


 Sign Out
Sign Out

 Click on icon to see table/diagram/image
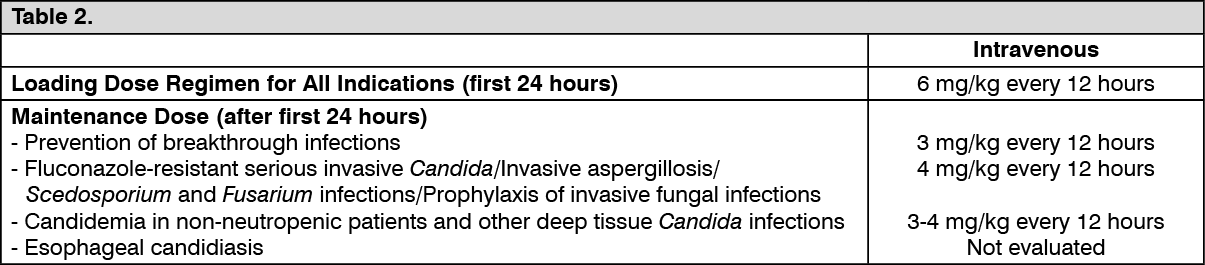
Click on icon to see table/diagram/imageDosage Adjustment: Intravenous Administration: If patient response at 3 mg/kg every 12 hours is inadequate, the intravenous maintenance dose may be increased to 4 mg/kg every 12 hours.
If patients are unable to tolerate 4 mg/kg every 12 hours, reduce the intravenous maintenance dose to a minimum of 3 mg/kg every 12 hours.
Phenytoin may be co-administered with voriconazole if the maintenance dose of voriconazole is increased to 5 mg/kg intravenously every 12 hours (see Precautions and Interactions).
Treatment duration depends upon patients' clinical and mycological response.
Elderly: No dose adjustment is necessary for elderly patients.
Patients with Renal Impairment: In patients with moderate to severe renal dysfunction (creatinine clearance <50 mL/min), accumulation of the intravenous vehicle, hydroxypropylbetadex, occurs. Oral voriconazole should be administered to these patients, unless an assessment of the risk-benefit to the patient justifies the use of intravenous voriconazole. Serum creatinine levels should be closely monitored in these patients and, if increases occur, consideration should be given to changing to oral voriconazole therapy.
Voriconazole is hemodialyzed with a clearance of 121 mL/min. A four-hour hemodialysis session does not remove a sufficient amount of voriconazole to warrant dose adjustment.
The intravenous vehicle, hydroxypropylbetadex, is hemodialyzed with a clearance of 37.5 ± 24 mL/min.
Patients with Hepatic Impairment: No dose adjustment is necessary for patients with acute hepatic injury, manifested by elevated liver function tests (ALT, AST). Continued monitoring of liver function tests for further elevations is recommended.
It is recommended that the standard loading dose regimens be used but that the maintenance dose is halved in patients with mild to moderate hepatic cirrhosis (Child-Pugh A and B) receiving voriconazole.
Voriconazole has not been studied in patients with severe chronic hepatic cirrhosis (Child-Pugh C).
Voriconazole has been associated with elevations in liver function tests and clinical signs of liver damage, such as jaundice, and must only be used in patients with severe hepatic impairment if the benefit outweighs the potential risk. Patients with severe hepatic impairment must be carefully monitored for drug toxicity. (See Table 3.)
 Click on icon to see table/diagram/image
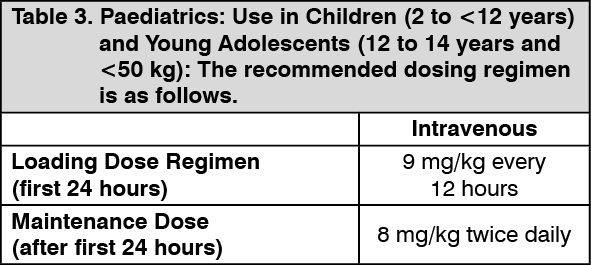
Click on icon to see table/diagram/imageIt is recommended to initiate the therapy with intravenous regimen, and oral regimen should be considered only after there is a significant clinical improvement. It should be noted that an 8 mg/kg intravenous dose will provide voriconazole exposure approximately 2-fold higher than a 9 mg/kg oral dose.
Safety and effectiveness in pediatric patients below the age of 2 years have not been established. Therefore, voriconazole is not recommended for children less than 2 years of age. Use in paediatric patients aged 2 to <12 years with hepatic or renal insufficiency has not been studied (see Pharmacology: Pharmacokinetics under Actions and Side Effects).
Use in All Other Adolescents (12 to 14 Years and ≥50 kg; 15 to 16 Years Regardless of Bodyweight): Voriconazole should be dosed as adults.
Dosage Adjustment: If patient response is inadequate, the dose may be increased by 1 mg/kg steps (or by 50 mg steps if the maximum oral dose of 350 mg was used initially). If patients are unable to tolerate treatment, reduce the dose by 1 mg/kg steps (or by 50 mg steps if the maximum oral dose of 350 mg was used initially).
Prophylaxis in Adults and Children: Prophylaxis should be initiated on the day of transplant and may be administered for up to 100 days. It may only be continued up to 180 days after transplantation in case of continuing immunosuppression or graft versus host disease (GvHD).
Dosage: The recommended dosing regimen for prophylaxis is the same as for treatment in the respective age groups. Refer to treatment Tables previously mentioned.
Duration of Prophylaxis: The safety and efficacy of voriconazole use for longer than 180 days has not been adequately studied in clinical trials.
Administration: Voriconazole requires reconstitution and dilution (see Instructions for Use under Cautions for Usage) prior to administration as an intravenous infusion.
Voriconazole powder for solution for infusion is not recommended for bolus injection.
It is recommended that voriconazole is administered at a maximum rate of 3 mg/kg per hour over 1 to 3 hours.
Route of Administration: Intravenous.