Pharmacology: Pharmacodynamics: Mechanism of action: Voriconazole is a triazole antifungal agent. The primary mode of action of voriconazole is the inhibition of fungal cytochrome P 450-mediated 14 alpha-lanosterol demethylations, an essential step in fungal ergosterol biosynthesis. The accumulation of 14 alpha-methyl sterols correlates with the subsequent loss of ergosterol in the fungal cell membrane and may be responsible for the antifungal activity of voriconazole. Voriconazole has been shown to be more selective for fungal cytochrome P-450 enzymes than for various mammalian cytochrome P-450 enzyme systems.
Clinical efficacy and safety: In vitro, voriconazole displays broad-spectrum antifungal activity with antifungal potency against
Candida species (including fluconazole resistant
C. krusei and resistant strains of
C. glabrata and
C. albicans) and fungicidal activity against all
Aspergillus species tested. In addition, voriconazole shows
in vitro fungicidal activity against emerging fungal pathogens, including those such as Scedosporium or Fusarium which have limited susceptibility to existing antifungal agents.
Clinical efficacy defined as a partial or complete response has been demonstrated for
Aspergillus spp. including
A. flavus, A. fumigatus, A. terreus, A. niger, A. nidulans, Candida spp., including
C. albicans, C. glabrata, C. krusei, C. parapsilosis and
C. tropicalis and limited numbers of
C. dubliniensis, C. inconspicua, and
C. guilliermondii, Scedosporium spp., including
S. apiospermum, S. prolificans and
Fusarium spp.
Other treated fungal infections (often with either partial or complete response) included isolated cases of
Alternaria spp.,
Blastomyces dermatitidis, Blastoschizomyces capitatus, Cladosporium spp.,
Coccidioides immitis, Conidiobolus coronatus, Cryptococcus neoformans, Exserohilum rostratum, Exophiala spinifera, Fonsecaea pedrosoi, Madurella mycetomatis, Paecilomyces lilacinus, Penicillium spp. including
P. marneffei, Phialophora richardsiae, Scopulariopsis brevicaulis and
Trichosporon spp. including
T. beigelii infections.
In vitro activity against clinical isolates has been observed for
Acremonium spp.,
Alternaria spp.,
Bipolaris spp.,
Cladophialophora spp., and
Histoplasma capsulatum, with most strains being inhibited by concentrations of voriconazole in the range 0.05 to 2 μg/ml.
In vitro activity against the following pathogens has been shown, but the clinical significance is unknown:
Curvularia spp. and
Sporothrix spp.
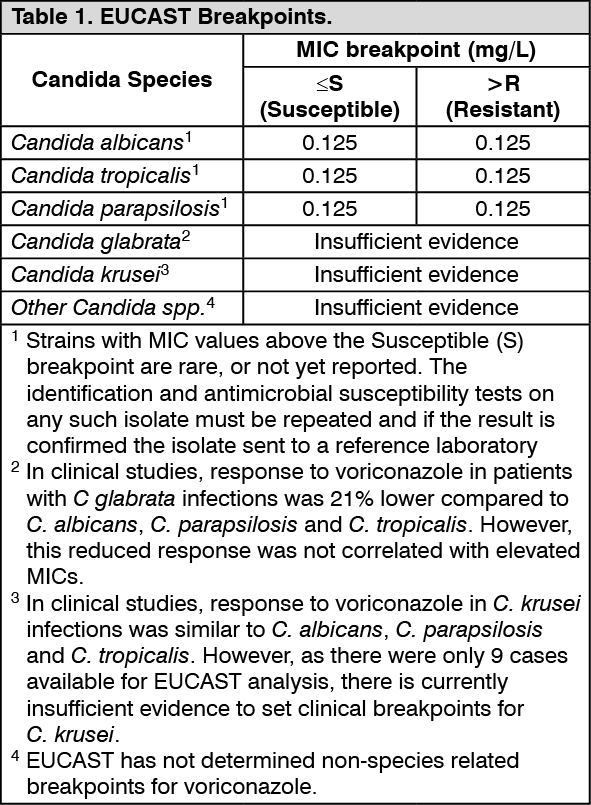
Breakpoints: Specimens for fungal culture and other relevant laboratory studies (serology, histopathology) should be obtained prior to therapy to isolate and identify causative organisms. Therapy may be instituted before the results of the cultures and other laboratory studies are known; however, once these results become available, anti-infective therapy should be adjusted accordingly.
The species most frequently involved in causing human infections include
C. albicans, C. parapsilosis, C. tropicalis, C. glabrata and
C. krusei, all of which usually exhibit minimal inhibitory concentration (MICs) of less than 1 mg/L for voriconazole.
However, the
in vitro activity of voriconazole against
Candida species is not uniform. Specifically, for
C. glabrata, the MICs of voriconazole for fluconazole-resistant isolates are proportionally higher than are those of fluconazole-susceptible isolates. Therefore, every attempt should be made to identify Candida to species level. If antifungal susceptibility testing is available, the MIC results may be interpreted using breakpoint criteria established by the European Committee on Antimicrobial Susceptibility Testing (EUCAST). (See Table 1.)
 Click on icon to see table/diagram/image
Pharmacokinetics: General pharmacokinetic characteristics:
Click on icon to see table/diagram/image
Pharmacokinetics: General pharmacokinetic characteristics: The pharmacokinetics of voriconazole are non-linear due to saturation of its metabolism. Greater than proportional increase in exposure is observed with increasing dose. It is estimated that, on average, increasing the oral dose from 200 mg twice daily to 300 mg twice daily leads to a 2.5-fold increase in exposure (AUCτ). The oral maintenance dose of 200 mg (or 100 mg for patients less than 40 kg) achieves a voriconazole exposure similar to 3 mg/kg IV. A 300 mg (or 150 mg for patients less than 40 kg) oral maintenance dose achieves an exposure similar to 4 mg/kg IV. When the recommended intravenous or oral loading dose regimens are administered, plasma concentrations close to steady state are achieved within the first 24 hours of dosing. Without the loading dose, accumulation occurs during twice-daily multiple dosing with steady-state plasma voriconazole concentrations being achieved by Day 6 in the majority of patients.
Long-term safety of hydroxypropylbetadex in humans is limited to 21 days (250 mg/kg/day).
Absorption: Voriconazole is rapidly and almost completely absorbed following oral administration, with maximum plasma concentrations (C
max) achieved 1-2 hours after dosing. The absolute bioavailability of voriconazole after oral administration is estimated to be 96%. When multiple doses of voriconazole are administered with high-fat meals, C
max and AUCτ are reduced by 34% and 24%, respectively. The absorption of voriconazole is not affected by changes in gastric pH.
Distribution: The volume of distribution at steady state for voriconazole is estimated to be 4.6 L/kg, suggesting extensive distribution into tissues. Plasma protein binding is estimated to be 58%.
Biotransformation: Voriconazole is metabolised by the hepatic cytochrome P 450 isoenzymes, CYP2C19, CYP2C9 and CYP3A4.
The inter-individual variability of voriconazole pharmacokinetics is high.
The major metabolite of voriconazole is the N-oxide, which accounts for 72% of the circulating radiolabelled metabolites in plasma. This metabolite has minimal antifungal activity and does not contribute to the overall efficacy of voriconazole.
Elimination: Voriconazole is eliminated via hepatic metabolism with less than 2% of the dose excreted unchanged in the urine.
After administration of a radiolabelled dose of voriconazole, approximately 80% of the radioactivity is recovered in the urine after multiple intravenous dosing and 83% in the urine after multiple oral dosing. The majority (>94%) of the total radioactivity is excreted in the first 96 hours after both oral and intravenous dosing.
The terminal half-life of voriconazole depends on dose and is approximately 6 hours at 200 mg (orally).
Because of non-linear pharmacokinetics, the terminal half-life is not useful in the prediction of the accumulation or elimination of voriconazole.
Pharmacokinetics in special patient groups: Gender: The safety profile and plasma concentrations observed in male and female were similar. Therefore, no dosage adjustment based on gender is necessary.
Older people: A relationship between plasma concentrations and age was observed. The safety profile of voriconazole in young and elderly patients was similar and, therefore, no dosage adjustment is necessary for the older (see Dosage & Administration).
Paediatric population: The higher intravenous maintenance dose in paediatric relative to adults reflects the higher elimination capacity in paediatric patients due to a greater liver mass to body mass ratio. Oral bioavailability may, however, be limited in paediatric patients with malabsorption and very low body weight for their age. In that case, intravenous voriconazole administration is recommended. Based on the population pharmacokinetic analysis, 12- to 14-year-old adolescents weighing less than 50 kg should receive children's doses (see Dosage & Administration).
Renal impairment: The plasma protein binding of voriconazole was similar with different degrees of renal impairment. See Dosage & Administration and Precautions.
In patients with normal renal function, the pharmacokinetic profile of hydroxypropylbetadex, an ingredient of Voriconazole 200 mg powder for solution for infusion, has a short half-life of 1 to 2 hours and demonstrates no accumulation following successive daily doses. In patients with mild to severe renal insufficiency, the majority (>85%) of an 8 g dose of hydroxypropylbetadex is eliminated in the urine. In patients with mild, moderate, and severe renal impairment, half-life values were increased over normal values by approximately two-, four-, and six-fold, respectively. In these patients, successive infusions may result in accumulation of hydroxypropylbetadex until steady state is reached. Hydroxypropylbetadex is removed by haemodialysis, with a clearance of 37.5 ± 24 ml/min.
Hepatic impairment: Protein binding of voriconazole was not affected by impaired hepatic function. (See Dosage & Administration and Precautions.)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image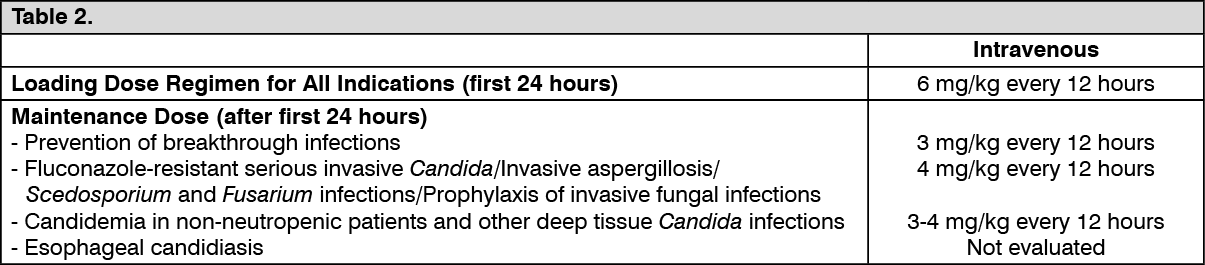 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image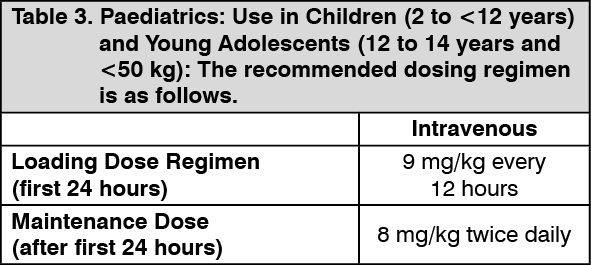 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image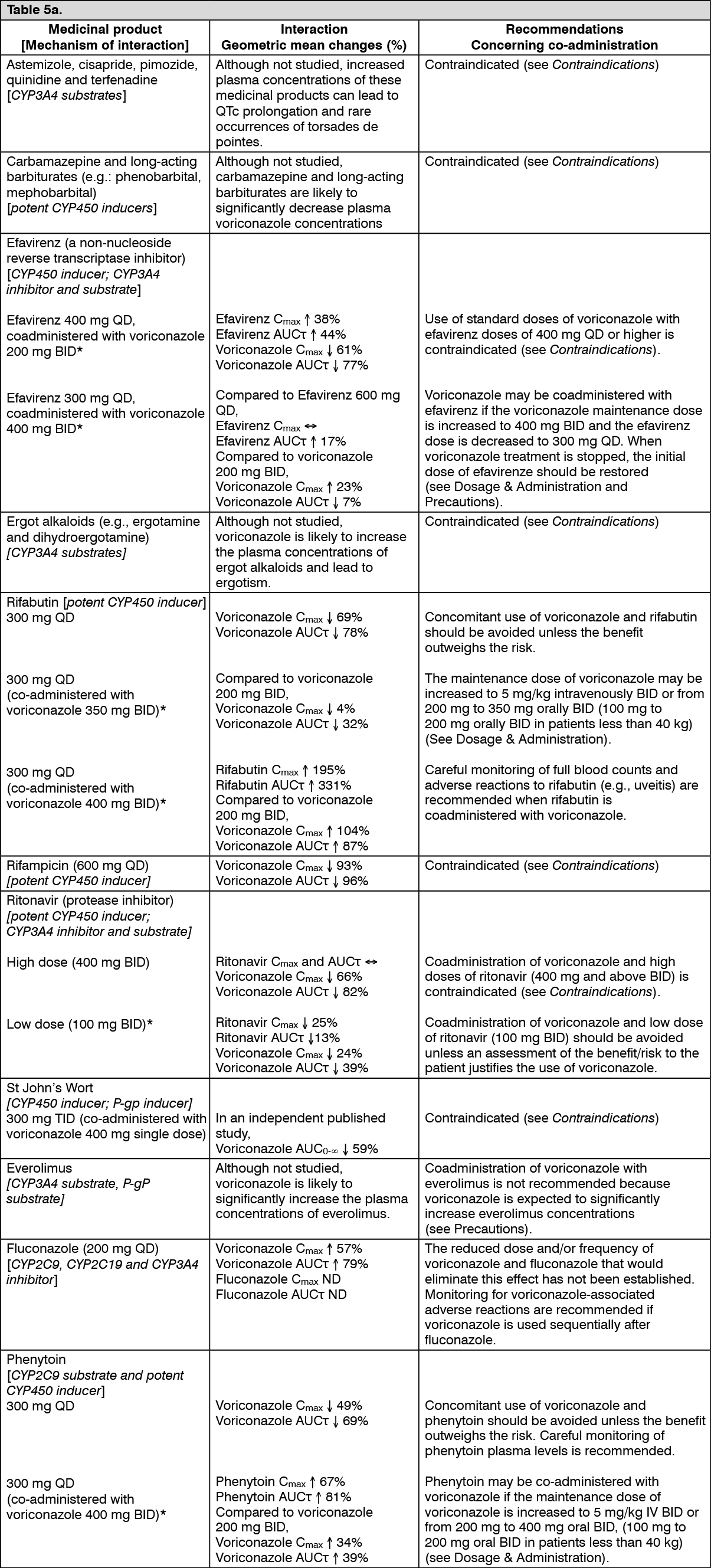 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image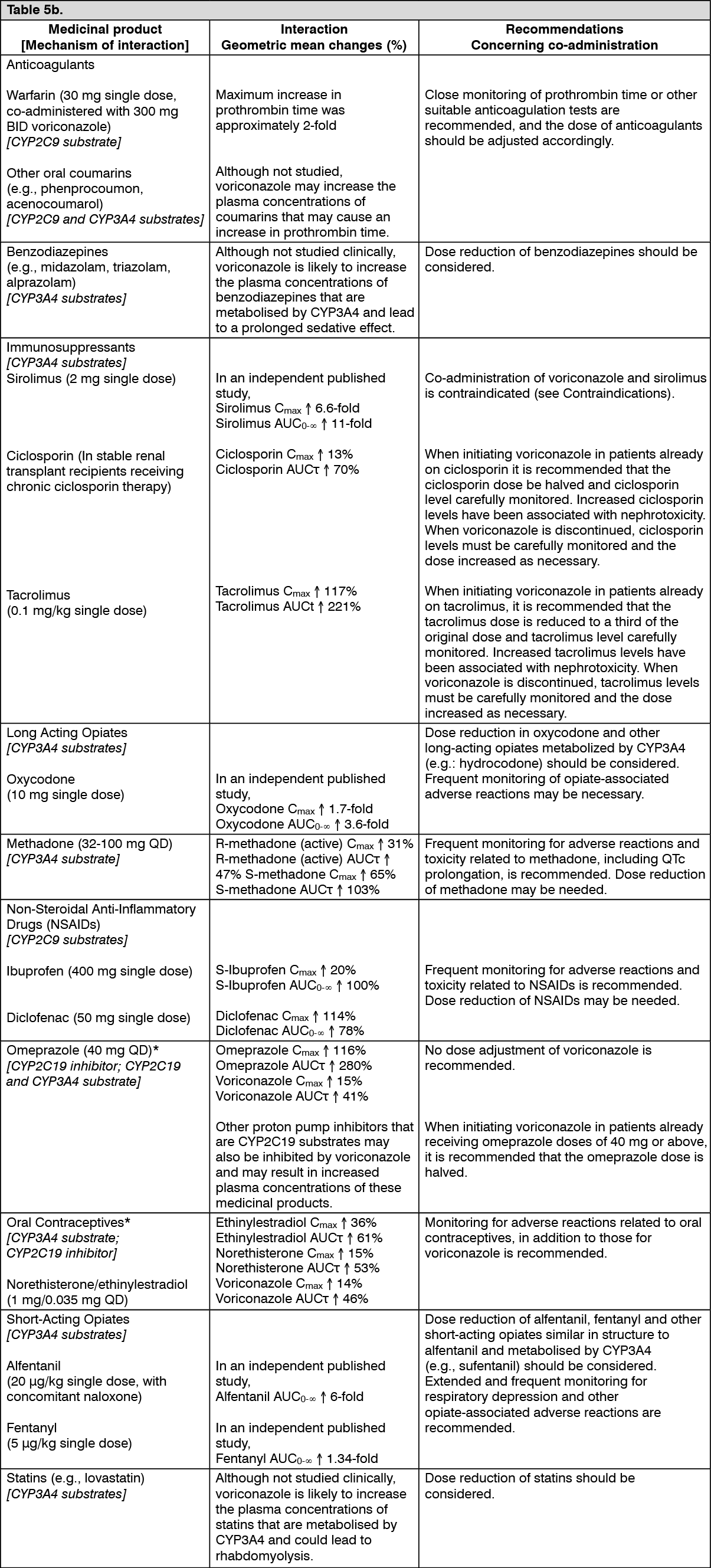 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image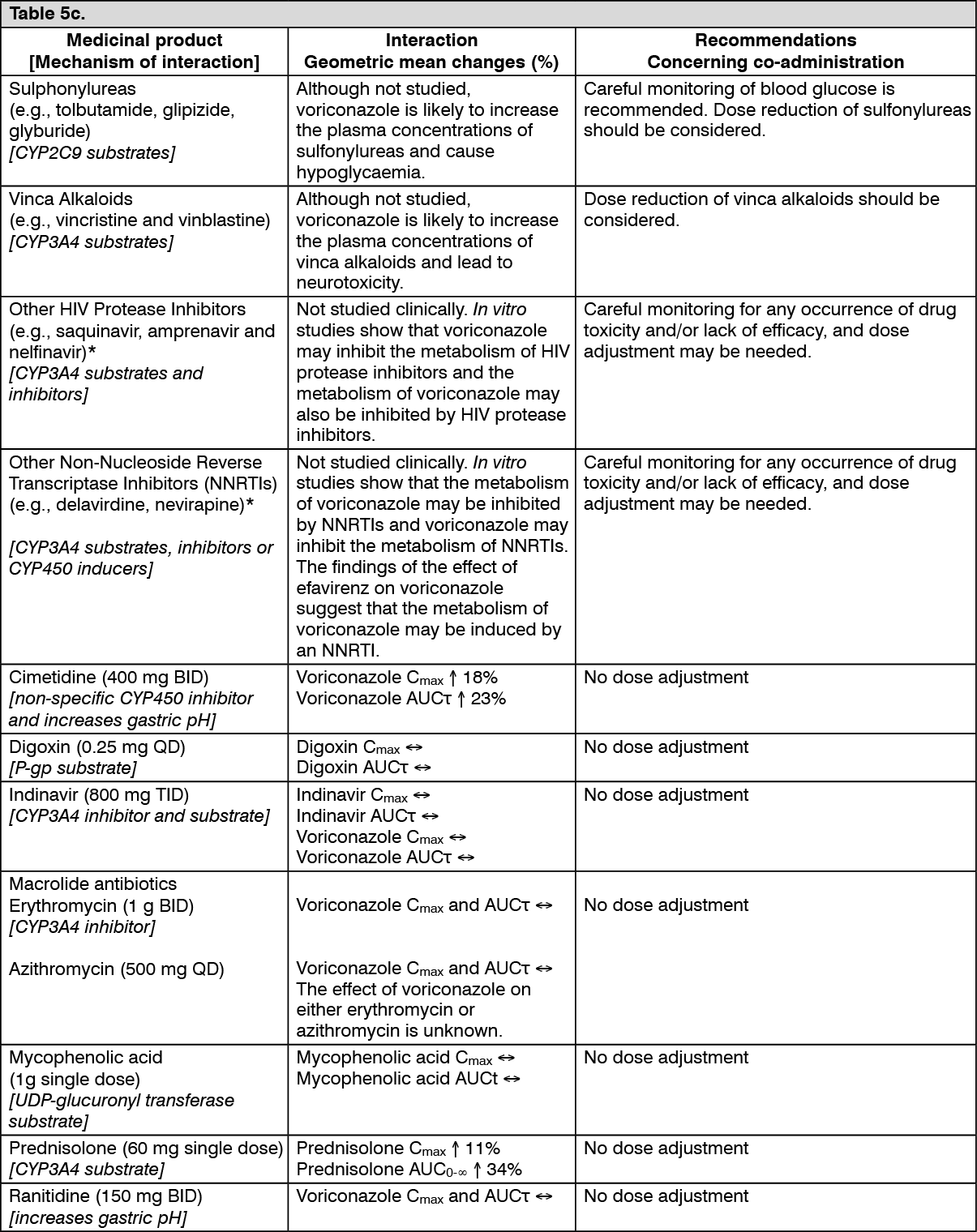 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image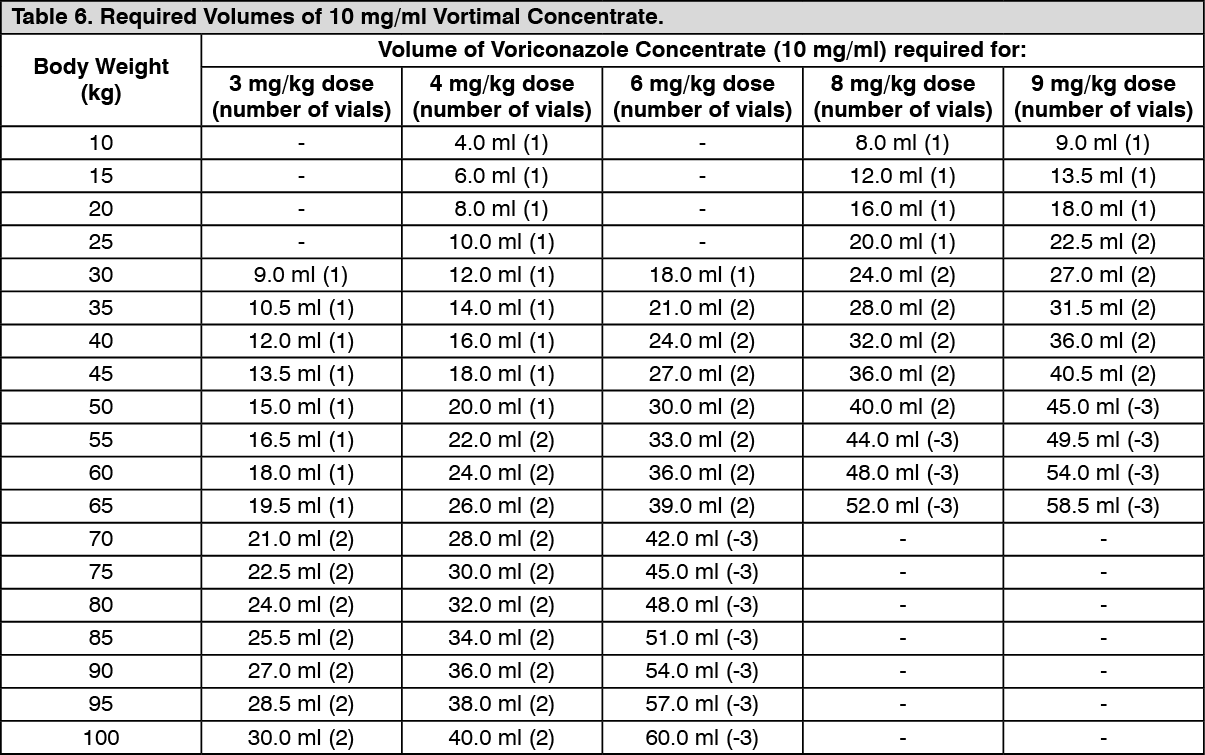 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
