


 Sign Out
Sign Out

Interstitial Lung Disease/Pneumonitis [see Interstitial Lung Disease/Pneumonitis under Precautions].
QT Interval Prolongation [see QT Interval Prolongation under Precautions].
Cardiac Failure [see Cardiac Failure under Precautions].
Bradycardia [see Bradycardia under Precautions].
Severe Visual Loss [see Severe Visual Loss under Precautions].
Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The data in Precautions reflect exposure to XALKORI in 1719 with NSCLC patients who received XALKORI 250 mg twice daily enrolled on Studies 1 (including an additional 109 patients who crossed over from the control arm), 2, 3, a single arm trial (n=1063) of ALK-positive NSCLC, and an additional ALK-positive NSCLC expansion cohort of a dose finding study (n=154).
ALK- or ROS1-Positive Metastatic NSCLC: The data described as follows is based primarily on 343 patients with ALK-positive metastatic NSCLC who received XALKORI 250 mg orally twice daily from 2 open-label, randomized, active-controlled trials (Studies 1 and 2). The safety of XALKORI was also evaluated in 50 patients with ROS1 positive metastatic NSCLC from a single-arm study (Study 3).
The most common adverse reactions (≥25%) of XALKORI in patients with NSCLC are vision disorders, nausea, diarrhea, vomiting, edema, constipation, elevated transaminases, fatigue, decreased appetite, upper respiratory infection, dizziness, and neuropathy.
Previously Untreated ALK-Positive Metastatic NSCLC - Study 1 (PROFILE 1014): The data in Table 3 are derived from 340 patients with ALK-positive metastatic NSCLC who had not received previous systemic treatment for advanced disease who received treatment in a randomized, multicenter, open-label, active-controlled trial (Study 1). Patients in the XALKORI arm (n=171) received XALKORI 250 mg orally twice daily until documented disease progression, intolerance to therapy, or the investigator determined that the patient was no longer experiencing clinical benefit. A total of 169 patients in the chemotherapy arm received pemetrexed 500 mg/m2 with cisplatin 75 mg/m2 (n=91) or carboplatin at a dose calculated to produce an AUC of 5 or 6 mg × min/mL (n=78). Chemotherapy was given by intravenous infusion every 3 weeks for up to 6 cycles, in the absence of dose-limiting chemotherapy-related toxicities. After 6 cycles, patients remained on study with no additional anticancer treatment, and tumor assessments continued until documented disease progression.
The median duration of study treatment was 10.9 months for patients in the XALKORI arm and 4.1 months for patients in the chemotherapy arm. Median duration of treatment was 5.2 months for patients who received XALKORI after cross over from chemotherapy. Across the 340 patients who were treated in Study 1, the median age was 53 years; 16% of patients were older than 65 years. A total of 62% of patients were female and 46% were Asian.
Serious adverse events were reported in 34% of patients treated with XALKORI. The most frequent serious adverse events reported in patients treated with XALKORI were dyspnea (4.1%) and pulmonary embolism (2.9%). Fatal adverse events in XALKORI-treated patients occurred in 2.3% patients, consisting of septic shock, acute respiratory failure, and diabetic ketoacidosis.
Dose reductions due to adverse reactions were required in 6% of XALKORI-treated patients. The most frequent adverse reactions that led to dose reduction in these patients were nausea (1.8%) and elevated transaminases (1.8%).
Permanent discontinuation of XALKORI treatment for adverse reactions was 8%. The most frequent adverse reactions that led to permanent discontinuation in XALKORI-treated patients were elevated transaminases (1.2%), hepatotoxicity (1.2%), and ILD (1.2%).
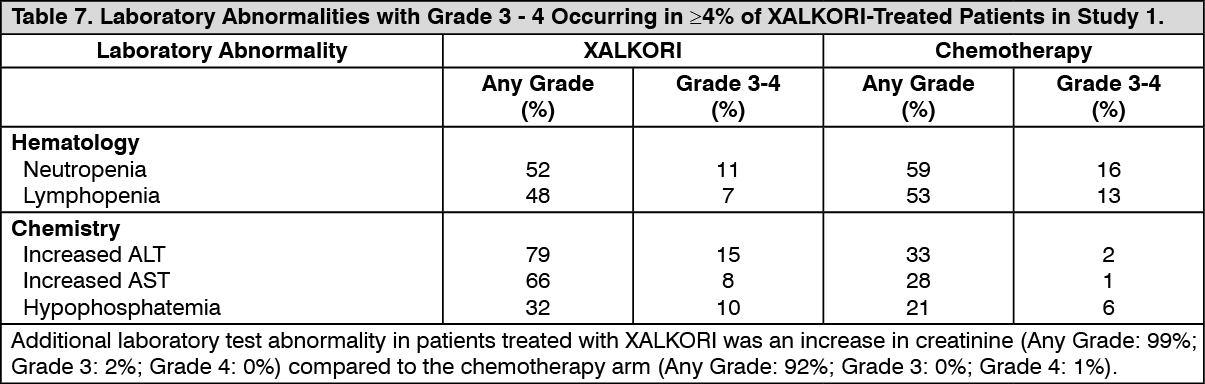
Tables 6 and 7 summarize common adverse reactions and laboratory abnormalities in XALKORI-treated patients. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional adverse reactions occurring at an overall incidence between 1% and 60% in patients treated with XALKORI included nausea (56%), decreased appetite (30%), fatigue (29%), neuropathy (21%; gait disturbance, hypoesthesia, muscular weakness, neuralgia, neuropathy peripheral, paresthesia, peripheral sensory neuropathy, polyneuropathy, sensory disturbance), rash (11%), renal cyst (5%), ILD (1%; ILD, pneumonitis), syncope (1%), and decreased blood testosterone (1%; hypogonadism).
Clinically relevant adverse reactions in <1% of patients who received XALKORI included photosensitivity (0.3%). (See Table 7.)
 Click on icon to see table/diagram/image
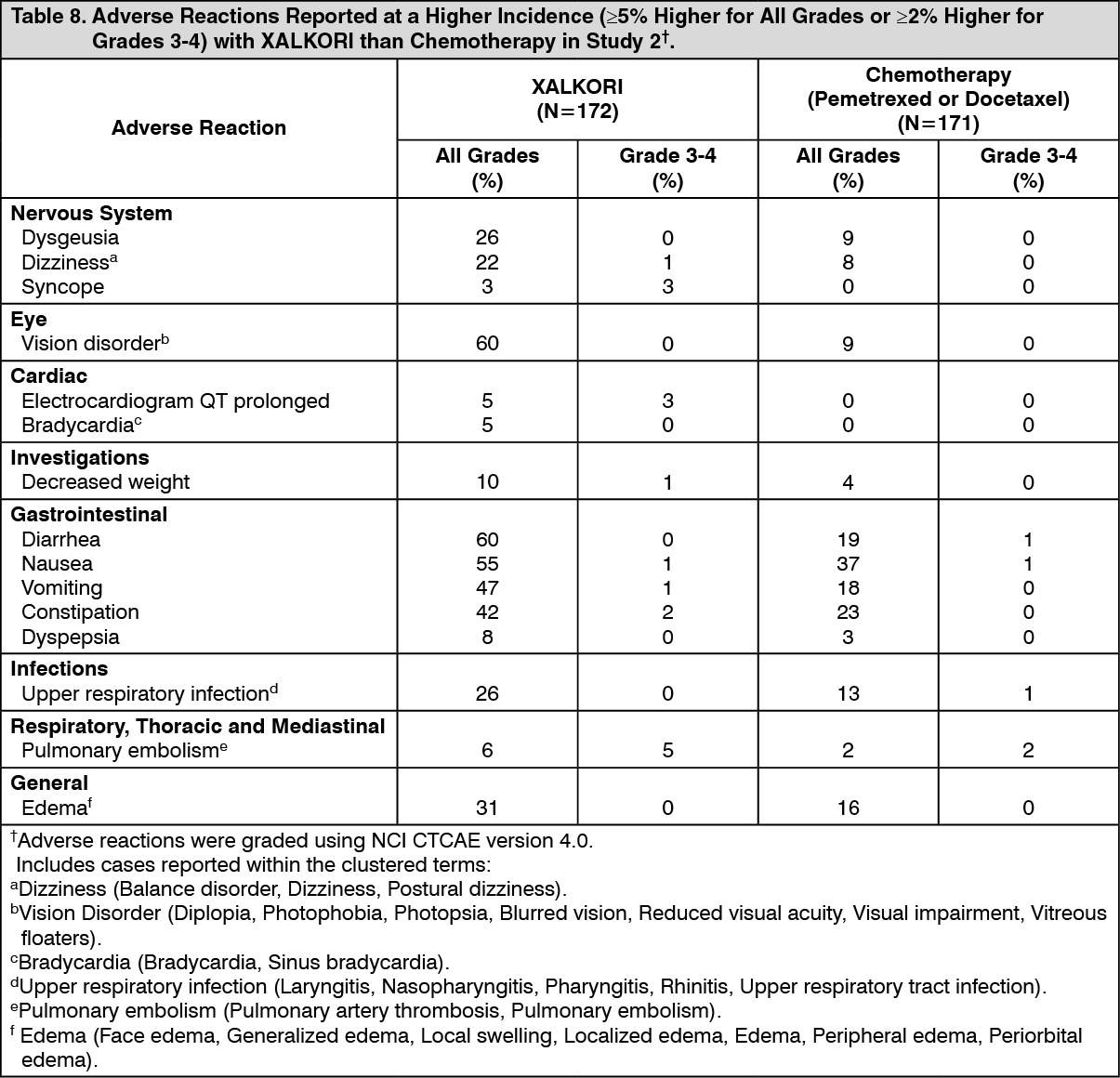
Click on icon to see table/diagram/imagePreviously Treated ALK-Positive Metastatic NSCLC - Study 2 (PROFILE 1007): The data in Table 8 are derived from 343 patients with ALK-positive metastatic NSCLC enrolled in a randomized, multicenter, active-controlled, open-label trial (Study 2). Patients in the XALKORI arm (n=172) received XALKORI 250 mg orally twice daily until documented disease progression, intolerance to therapy, or the investigator determined that the patient was no longer experiencing clinical benefit. A total of 171 patients in the chemotherapy arm received pemetrexed 500 mg/m2 (n=99) or docetaxel 75 mg/m2 (n=72) by intravenous infusion every 3 weeks until documented disease progression, intolerance to therapy, or the investigator determined that the patient was no longer experiencing clinical benefit. Patients in the chemotherapy arm received pemetrexed unless they had received pemetrexed as part of first-line or maintenance treatment.
The median duration of study treatment was 7.1 months for patients who received XALKORI and 2.8 months for patients who received chemotherapy. Across the 347 patients who were randomized to study treatment (343 received at least 1 dose of study treatment), the median age was 50 years; 14% of patients were older than 65 years. A total of 56% of patients were female and 45% of patients were Asian.
Serious adverse reactions were reported in 37% of patients treated with XALKORI and 23% of patients in the chemotherapy arm. The most frequent serious adverse reactions reported in patients treated with XALKORI were pneumonia (4.1%), pulmonary embolism (3.5%), dyspnea (2.3%), and ILD (2.9%). Fatal adverse reactions in XALKORI-treated patients in Study 2 occurred in 5% of patients, consisting of: acute respiratory distress syndrome, arrhythmia, dyspnea, pneumonia, pneumonitis, pulmonary embolism, ILD, respiratory failure and sepsis.
Dose reductions due to adverse reactions were required in 16% of XALKORI-treated patients. The most frequent adverse reactions that led to dose reduction in the patients treated with XALKORI were increased ALT (8%) including some patients with concurrent increased AST, QTc prolongation (2.9%), and neutropenia (2.3%).
XALKORI was discontinued for adverse reactions in 15% of patients. The most frequent adverse reactions that led to discontinuation of XALKORI were ILD (1.7%), increased ALT and AST (1.2%), dyspnea (1.2%), and pulmonary embolism (1.2%).
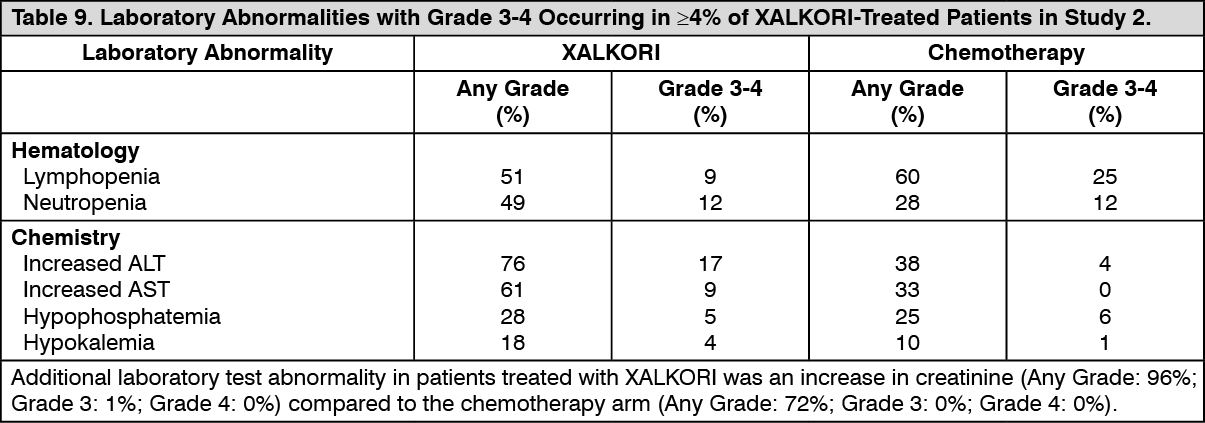
Tables 8 and 9 summarize common adverse reactions and laboratory abnormalities in XALKORI-treated patients. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional adverse reactions occurring at an overall incidence between 1% and 30% in patients treated with XALKORI included decreased appetite (27%), fatigue (27%), neuropathy (19%; dysesthesia, gait disturbance, hypoesthesia, muscular weakness, neuralgia, peripheral neuropathy, paresthesia, peripheral sensory neuropathy, polyneuropathy, burning sensation in skin), rash (9%), ILD (4%; acute respiratory distress syndrome, ILD, pneumonitis), renal cyst (4%), esophagitis (2%), hepatic failure (1%), and decreased blood testosterone (1%; hypogonadism).
Clinically relevant adverse reactions in <1% of patients who received XALKORI included photosensitivity (0.4%). (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageROS1-Positive Metastatic NSCLC - Study 3 (PROFILE 1001): The safety profile of XALKORI from Study 3, which was evaluated in 50 patients with ROS1-positive metastatic NSCLC, was generally consistent with the safety profile of XALKORI evaluated in patients with ALK-positive metastatic NSCLC (n=1669). Vision disorders occurred in 92% of patients in Study 3; 90% were Grade 1 and 2% were Grade 2. The median duration of exposure to XALKORI was 34.4 months.
Description of Selected Adverse Reactions: Vision disorders: Vision disorders, most commonly visual impairment, photopsia, blurred vision, or vitreous floaters, occurred in 63% of 1719 patients. The majority (95%) of these patients had Grade 1 visual adverse reactions. There were 0.8% of patients with Grade 3 and 0.2% of patients with Grade 4 visual impairment.
Based on the Visual Symptom Assessment Questionnaire (VSAQ-ALK), patients treated with XALKORI in Studies 1 and 2 reported a higher incidence of visual disturbances compared to patients treated with chemotherapy. The onset of vision disorder generally was within the first week of drug administration. The majority of patients on the XALKORI arms in Studies 1 and 2 (>50%) reported visual disturbances which occurred at a frequency of 4-7 days each week, lasted up to 1 minute, and had mild or no impact (scores 0 to 3 out of a maximum score of 10) on daily activities as captured in the VSAQ-ALK questionnaire.
Neuropathy: Neuropathy, most commonly sensory in nature, occurred in 25% of 1719 patients. Most events (95%) were Grade 1 or Grade 2 in severity.
Renal cysts: Renal cysts were experienced by 3.0% of 1719 patients.
The majority of renal cysts in XALKORI-treated patients were complex. Local cystic invasion beyond the kidney occurred, in some cases with imaging characteristics suggestive of abscess formation. However, across clinical trials no renal abscesses were confirmed by microbiology tests.
Renal toxicity: The estimated glomerular filtration rate (eGFR) decreased from a baseline median of 96.42 mL/min/1.73 m2 (n=1681) to a median of 80.23 mL/min/1.73 m2 at 2 weeks (n=1499) in patients with ALK-positive advanced NSCLC who received XALKORI in clinical trials. No clinically relevant changes occurred in median eGFR from 12 to 104 weeks of treatment. Median eGFR slightly increased (83.02 mL/min/1.73 m2) 4 weeks after the last dose of XALKORI. Overall, 76% of patients had a decrease in eGFR to <90 mL/min/1.73 m2, 38% had a decrease to eGFR to <60 mL/min/1.73 m2, and 3.6% had a decrease to eGFR to <30 mL/min/1.73 m2.
Postmarketing Experience: The following additional adverse reaction has been identified during post approval use of XALKORI. Because this reaction is reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate the frequency or establish a causal relationship to drug exposure.
Investigations: Increased blood creatine phosphokinase.
View ADR Monitoring Form