Treatment under Dosage & Administration and Adverse Reactions).
Panic disorders have been associated with primary and secondary major depressive disorders and increased reports of suicide among untreated patients. Therefore, the same precaution must be exercised when using the higher doses of alprazolam in treating patients with panic disorders as is exercised with the use of any psychotropic drug in treating depressed patients or those in whom there is reason to expect concealed suicidal ideation or plans.
Administration to severely depressed or suicidal patients should be done with appropriate precautions and appropriate size of the prescription.
Episodes of hypomania and mania have been reported in association with the use of alprazolam in patients with depression.
The use of alprazolam has not been established in certain types of depression (see Indications/Uses).
Anaphylaxis (severe allergic reaction) and angioedema (severe facial swelling) which can occur as early as the first time the product is taken.
Complex sleep - related behaviors which may include sleep driving, making phone calls, preparing and eating food while asleep.
Effects on Ability to Drive and Use Machines: Patients should be cautioned about using alprazolam while operating motor vehicles or engaging in other dangerous activities until it is established that they do not become impaired while receiving the drug.
Pregnancy: The data concerning teratogenicity and effects on post-natal development and behavior following benzodiazepine treatment are inconsistent. There is evidence from some early studies with other members of the benzodiazepine class that in utero exposure may be associated with malformations. Later studies with the benzodiazepine class of drugs have provided no clear evidence of any type of defect. Infants exposed to benzodiazepines during late third trimester of pregnancy or during labor have been reported to exhibit either the floppy infant syndrome or neonatal withdrawal symptoms. If alprazolam is used during pregnancy, or if the patient becomes pregnant while taking alprazolam, the patient should be apprised of the potential hazard to the fetus.
Breastfeeding: Levels of benzodiazepines, including alprazolam, in breast milk are low. However, nursing should not be undertaken while using benzodiazepines.
Adverse events, if they occur, are generally observed at the beginning of therapy and usually disappear upon continued medication or decreased dosage.
Undesirable effects associated with alprazolam therapy in patients participating in controlled clinical studies and with post-marketing experience are as follows: (See Table 2).
Click on icon to see table/diagram/image
In many of the spontaneous case reports of adverse behavioral effects, patients were receiving other CNS drugs concomitantly and/or were described as having underlying psychiatric conditions. Patients who have borderline personality disorder, a prior history of violent or aggressive behavior, or alcohol or substance abuse may be at risk for such events. Instances of irritability, hostility and intrusive thoughts have been reported during discontinuance of alprazolam in patients with post-traumatic stress disorder.
Opioids: Due to additive pharmacologic effect, the concomitant use of opioids with benzodiazepines increases the risk of respiratory depression, profound sedation, coma and death.
The concomitant use of opioids and benzodiazepines increases the risk of respiratory depression because of actions at different receptor sites in the central nervous system that control respiration. Opioids interact primarily at μ-receptors, and benzodiazepines interact at GABAA sites. When opioids and benzodiazepines are combined, the potential for benzodiazepines to significantly worsen opioid-related respiratory depression exists.
Reserve concomitant prescribing of these drugs for use in patients for whom alternative treatment options are inadequate (see Precautions).
Limit dosage and duration of concomitant use of benzodiazepines and opioids, and follow patients closely for respiratory depression and sedation.
Benzodiazepines produce additive CNS depressant effects when co-administered with alcohol or other drugs producing CNS depression (see Precautions).
Pharmacokinetic interactions can occur when alprazolam is administered along with drugs that interfere with its metabolism. Compounds which inhibit certain hepatic enzymes (particularly cytochrome P4503A4) may increase the concentration of alprazolam and enhance its activity. Data from clinical studies with alprazolam, in vitro studies with alprazolam, and clinical studies with drugs metabolized similarly to alprazolam provide evidence for varying degrees of interaction and possible interaction with alprazolam for a number of drugs. Based on the degree of interaction and the type of data available, the following recommendations are made: The co-administration of alprazolam with ketoconazole, itraconazole, or other azole-type antifungals is not recommended.
Caution and consideration of dose reduction is recommended when alprazolam is co-administered with nefazodone, fluvoxamine, and cimetidine.
Caution is recommended when alprazolam is co-administered with fluoxetine, propoxyphene, oral contraceptives, diltiazem, or macrolide antibiotics such as erythromycin and troleandomycin.
Interactions involving human immunodeficiency virus (HIV) protease inhibitors (e.g., ritonavir) and alprazolam are complex and time dependent. Low doses of ritonavir resulted in a large impairment of alprazolam clearance, prolonged its elimination half-life and enhanced clinical effects. However, upon extended exposure to ritonavir, CYP3A induction offset this inhibition. This interaction will require a dose-adjustment or discontinuation of alprazolam.
Increased digoxin concentrations have been reported when alprazolam was given, especially in elderly (>65 years of age). Patients who receive alprazolam and digoxin should therefore be monitored for signs and symptoms related to digoxin toxicity.
Special Precautions for Disposal of a Used Medicinal Product or Waste Materials Derived from such Medicinal Product and Other Handling of the Product: Not applicable.
Incompatibilities: Not applicable.
This medicinal product does not require any special storage conditions.
Storage condition: Do not store above 30°C.
Shelf-Life: 3 years.
N05BA12 - alprazolam ; Belongs to the class of benzodiazepine derivatives anxiolytics. Used in the management of anxiety, agitation or tension.
Xanax tab 0.5 mg
100's;5 × 100's (RM430.7/box)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image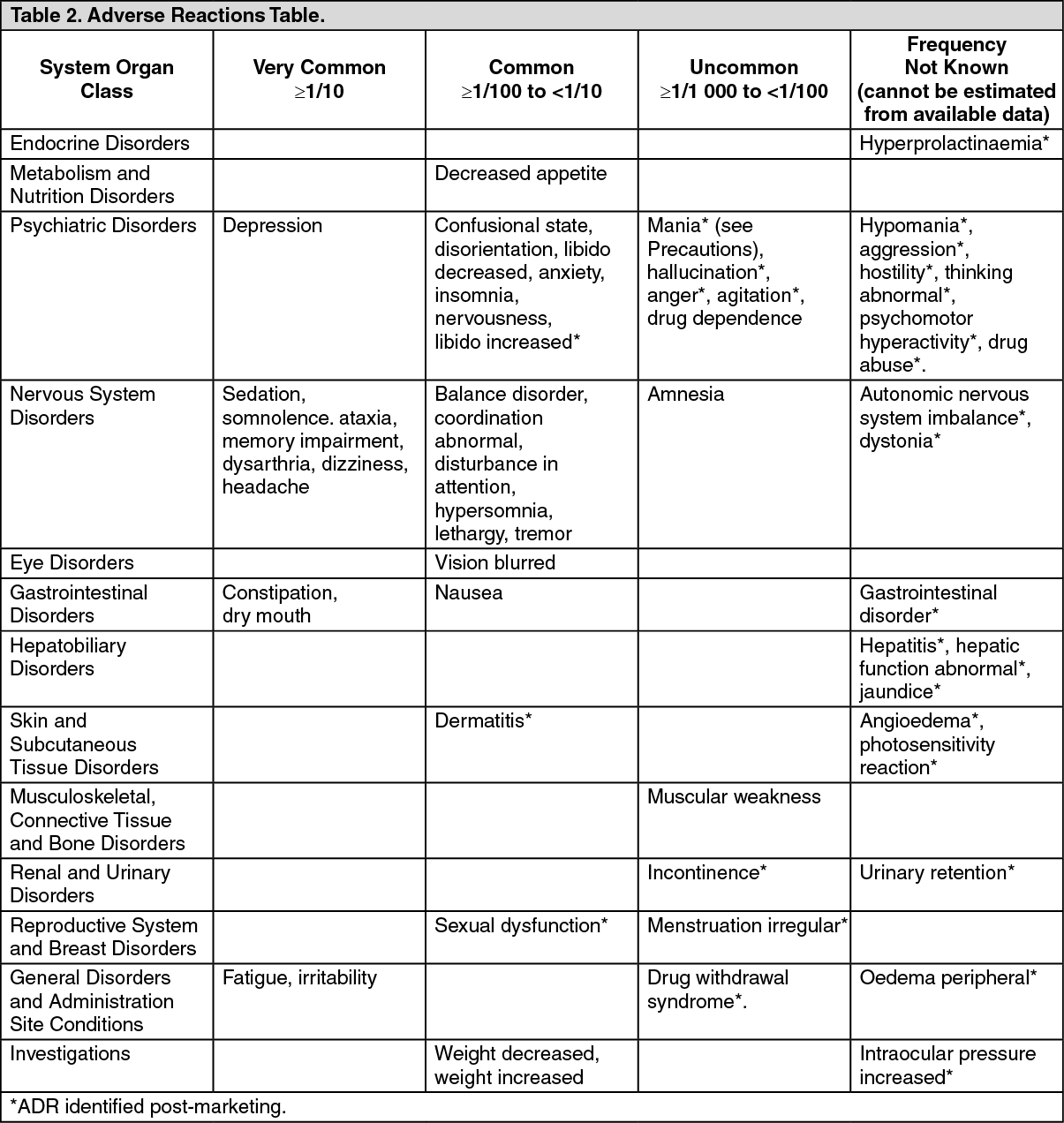 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
