Pharmacology: Mechanism of Action: Dacomitinib is an irreversible inhibitor of the kinase activity of the human EGFR family (EGFR/HER1, HER2, and HER4) and certain EGFR activating mutations (exon 19 deletion or the exon 21 L858R substitution mutation).
In vitro dacomitinib also inhibited the activity of DDR1, EPHA6, LCK, DDR2, and MNK1 at clinically relevant concentrations.
Dacomitinib demonstrated dose-dependent inhibition of EGFR and HER2 autophosphorylation and tumor growth in mice bearing subcutaneously implanted human tumor xenografts driven by HER family targets including mutated EGFR. Dacomitinib also exhibited antitumor activity in orally-dosed mice bearing intracranial human tumor xenografts driven by EGFR amplifications.
Pharmacodynamics: Cardiac Electrophysiology: The effect of dacomitinib on the QT interval corrected for heart rate (QTc) was evaluated using time-matched electrocardiograms (ECGs) evaluating the change from baseline and corresponding pharmacokinetic data in 32 patients with advanced NSCLC. Dacomitinib had no large effect on QTc (i.e., >20 ms) at maximum dacomitinib concentrations achieved with VIZIMPRO 45 mg orally once daily.
Exposure-Response Relationships: Higher exposures, across the range of exposures with the recommended dose of 45 mg daily, correlated with an increased probability of Grade ≥3 adverse events, specifically dermatologic toxicities and diarrhea.
Clinical Studies: The efficacy of VIZIMPRO was demonstrated in a randomized, multicenter, multinational, open-label study (ARCHER 1050; [NCT01774721]). Patients were required to have unresectable, metastatic NSCLC with no prior therapy for metastatic disease or recurrent disease with a minimum of 12 months disease-free after completion of systemic therapy; an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1; EGFR exon 19 deletion or exon 21 L858R substitution mutations. EGFR mutation status was prospectively determined by local laboratory or commercially available tests (e.g., therascreen EGFR RGQ PCR and cobas EGFR Mutation Test).
Patients were randomized (1:1) to receive VIZIMPRO 45 mg orally once daily or gefitinib 250 mg orally once daily until disease progression or unacceptable toxicity. Randomization was stratified by region (Japanese versus mainland Chinese versus other East Asian versus non-East Asian), and EGFR mutation status (exon 19 deletions versus exon 21 L858R substitution mutation). The major efficacy outcome measure was progression-free survival (PFS) as determined by blinded Independent Radiologic Central (IRC) review per RECIST v1.1. Additional efficacy outcome measures were overall response rate (ORR), duration of response (DoR), and overall survival (OS).
A total of 452 patients were randomized to receive VIZIMPRO (N=227) or gefitinib (N=225). The demographic characteristics were 60% female; median age 62 years (range: 28 to 87), with 40% aged 65 years and older; and 23% White, 77% Asian, and less than 1% Black. Prognostic and tumor characteristics were ECOG performance status 0 (30%) or 1 (70%); 59% with exon 19 deletion and 41% with exon 21 L858R substitution; Stage IIIB (8%) and Stage IV (92%); 64% were never smokers; and 1% received prior adjuvant or neoadjuvant therapy.
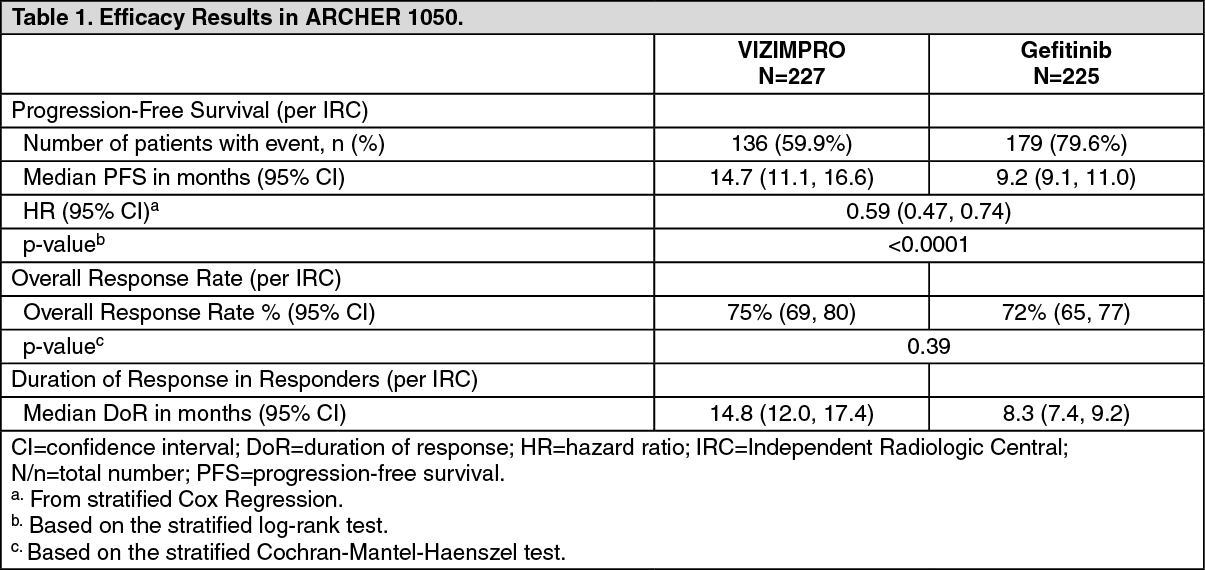
ARCHER 1050 demonstrated a statistically significant improvement in PFS as determined by the IRC. Results are summarized in Table 1 and Figures 1 and 2.
The hierarchical statistical testing order was PFS followed by ORR and then OS. No formal testing of OS was conducted since the formal comparison of ORR was not statistically significant. (See Table 1, Figures 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics: The maximum dacomitinib plasma concentration (C
max) and AUC at steady state increased proportionally over the dose range of VIZIMPRO 2 mg to 60 mg orally once daily (0.04 to 1.3 times the recommended dose) across dacomitinib studies in patients with cancer. At a dose of 45 mg orally once daily, the geometric mean [coefficient of variation (CV%)] C
max was 108 ng/mL (35%) and the AUC
0-24h was 2213 ng·h/mL (35%) at steady state in a dose-finding clinical study conducted in patients with solid tumors. Steady state was achieved within 14 days following repeated dosing and the estimated geometric mean (CV%) accumulation ratio was 5.7 (28%) based on AUC.
Absorption: The mean absolute bioavailability of dacomitinib is 80% after oral administration. The median dacomitinib time to reach maximum concentration (T
max) occurred at approximately 6.0 hours (range 2.0 to 24 hours) after a single oral dose of VIZIMPRO 45 mg in patients with cancer.
Effect of Food: Administration of VIZIMPRO with a high-fat, high-calorie meal (approximately 800 to 1000 calories with 150, 250, and 500 to 600 calories from protein, carbohydrate and fat, respectively) had no clinically meaningful effect on dacomitinib pharmacokinetics.
Distribution: The geometric mean (CV%) volume of distribution of dacomitinib (V
ss) was 1889 L (18%).
In vitro binding of dacomitinib to human plasma proteins is approximately 98% and is independent of drug concentrations from 250 ng/mL to 1000 ng/mL.
Elimination: Following a single 45 mg oral dose of VIZIMPRO in patients with cancer, the mean (CV%) plasma half-life of dacomitinib was 70 hours (21%), and the geometric mean (CV%) apparent plasma clearance of dacomitinib was 24.9 L/h (36%).
Metabolism: Hepatic metabolism is the main route of clearance of dacomitinib, with oxidation and glutathione conjugation as the major pathways. Following oral administration of a single 45 mg dose of [
14C] dacomitinib, the most abundant circulating metabolite was O-desmethyl dacomitinib, which had similar
in vitro pharmacologic activity as dacomitinib. The steady-state plasma trough concentration of O-desmethyl dacomitinib ranges from 7.4% to 19% of the parent.
In vitro studies indicated that cytochrome P450 (CYP) 2D6 was the major isozyme involved in the formation of O-desmethyl dacomitinib, while CYP3A4 contributed to the formation of other minor oxidative metabolites.
Excretion: Following a single oral 45 mg dose of [
14C] radiolabeled dacomitinib, 79% of the radioactivity was recovered in feces (20% as dacomitinib) and 3% in urine (<1% as dacomitinib).
Specific Populations: Patients with Renal Impairment: Based on population pharmacokinetic analyses, mild (60 mL/min ≤CLcr <90 mL/min; N=590) and moderate (30 mL/min ≤CLcr <60 mL/min; N=218) renal impairment did not alter dacomitinib pharmacokinetics, relative to the pharmacokinetics in patients with normal renal function (CLcr ≥90 mL/min; N=567). The pharmacokinetics of dacomitinib has not been adequately characterized in patients with severe renal impairment (CLcr <30 mL/min) (N=4) or studied in patients requiring hemodialysis.
Patients with Hepatic Impairment: In a dedicated hepatic impairment trial, following a single oral dose of 30 mg VIZIMPRO, dacomitinib exposure (AUC
inf and C
max) was unchanged in mild hepatic impairment (Child-Pugh class A; N=8) and decreased by 15% and 20%, respectively with moderate hepatic impairment (Child-Pugh class B; N=9) when compared to subjects with normal hepatic function (N=8). In a second dedicated hepatic impairment trial, following a single oral dose of 30 mg Vizimpro, dacomitinib exposure was unchanged for AUC
inf and increased by 31% for C
max in subjects with severe hepatic impairment (Child-Pugh class C; N=8), when compared to subjects with normal hepatic function (N=8). In addition, based on a population pharmacokinetic analysis using data from 1381 patients that included 158 patients with mild hepatic impairment defined by National Cancer Institute (NCI) criteria (total bilirubin ≤ Upper Limit of Normal (ULN) and Aspartate Aminotransferase AST >ULN, or total bilirubin >1.0 to 1.5 × ULN and any AST; N=158), mild hepatic impairment had no effect on the pharmacokinetics of dacomitinib. From the small number of patients in the moderate group [total bilirubin >1.5 to 3 × ULN and any AST; N=5], there is no evidence for a change in dacomitinib pharmacokinetics.
Drug Interaction Studies: Clinical Studies: Effect of Acid-Reducing Agents on Dacomitinib: Coadministration of a single 45 mg dose of VIZIMPRO with multiple doses of rabeprazole (a proton pump inhibitor) decreased dacomitinib C
max by 51% and AUC
0-96h by 39% [see Dosage Modifications for Acid-Reducing Agents under Dosage & Administration and Effect of Other Drugs on VIZIMPRO under Interactions].
Coadministration of VIZIMPRO with a local antacid (Maalox Maximum Strength, 400 mg/5 mL) did not cause clinically relevant changes dacomitinib concentrations [see Dosage Modifications for Acid-Reducing Agents under Dosage & Administration and Effect of Other Drugs on VIZIMPRO under Interactions].
The effect of H2 receptor antagonists on dacomitinib pharmacokinetics has not been studied [see Dosage Modifications for Acid-Reducing Agents under Dosage & Administration and Effect of Other Drugs on VIZIMPRO under Interactions].
Effect of Strong CYP2D6 Inhibitors on Dacomitinib: Coadministration of a single 45 mg dose of VIZIMPRO with multiple doses of paroxetine (a strong CYP2D6 inhibitor) in healthy subjects increased the total AUC
last of dacomitinib plus its active metabolite (O-desmethyl dacomitinib) in plasma by approximately 6%, which is not considered clinically relevant.
Effect of Dacomitinib on CYP2D6 Substrates: Coadministration of a single 45 mg oral dose of VIZIMPRO increased dextromethorphan (a CYP2D6 substrate) C
max by 9.7-fold and AUC
last by 9.6-fold [see Effect of VIZIMPRO on CYP2D6 Substrates under Interactions].
In Vitro Studies: Effect of Dacomitinib and O-desmethyl Dacomitinib on CYP Enzymes: Dacomitinib and its metabolite O-desmethyl dacomitinib do not inhibit CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, or CYP3A4/5. Dacomitinib does not induce CYP1A2, CYP2B6, or CYP3A4.
Effect of Dacomitinib on Uridine 5' diphospho-glucuronosyltransferase (UGT) Enzymes: Dacomitinib inhibits UGT1A1. Dacomitinib does not inhibit UGT1A4, UGT1A6, UGT1A9, UGT2B7, or UGT2B15.
Effect of Dacomitinib on Transporter Systems: Dacomitinib is a substrate for the membrane transport protein P-glycoprotein (P-gp) and Breast Cancer Resistance Protein (BCRP). Dacomitinib inhibits P-gp, BCRP, and organic cation transporter (OCT)1. Dacomitinib does not inhibit organic anion transporters (OAT)1 and OAT3, OCT2, organic anion transporting polypeptide (OATP)1B1, and OATP1B3.
Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: Carcinogenicity studies have not been performed with VIZIMPRO.
Dacomitinib was not mutagenic in a bacterial reverse mutation (Ames) assay or clastogenic in an
in vitro human lymphocyte chromosome aberration assay or clastogenic or aneugenic in an
in vivo rat bone marrow micronucleus assay.
Daily oral administration of dacomitinib at doses ≥0.5 mg/kg/day to female rats (approximately 0.14 times the exposure based on AUC at the 45 mg human dose) resulted in reversible epithelial atrophy in the cervix and vagina. Oral administration of dacomitinib at 2 mg/kg/day to male rats (approximately 0.6 times the human exposure based on AUC at the 45 mg clinical dose) resulted in reversible decreased secretion in the prostate gland.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image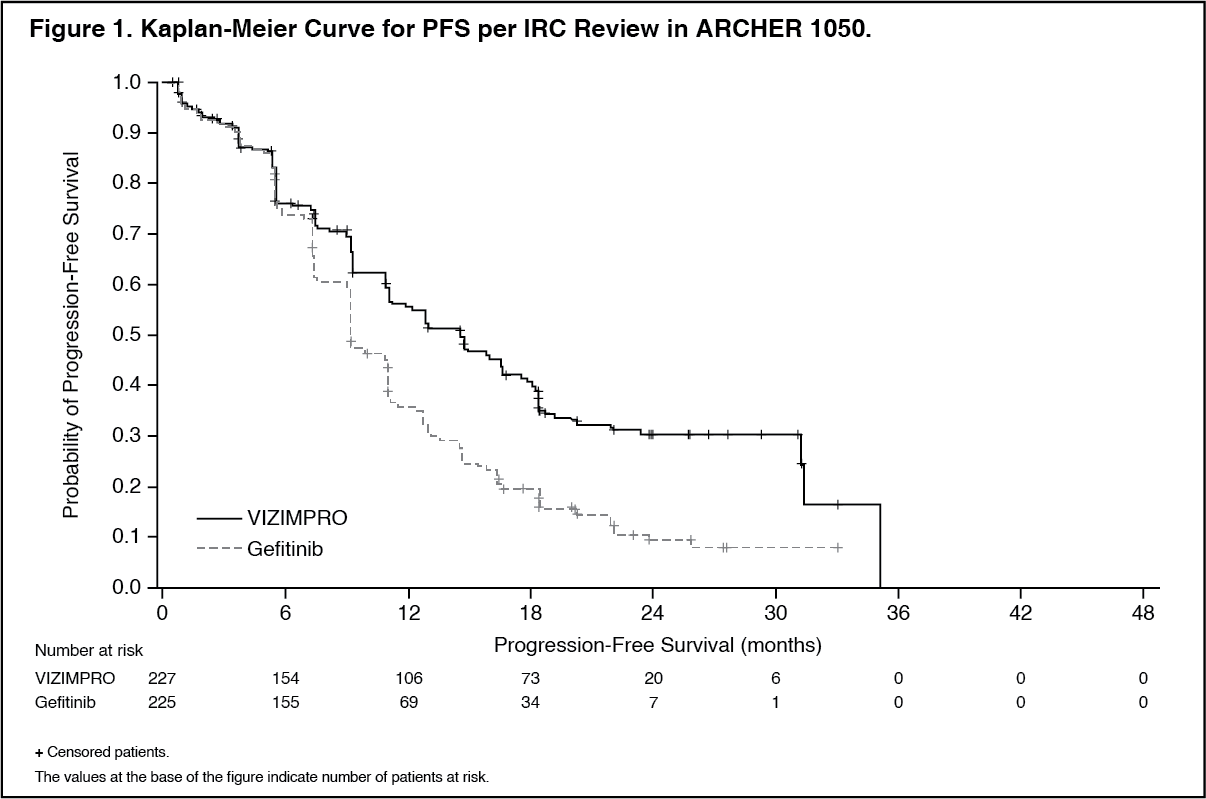 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image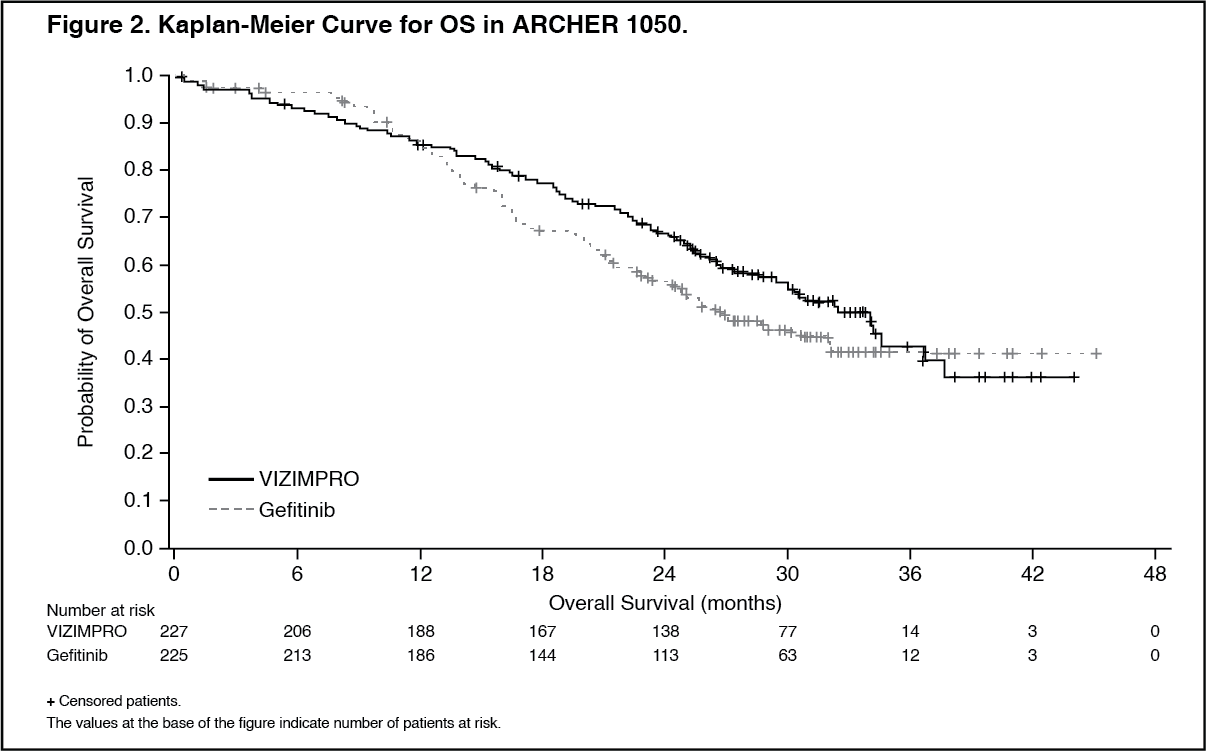 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
