The information highlighted (if any) are the most recent updates for this brand.
Perindopril arginine, amlodipine.
Viacoram 3.5 mg/2.5 mg tablets: One tablet contains 2.378 mg perindopril equivalent to 3.5 mg perindopril arginine and 3.4675 mg amlodipine besilate equivalent to 2.5 mg amlodipine.
Excipient with known effect: 31.62 mg lactose monohydrate.
Excipients/Inactive Ingredients: Lactose monohydrate, Microcrystalline cellulose (E460), Colloidal anhydrous silica (E551), Magnesium stearate (E470B).
Pharmacotherapeutic group: Agents acting on the renin-angiotensin system, ACE inhibitors and calcium channel blockers. ATC code: C09BB04.
Pharmacology: Pharmacodynamics: Mechanism of action: Viacoram combines two antihypertensive compounds with complementary mechanisms to control blood pressure in patients with essential hypertension: amlodipine belongs to the calcium antagonist class and perindopril to the angiotensin converting enzyme inhibitors class of medicines.
The combination of these substances has an additive antihypertensive effect.
Pharmacodynamic effects: Perindopril: Perindopril is an inhibitor of the enzyme that converts angiotensin I into angiotensin II (Angiotensin Converting Enzyme ACE). The converting enzyme, or kinase, is an exopeptidase that allows conversion of angiotensin I into the vasoconstrictor angiotensin II as well as causing the degradation of the vasodilator bradykinin into an inactive heptapeptide. Inhibition of ACE results in a reduction of angiotensin II in the plasma, which leads to increased plasma renin activity (by inhibition of the negative feedback of renin release) and reduced secretion of aldosterone. Since ACE inactivates bradykinin, inhibition of ACE also results in an increased activity of circulating and local kallikrein-kinin systems (and thus also activation of the prostaglandin system). It is possible that this mechanism contributes to the blood pressure-lowering action of ACE inhibitors and is partially responsible for certain of their side effects (e.g. cough).
Perindopril acts through its active metabolite, perindoprilat. The other metabolites show no inhibition of ACE activity in vitro.
Amlodipine: Amlodipine is a calcium ion influx inhibitor of the dihydropyridine group (slow channel blocker or calcium ion antagonist) and inhibits the transmembrane influx of calcium ions into cardiac and vascular smooth muscle.
The mechanism of the antihypertensive action of amlodipine is due to a direct relaxant effect on vascular smooth muscle. The precise mechanism by which amlodipine relieves angina has not been fully determined but amlodipine reduces total ischaemic burden by the following two actions: Amlodipine dilates peripheral arterioles and thus, reduces the total peripheral resistance (afterload) against which the heart works. Since the heart rate remains stable, this unloading of the heart reduces myocardial energy consumption and oxygen requirements.
The mechanism of action of amlodipine also probably involves dilatation of the main coronary arteries and coronary arterioles, both in normal and ischaemic regions. This dilatation increases myocardial oxygen delivery in patients with coronary artery spasm (Prinzmetal's or variant angina).
Clinical efficacy and safety: Perindopril/Amlodipine: In an 8-week, multicentre, randomised, double-blind, placebo-controlled, parallel group factorial study of 1581 patients with mild to moderate hypertension, perindopril 3.5 mg/amlodipine 2.5 mg clinically and statistically significantly reduced mean systolic/diastolic blood pressure (SBP/DBP) by 22.0/13.6 mmHg as compared to placebo (14.2/9.3 mmHg), perindopril 3.5 mg (16.3/9.7 mmHg) and amlodipine 2.5 mg (16.0/10.3 mmHg) (p<0.001 for all comparisons).
In a 6-month, multicentre, randomised, double-blind, active-controlled study, 1,774 patients with mild to moderate hypertension received either perindopril 3.5 mg/amlodipine 2.5 mg, uptitrated to 7 mg/5 mg, and 14 mg/10 mg, then to 14 mg/10 mg combined with indapamide 1.5 mg, or a valsartan-amlodipine strategy (valsartan 80 mg uptitrated to 160 mg and to valsartan/amlodipine 160 mg/5 mg, then to valsartan/amlodipine 160 mg/10 mg).
At 3 months, Viacoram strategy showed clinically and statistically significant mean decrease in SBP/DBP (25.9/16.9 mmHg) as compared to valsartan-amlodipine strategy (23.6/15.5 mmHg) (p<0.001 for all comparisons).
Blood pressure was controlled in 56.4% of patients treated with Viacoram strategy versus 49.0% with valsartan-amlodipine strategy (p=0.002), and the rate of responders was 87.4% versus 81.6%, respectively (p<0.001).
The superiority of Viacoram strategy over the valsartan-amlodipine strategy on blood pressure decrease and responder rates was observed from 1 month and maintained at each visit up to 6 months.
These results were confirmed in a 24-hour automated blood pressure monitoring (ABPM) performed in a subset of 1029 patients. At 3 months and 6 months, the decrease of the mean SBP and DBP over 24 hours was greater with Viacoram (15.5/9.4 mmHg and 17/10.4 mmHg, respectively) as compared to valsartan-amlodipine strategy (12.7/8.0 mmHg and 14.7/9.2 mmHg, respectively) (p≤0.001).
In the 8-month open-label follow-up on 1,554 patients, the safety profile of Viacoram was in line with the safety profiles of perindopril and amlodipine.
In a 9-month, multicentre, randomised, double-blind, active-controlled study, 3,270 patients with mild to severe hypertension received either perindopril/amlodipine 3.5 mg/2.5 mg, uptitrated to 7 mg/5 mg, 14 mg/5 mg then 14 mg/10 mg, or an irbesartan-hydrochlorothiazide strategy (irbesartan 150 mg, then irbesartan/hydrochlorothiazide 150 mg/12.5 mg, 300 mg/12.5 mg and 300 mg/25 mg).
The proportion of patients with controlled blood pressure statistically significantly increased with each of the perindopril/amlodipine treatment dose over each evaluation period (p<0.001 until 3 months, and p≤0.003 until 6 months).
After 6 months of treatment, the mean decrease in blood pressure was similar in the perindopril/amlodipine group (22.0/10.1 mmHg) and the irbesartan-hydrochlorothiazide group (22.5/9.6 mmHg) for both SBP (p=0.116) and DBP (p=0.050).
The most common adverse reactions in clinical trials were dizziness, cough and oedema (see Adverse Reactions).
The adverse reactions reported in clinical trials were in agreement with those anticipated from the safety profiles of the components perindopril and amlodipine.
Dual blockade of the renin-angiotensin-aldosterone system (RAAS) clinical trial data: Two large, randomised, controlled trials (ONTARGET (ONgoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial) and VA NEPHRON-D (The Veterans Affairs Nephropathy in Diabetes)) have examined the use of combination of an ACE-inhibitor with an angiotensin II receptor blocker.
ONTARGET was a study conducted in patients with a history of cardiovascular or cerebrovascular disease, or type 2 diabetes mellitus accompanied by evidence of end-organ damage. VA NEPHRON-D was a study in patients with type 2 diabetes mellitus and diabetic nephropathy.
These studies have shown no significant beneficial effect on renal and/or cardiovascular outcomes and mortality, while an increased risk of hyperkalaemia, acute kidney injury and/or hypotension as compared to monotherapy was observed.
Given their similar pharmacodynamic properties, these results are also relevant for other ACE-inhibitors and angiotensin II receptor blockers.
ACE-inhibitors and angiotensin II receptor blockers should therefore not be used concomitantly in patients with diabetic nephropathy.
ALTITUDE (Aliskiren Trial in Type 2 Diabetes Using Cardiovascular and Renal Disease Endpoints) was a study designed to test the benefit of adding aliskiren to a standard therapy of an ACE-inhibitor or an angiotensin II receptor blocker in patients with type 2 diabetes mellitus and chronic kidney disease, cardiovascular disease, or both. The study was terminated early because of an increased risk of adverse outcomes. Cardiovascular death and stroke were both numerically more frequent in the aliskiren group than in the placebo group and adverse events and serious adverse events of interest (hyperkalaemia, hypotension and renal dysfunction) were more frequently reported in the aliskiren group than in the placebo group.
Pharmacokinetics: The rate and extent of absorption of perindopril and amlodipine from Viacoram are not significantly different, respectively, from the rate and extent of absorption of perindopril and amlodipine from individual tablet formulations.
Perindopril: Absorption: After oral administration, the absorption of perindopril is rapid and the peak concentration is achieved within 1 hour. The plasma half-life of perindopril is equal to 1 hour.
Perindopril is a prodrug. Twenty-seven percent of the administered perindopril dose reaches the bloodstream as the active metabolite perindoprilat. In addition to active perindoprilat, perindopril yields five metabolites, all inactive. The peak plasma concentration of perindoprilat is achieved within 3 to 4 hours.
As ingestion of food decreases conversion to perindoprilat, hence bioavailability, perindopril arginine should be administered orally in a single daily dose in the morning before a meal.
It has been demonstrated a linear relationship between the dose of perindopril and its plasma exposure.
Distribution: The volume of distribution is approximately 0.2 l/kg for unbound perindoprilat. Protein binding of perindoprilat to plasma proteins is 20%, principally to angiotensin converting enzyme, but is concentration-dependent.
Elimination: Perindoprilat is eliminated in the urine and the terminal half-life of the unbound fraction is approximately 17 hours, resulting in steady-state within 4 days.
Amlodipine: Absorption, distribution, plasma protein binding: After oral administration of therapeutic doses, amlodipine is well absorbed with peak blood levels between 6-12 hours post dose. Absolute bioavailability has been estimated to be between 64 and 80%. The volume of distribution is approximately 21 l/kg. In vitro studies have shown that approximately 97.5% of circulating amlodipine is bound to plasma proteins.
The bioavailability of amlodipine is not affected by food intake.
Biotransformation, elimination: The terminal plasma elimination half-life is about 35-50 hours and is consistent with once daily dosing. Amlodipine is extensively metabolised by the liver to inactive metabolites with 10% of the parent compound and 60% of metabolites excreted in the urine.
Special populations: Paediatric population (age below 18 years): No pharmacokinetic data are available in the paediatric population.
Older people: The time to reach peak plasma concentrations of amlodipine is similar in elderly and younger subjects. In elderly patients, amlodipine clearance tends to be decreased with resulting increases in AUC and elimination half-life in elderly patients.
Initiation and increase of the dosage should take place with care in older people depending on renal function.
Elimination of perindoprilat is decreased in the elderly. Renal function should be monitored before increase of the dosage. Therefore, the usual medical follow-up will include monitoring of creatinine and potassium (see Dosage & Administration and Precautions).
Renal impairment: In patients with moderate renal impairment (Creatinine clearance between 30 ml/min to 60 ml/min), the initial recommended dose of Viacoram is 3.5 mg/2.5 mg every other day (see Dosage & Administration).
The pharmacokinetics of amlodipine are not significantly influenced by renal impairment. Amlodipine is not dialyzable.
Elimination of perindoprilat is decreased in patients with heart or renal failure.
Therefore, the usual medical follow-up will include monitoring of creatinine and potassium (see Dosage & Administration and Precautions).
Hepatic impairment: Caution should be exercised in patients with liver disease (see Dosage & Administration and Precautions).
Very limited clinical data are available regarding amlodipine administration in patients with hepatic impairment. Patients with hepatic insufficiency have decreased clearance of amlodipine resulting in a longer half-life and an increase in AUC of approximately 40-60%.
Dialysis clearance of perindoprilat is equal to 70 ml/min. Perindopril kinetics are modified in patients with cirrhosis: hepatic clearance of the parent molecule is reduced by half. However, the quantity of perindoprilat formed is not reduced and therefore no dosage adjustment is required (see Dosage & Administration and Precautions).
Toxicology: Preclinical safety data: Perindopril/Amlodipine: A preclinical safety study has demonstrated that the combination of perindopril and amlodipine was well tolerated in rats. The findings from the 13-week oral toxicity study in rats were consistent with those of perindopril and amlodipine when both active substances are administered alone. There were no new toxicities or increased severity of the toxicities which were associated with either component.
Perindopril: In the chronic oral toxicity studies (rats and monkeys), the target organ is the kidney, with reversible damage.
No mutagenicity has been observed in in vitro or in vivo studies.
Reproduction toxicology studies (rats, mice, rabbits and monkeys) showed no sign of embryotoxicity or teratogenicity. However, angiotensin converting enzyme inhibitors, as a class, have been shown to induce adverse effects on late foetal development, resulting in foetal death and congenital effects in rodents and rabbits: renal lesions and an increase in peri- and postnatal mortality have been observed.
No carcinogenicity has been observed in long term studies in rats and mice. Fertility was not impaired either in male or in female rats.
Amlodipine: Reproductive toxicology: Reproductive studies in rats and mice have shown delayed date of delivery, prolonged duration of labour and decreased pup survival at dosages approximately 50 times greater than the maximum recommended dosage for humans based on mg/kg.
Impairment of fertility: There was no effect on the fertility of rats treated with amlodipine (males for 64 days and females 14 days prior to mating) at doses up to 10 mg/kg/day (8 times* the maximum recommended human dose of 10 mg on a mg/m2 basis). In another rat study in which male rats were treated with amlodipine besilate for 30 days at a dose comparable with the human dose based on mg/kg, decreased plasma follicle-stimulating hormone and testosterone were found as well as decreases in sperm density and in the number of mature spermatids and Sertoli cells.
Carcinogenesis, mutagenesis: Rats and mice treated with amlodipine in the diet for two years, at concentrations calculated to provide daily dosage levels of 0.5, 1.25, and 2.5 mg/kg/day showed no evidence of carcinogenicity. The highest dose (for mice, similar to, and for rats twice* the maximum recommended clinical dose of 10 mg on a mg/m2 basis) was close to the maximum tolerated dose for mice but not for rats.
Mutagenicity studies revealed no drug related effects at either the gene or chromosome levels.
* Based on patient weight of 50 kg.
Viacoram is indicated for the treatment of mild to moderate essential hypertension in patients for whom combination therapy is appropriate.
Viacoram 3.5 mg/2.5 mg is indicated for initial therapy in patients with mild to moderate essential hypertension.
Viacoram is not indicated for switching therapy from the individual drugs currently on the market (perindopril as erbumine or arginine salt, amlodipine).
Posology: Oral use.
Viacoram 3.5 mg/2.5 mg is intended for initial therapy in patients with mild to moderate essential hypertension.
The recommended starting dose of Viacoram is 3.5 mg/2.5 mg once daily.
After at least four weeks of treatment, the dose may be increased to 7 mg/5 mg once daily in patients whose blood pressure is not adequately controlled with Viacoram 3.5 mg/2.5 mg.
Special populations: Patients with renal impairment (see Contraindications, Precautions and Pharmacology: Pharmacokinetics under Actions): Viacoram is contraindicated in patients with severe renal impairment (Creatinine clearance below 30 ml/min) (see Contraindications).
In patients with moderate renal impairment (Creatinine clearance between 30 ml/min to 60 ml/min), the initial recommended dose of Viacoram is 3.5 mg/2.5 mg every other day. In patients whose blood pressure is not adequately controlled, the dose of Viacoram 3.5 mg/2.5 mg may be taken once daily. If necessary, the dose may be increased in patients insufficiently controlled. The usual medical follow-up includes monitoring of creatinine and potassium (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Patients with hepatic impairment (see Precautions and Pharmacology: Pharmacokinetics under Actions): Caution should be exercised when prescribing Viacoram to patients with severe hepatic impairment.
Older people (see Precautions and Pharmacology: Pharmacokinetics under Actions): The efficacy and safety of Viacoram have been established in older people. Caution should be exercised at initiation depending on renal function.
After initiation of the treatment, renal function should be monitored before increase of the dosage, particularly in patients aged 75 years and above. The usual medical follow-up should include monitoring of creatinine and potassium.
Paediatric population: The safety and efficacy of Viacoram in children aged below 18 years have not been established. No data are available.
Method of administration: The tablet of Viacoram should be taken as a single dose, preferably in the morning and before a meal.
There is no experience of overdose with Viacoram.
For amlodipine, experience with intentional overdose in humans is limited.
Symptoms: Available data suggest that gross overdosage could result in excessive peripheral vasodilatation and possibly reflex tachycardia. Marked and probably prolonged systemic hypotension up to and including shock with fatal outcome have been reported.
Non-cardiogenic pulmonary oedema has rarely been reported as a consequence of amlodipine overdose that may manifest with a delayed onset (24-48 hours post-ingestion) and require ventilatory support. Early resuscitative measures (including fluid overload) to maintain perfusion and cardiac output may be precipitating factors.
Treatment: Clinically significant hypotension due to amlodipine overdosage calls for active cardiovascular support including frequent monitoring of cardiac and respiratory function, elevation of extremities and attention to circulating fluid volume and urine output.
A vasoconstrictor may be helpful in restoring vascular tone and blood pressure, provided that there is no contraindication to its use. Intravenous calcium gluconate may be beneficial in reversing the effects of calcium channel blockade.
Gastric lavage may be worthwhile in some cases. In healthy volunteers, the use of charcoal up to 2 hours after administration of amlodipine 10 mg has been shown to reduce the absorption rate of amlodipine.
Since amlodipine is highly protein-bound, dialysis is not likely to be of benefit.
For perindopril, limited data are available for overdosage in humans. Symptoms associated with the overdosage of ACE inhibitors may include hypotension, circulatory shock, electrolyte disturbances, renal failure, hyperventilation, tachycardia, palpitations, bradycardia, dizziness, anxiety, and cough.
The recommended treatment of overdosage is intravenous infusion of normal saline solution. If hypotension occurs, the patient should be placed in the shock position. If available, treatment with angiotensin II infusion and/or intravenous catecholamines may also be considered. Perindopril can be removed from the systemic circulation by haemodialysis (see Precautions). Pacemaker therapy is indicated for treatment-resistant bradycardia. Vital signs, serum electrolytes and creatinine concentrations should be monitored continuously.
Hypersensitivity to the active substances, to ACE inhibitors, to dihydropyridines derivatives, or to any of the excipients listed in Description.
Severe renal impairment (see Dosage & Administration and Precautions).
History of angioedema associated with previous ACE inhibitor therapy.
Hereditary or idiopathic angioedema.
Second and third trimesters of pregnancy (see Precautions and Use in Pregnancy & Lactation).
Severe hypotension.
Shock, including cardiogenic shock.
Obstruction of the outflow-tract of the left ventricle (e.g. high grade aortic stenosis).
Haemodynamically unstable heart failure after acute myocardial infarction.
Concomitant use of Viacoram with aliskiren in patients with diabetes mellitus or renal impairment (GFR <60 ml/min/1.73 m2) (see Interactions and Pharmacology: Pharmacodynamics under Actions).
Extracorporeal treatments leading to contact of blood with negatively charged surfaces (see Interactions).
Significant bilateral renal artery stenosis or renal artery stenosis in a single functioning kidney (see Precautions).
Concomitant use with sacubitril/valsartan therapy, Perindopril must not be initiated earlier than 36 hours after the last dose of sacubitril/valsartan (see Precautions and Interactions).
The use of ACE inhibitors is not recommended during the first trimester of pregnancy (see Precautions). The use of ACE inhibitors is contraindicated during the second and third trimester of pregnancy (see Contraindications and Precautions).
Special warnings: Hypersensitivity/Angioedema: Angioedema of the face, extremities, lips, mucous membranes, tongue, glottis and/or larynx has been reported rarely in patients treated with ACE inhibitors, including perindopril (see Adverse Reactions). This may occur at any time during therapy. In such cases, Viacoram should promptly be discontinued and appropriate monitoring should be initiated and continued until complete resolution of symptoms has occurred. In those instances where swelling was confined to the face and lips the condition generally resolved without treatment, although antihistamines have been useful in relieving symptoms.
Angioedema associated with laryngeal oedema may be fatal. Where there is involvement of the tongue, glottis or larynx, likely to cause airway obstruction, emergency therapy should be administered promptly. This may include the administration of adrenaline and/or the maintenance of a patent airway. The patient should be under close medical supervision until complete and sustained resolution of symptoms has occurred.
Patients with a history of angioedema unrelated to ACE inhibitor therapy may be at increased risk of angioedema while receiving Viacoram (see Contraindications).
Intestinal angioedema has been reported rarely in patients treated with ACE inhibitors. These patients presented with abdominal pain (with or without nausea or vomiting); in some cases there was no prior facial angioedema and C-1 esterase levels were normal. The angioedema was diagnosed by procedures including abdominal CT scan, or ultrasound or at surgery and symptoms resolved after stopping the ACE inhibitor. Intestinal angioedema should be included in the differential diagnosis of patients on ACE inhibitors presenting with abdominal pain (see Adverse Reactions).
The combination of perindopril with sacubitril/valsartan is contraindicated due to the increased risk of angioedema (see Contraindications). Sacubitril/valsartan must not be initiated until 36 hours after taking the last dose of perindopril therapy. If treatment with sacubitril/valsartan is stopped, perindopril therapy must not be initiated until 36 hours after the last dose of sacubitril/valsartan (see Contraindications and Interactions).
Concomitant use of ACE inhibitors with NEP inhibitors (e.g. racecadotril), mTOR inhibitors (e.g. sirolimus, everolimus, temsirolimus) and gliptins (e.g. linagliptin, saxagliptin, sitagliptin, vildagliptin) may lead to an increased risk of angioedema (e.g. swelling of the airways or tongue, with or without respiratory impairment) (see Interactions). Caution should be used when starting racecadotril, mTOR inhibitors (e.g. sirolimus, everolimus, temsirolimus) and gliptins (e.g. linagliptin, saxagliptin, sitagliptin, vildagliptin) in a patient already taking an ACE inhibitor.
Hence, a careful benefit-risk assessment is needed before initiating treatment with NEP inhibitors (e.g. racecadotril) in patients on perindopril.
Anaphylactoid reactions during low-density lipoproteins (LDL) apheresis: Rarely, patients receiving ACE inhibitors during low-density lipoprotein (LDL) apheresis with dextran sulphate have experienced life-threatening anaphylactoid reactions. These reactions were avoided by temporarily withholding ACE inhibitor therapy prior to each apheresis.
Anaphylactoid reactions during desensitisation: Patients receiving ACE inhibitors during desensitisation treatment (e.g. hymenoptera venom) have experienced anaphylactoid reactions. In the same patients, these reactions have been avoided when the ACE inhibitors were temporarily withheld, but they reappeared upon inadvertent rechallenge.
Haemodialysis patients: Anaphylactoid reactions have been reported in patients dialysed with high flux membranes and treated concomitantly with an ACE inhibitor. In these patients, consideration should be given to using a different type of dialysis membrane or different class of antihypertensive agent.
Neutropenia/Agranulocytosis/Thrombocytopenia/Anaemia: Neutropenia/agranulocytosis, thrombocytopenia and anaemia have been reported in patients receiving ACE inhibitors. In patients with normal renal function and no other complicating factors, neutropenia occurs rarely. Viacoram should be used with extreme caution in patients with collagen vascular disease, immunosuppressant therapy, treatment with allopurinol or procainamide, or a combination of these complicating factors, especially if there is pre-existing impaired renal function. Some of these patients developed serious infections, which in a few instances did not respond to intensive antibiotic therapy. If Viacoram is used in such patients, periodic monitoring of white blood cell counts is advised and patients should be instructed to report any sign of infection (e.g. sore throat, fever).
Dual blockade of the renin-angiotensin-aldosterone system (RAAS): There is evidence that the concomitant use of ACE-inhibitors, angiotensin II receptor blockers or aliskiren increases the risk of hypotension, hyperkalaemia and decreased renal function (including acute renal failure). Dual blockade of RAAS through the combined use of ACE-inhibitors, angiotensin II receptor blockers or aliskiren is therefore not recommended (see Interactions and Pharmacology: Pharmacodynamics under Actions).
If dual blockade therapy is considered absolutely necessary, this should only occur under specialist supervision and subject to frequent close monitoring of renal function, electrolytes and blood pressure.
ACE-inhibitors and angiotensin II receptor blockers should not be used concomitantly in patients with diabetic nephropathy.
Primary aldosteronism: Patients with primary hyperaldosteronism generally will not respond to anti-hypertensive drugs acting through inhibition of the renin-angiotensin system. Therefore, the use of this product is not recommended.
Kidney transplantation: Since there is no experience regarding the administration of Viacoram in patients with a recent kidney transplantation, treatment with Viacoram is therefore not recommended.
Renovascular hypertension: There is an increased risk of hypotension and renal insufficiency when patient with bilateral renal artery stenosis or stenosis of the artery to a single functioning kidney are treated with ACE inhibitors (see Contraindications). Treatment with diuretics may be a contributory factor. Loss of renal function may occur with only minor changes in serum creatinine even in patients with unilateral renal artery stenosis.
Precautions for use: Hypertensive crisis: The safety and efficacy of amlodipine in hypertensive crisis has not been established.
Use in patients with cardiac failure: Patients with heart failure should be treated with caution.
Viacoram should be used with caution in patients with congestive heart failure, as amlodipine may increase the risk of future cardiovascular events and mortality.
Hypotension: ACE inhibitors may cause a fall in blood pressure. Symptomatic hypotension is seen rarely in uncomplicated hypertensive patients and is more likely to occur in patients who have been volume-depleted e.g. by diuretic therapy, dietary salt restriction, dialysis, diarrhoea or vomiting, or who have severe renin-dependent hypertension (see Interactions and Adverse Reactions). In patients at high risk of symptomatic hypotension, blood pressure, renal function and serum potassium should be monitored closely during treatment with Viacoram.
Similar considerations apply to patients with ischaemic heart or cerebrovascular disease in whom an excessive fall in blood pressure could result in a myocardial infarction or cerebrovascular accident.
If hypotension occurs, the patient should be placed in the supine position and, if necessary, should receive an intravenous infusion of sodium chloride 9 mg/ml (0.9%) solution. A transient hypotensive response is not a contraindication to further doses, which can be given usually without difficulty once the blood pressure has increased after volume expansion.
Aortic and mitral valve stenosis/hypertrophic cardiomyopathy: ACE inhibitors should be given with caution to patients with mitral valve stenosis and obstruction in the outflow of the left ventricle such as aortic stenosis or hypertrophic cardiomyopathy.
Race: ACE inhibitors cause a higher rate of angioedema in black patients than in non-black patients.
ACE inhibitors may be less effective in lowering blood pressure in black people than in non-blacks, possibly because of a higher prevalence of low-renin states in the black hypertensive population.
Cough: Cough has been reported with the use of Viacoram. Characteristically, the cough is non-productive, persistent and resolves after discontinuation of therapy. ACE inhibitor-induced cough should be considered as part of the differential diagnosis of cough.
Surgery/Anaesthesia: In patients undergoing major surgery or during anaesthesia with agents that produce hypotension, perindopril may block angiotensin II formation secondary to compensatory renin release. Viacoram should be discontinued one day prior to the surgery. If hypotension occurs and is considered to be due to this mechanism, it can be corrected by volume expansion.
Hyperkalaemia: Elevations in serum potassium have been observed in some patients treated with ACE inhibitors, including perindopril. Risk factors for the development of hyperkalaemia include those with renal insufficiency, worsening of renal function, age (>70 years), diabetes mellitus, intercurrent events, in particular dehydration, acute cardiac decompensation, metabolic acidosis, and concomitant use of potassium-sparing diuretics (e.g. spironolactone, eplerenone, triamterene, or amiloride, alone or in combination), potassium supplements or potassium-containing salt substitutes; or those patients taking other drugs associated with increases in serum potassium (e.g. heparin, other ACE inhibitors, angiotensin II antagonists, acetylsalicylic acid ≥3 g/day, COX-2 inhibitors and non-selective NSAIDs, immunosuppressant agents such as ciclosporin or tacrolimus, trimethoprim and co-trimoxazole also known as trimethoprim/sulfamethoxazole). The use of potassium supplements, potassium-sparing diuretics, or potassium-containing salt substitutes particularly in patients with impaired renal function may lead to a significant increase in serum potassium. Hyperkalaemia can cause serious, sometimes fatal arrhythmias. If concomitant use of Viacoram and any of the previously mentioned agents is deemed appropriate, they should be used with caution and with frequent monitoring of serum potassium (see Interactions).
Diabetic patients: In diabetic patients treated with oral antidiabetic agents or insulin, glycaemic control should be closely monitored during the first month of treatment with Viacoram (see Interactions).
Potassium-sparing drugs, potassium supplements or potassium-containing salt substitutes: The combination of Viacoram and potassium-sparing drugs, potassium supplements or potassium-containing salt substitutes is not recommended (see Interactions).
Excipients: This medicine contains lactose. Patients with rare hereditary problems of galactose intolerance, the total lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Effects on ability to drive and use machines: No studies on the effects of Viacoram on the ability to drive and use machines have been performed.
Perindopril and amlodipine can have minor or moderate influence on the ability to drive and use machines. If patients suffer from dizziness, headache, fatigue, weariness or nausea, the ability to react may be impaired.
Caution is recommended with Viacoram especially at the start of treatment.
Use in patients with renal impairment: Viacoram is contraindicated in patients with severe renal impairment (Creatinine clearance below 30 ml/min) (see Contraindications).
In patients with moderate renal impairment (Creatinine clearance between 30 ml/min to 60 ml/min), the initial recommended dose of Viacoram is 3.5 mg/2.5 mg every other day (see Dosage & Administration). The usual medical follow-up in such patients should include monitoring of potassium levels and creatinine (see Dosage & Administration and Pharmacology: Pharmacokinetics under Actions).
In some patients with bilateral renal artery stenosis or stenosis of the artery to a solitary kidney, who have been treated with ACE inhibitors, increases in blood urea and serum creatinine, usually reversible upon discontinuation of therapy, have been seen. This is especially likely in patients with renal insufficiency. If renovascular hypertension is also present, there is an increased risk of severe hypotension and renal insufficiency. Some hypertensive patients with no apparent pre-existing renal vascular disease have developed increases in blood urea and serum creatinine, usually minor and transient, especially when perindopril has been given concomitantly with a diuretic. This is more likely to occur in patients with pre-existing renal impairment.
Amlodipine may be used in patients with renal failure at normal doses. Changes in amlodipine plasma concentrations are not correlated with degree of renal impairment. Amlodipine is not dialysable.
Use in patients with impaired hepatic function: Rarely, ACE inhibitors have been associated with a syndrome that starts with cholestatic jaundice and progresses to fulminant hepatic necrosis and (sometimes) death. The mechanism of this syndrome is not understood. Patients receiving Viacoram who develop jaundice or marked elevations of hepatic enzymes should discontinue Viacoram and receive appropriate medical follow-up (see Adverse Reactions).
The half-life of amlodipine is prolonged and AUC values are higher in patients with impaired liver function.
Use in Pregnancy: Viacoram should not be initiated during pregnancy. Unless continued Viacoram is considered essential, patients planning pregnancy should be changed to alternative antihypertensive treatments which have an established safety profile for use in pregnancy. When pregnancy is diagnosed, treatment with Viacoram should be stopped immediately, and, if appropriate, alternative therapy should be started. Increased risk of birth defects, foetal and neonatal morbidity and death when ACE inhibitors used throughout pregnancy (see Contraindications and Use in Pregnancy & Lactation).
Use in the Elderly: Initiation and increase of the dosage should take place with care in older people, depending on renal function.
Renal function should be monitored before increase of the dosage. Therefore, the medical follow-up should include monitoring of potassium and creatinine (see Dosage & Administration and Pharmacology: Pharmacokinetics under Actions).
Given the effects of the individual components in this combination product on pregnancy and lactation: Viacoram is not recommended during the first trimester of pregnancy. Viacoram is contraindicated during the second and third trimesters of pregnancy.
Viacoram is not recommended during lactation. A decision should therefore be made whether to discontinue nursing or to discontinue Viacoram taking account the importance of this therapy for the mother.
Pregnancy: Linked to perindopril: Epidemiological evidence regarding the risk of teratogenicity following exposure to ACE inhibitors during the first trimester of pregnancy has not been conclusive; however, a small increase in risk cannot be excluded. Unless continued ACE inhibitor therapy is considered essential, patients planning pregnancy should be changed to alternative antihypertensive treatments which have an established safety profile for use in pregnancy. When pregnancy is diagnosed, treatment with ACE inhibitors should be stopped immediately, and, if appropriate, alternative therapy should be started. Increased risk of birth defects, foetal and neonatal morbidity and death when used throughout pregnancy.
Exposure to ACE inhibitor therapy during the second and third trimesters is known to induce human foetotoxicity (decreased renal function, oligohydramnios, skull ossification retardation) and neonatal toxicity (renal failure, hypotension, hyperkalaemia) (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Should exposure to ACE inhibitor have occurred from the second trimester of pregnancy, ultrasound check of renal function and skull is recommended.
Infants whose mothers have taken ACE inhibitors should be closely observed for hypotension (see Contraindications and Precautions).
Linked to amlodipine: The safety of amlodipine in human pregnancy has not been established.
In animal studies, reproductive toxicity was observed at high doses (see Pharmacology: Toxicology: Preclinical safety data under Actions). Use in pregnancy is only recommended when there is no safer alternative and when the disease itself carries greater risk for the mother and foetus.
Breast-feeding: Linked to perindopril: Because no information is available regarding the use of perindopril during breast-feeding, perindopril is not recommended and alternative treatments with better established safety profiles during breast-feeding are preferable, especially while nursing a newborn or preterm infant.
Linked to amlodipine: Amlodipine is excreted in human milk. The proportion of the maternal dose received by the infant has been estimated with an interquartile range of 3 - 7%, with a maximum of 15%. The effect of amlodipine on infants is unknown. A decision on whether to continue/discontinue breast-feeding or to continue/discontinue therapy with amlodipine should be made taking into account the benefit of breast-feeding to the child and the benefit of amlodipine therapy to the mother.
Fertility: Linked to perindopril: There was no effect on reproductive performance or fertility.
Linked to amlodipine: Reversible biochemical changes in the head of spermatozoa have been reported in some patients treated by calcium channel blockers. Clinical data are insufficient regarding the potential effect of amlodipine on fertility. In one rat study, adverse effects were found on male fertility (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Summary of the safety profile: The safety profile of Viacoram has been evaluated on a 6-month controlled study involving 1,771 patients, 887 of whom received Viacoram, a 6-week controlled study involving 837 patients, 279 of whom received Viacoram, and an 8-week placebo-controlled study involving 1581 patients, 249 of whom received Viacoram.
In these clinical studies, no significant new adverse reactions were observed with the combination compared to the known effects of the individual monocomponents.
The following adverse reactions were found to be the most frequently reported during clinical trials: dizziness, cough and oedema.
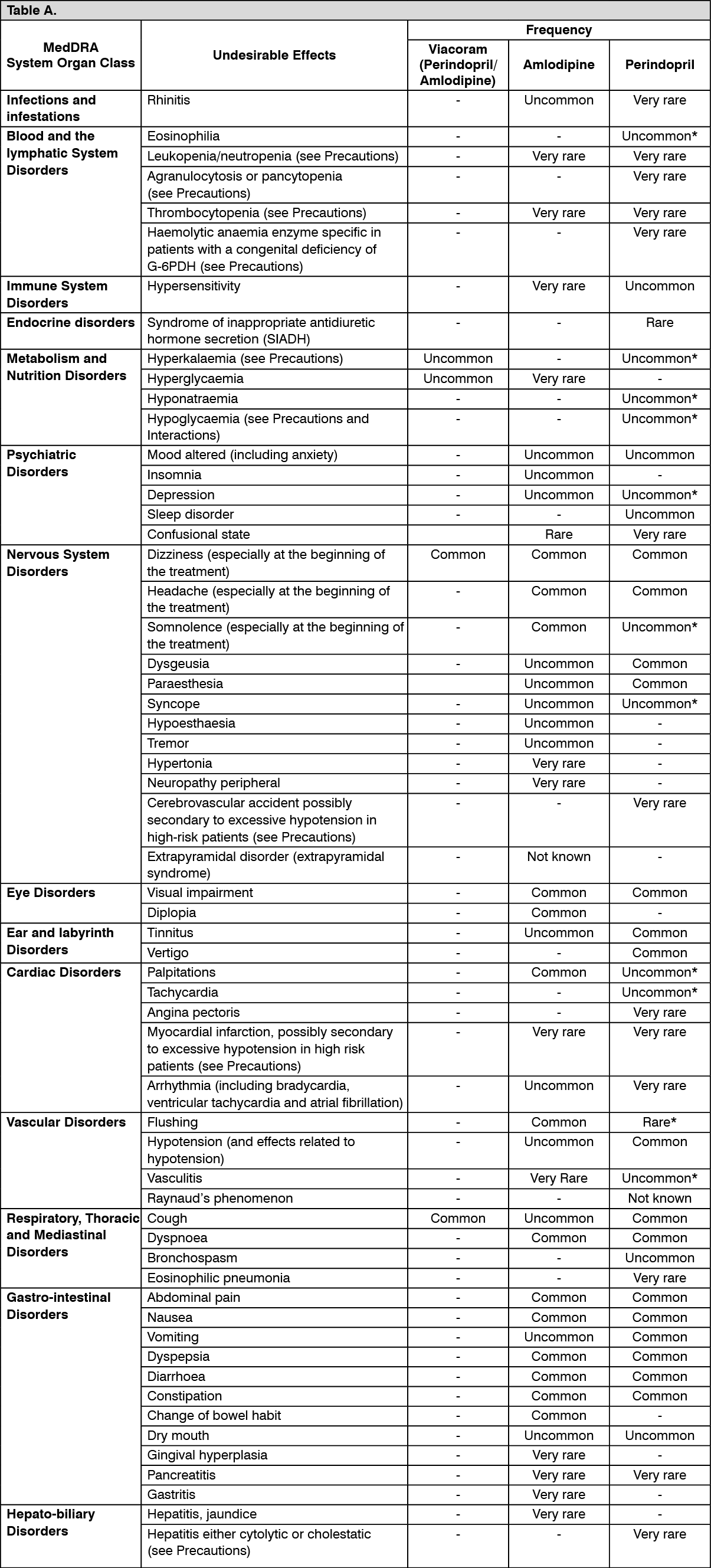
The adverse drug reactions previously reported during clinical trials and/or post-marketing experience with one of the individual components of Viacoram (perindopril and amlodipine) have been listed in the following table since they may occur with the fixed-dose combination.
Tabulated list of adverse reactions: The following undesirable effects have been observed during treatment with Viacoram, perindopril or amlodipine given separately and ranked under the MedDRA classification by body system and under the following frequency: Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1000 to <1/100); rare (≥1/10000 to <1/1000); very rare (<1/10000); not known (cannot be estimated from the available data). (
See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Additional information on the combination perindopril/amlodipine:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Additional information on the combination perindopril/amlodipine: A randomised, double-blind, placebo-controlled study over 8 weeks demonstrated that peripheral oedema, a recognised side effect of amlodipine, was observed at a lower incidence in patients who received the perindopril 3.5 mg/amlodipine 2.5 mg combination than in those who received amlodipine 5 mg alone (1.6% and 4.9% respectively).
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system.
Dual blockade of the renin-angiotensin-aldosterone system (RAAS): Clinical trial data has shown that dual blockade of the renin-angiotensin-aldosterone-system (RAAS) through the combined use of ACE-inhibitors, angiotensin II receptor blockers or aliskiren is associated with a higher frequency of adverse events such as hypotension, hyperkalaemia and decreased renal function (including acute renal failure) compared to the use of a single RAAS-acting agent (see Contraindications, Precautions and Pharmacology: Pharmacodynamics under Actions).
Medicines increasing the risk of angioedema: Concomitant use of ACE inhibitors with sacubitril/valsartan is contraindicated as this increases the risk of angioedema (see Contraindications and Precautions).
Concomitant use of ACE inhibitors with racecadotril, mTOR inhibitors (e.g. sirolimus, everolimus, temsirolimus) and gliptins (e.g. linagliptin, saxagliptin, sitagliptin, vildagliptin) may lead to an increased risk for angioedema (see Precautions).
Drugs inducing hyperkalaemia: Some drugs or therapeutic classes may increase the occurrence of hyperkalaemia: aliskiren, potassium salts, potassium-sparing diuretics, ACE inhibitors, angiotensin-II receptor antagonists, NSAIDs, heparins, immunosuppressant agents such as ciclosporin or tacrolimus, trimethoprim and Co-trimoxazole (trimethoprim/sulfamethoxazole). The combination of Viacoram with these drugs increases the risk of hyperkalaemia (see Precautions). Therefore, the combination of Viacoram with the previously mentioned drugs is not recommended. If concomitant use is indicated, they should be used with caution and with frequent monitoring of serum potassium.
Concomitant use contraindicated (see Contraindications): Aliskiren: In diabetic or impaired renal patients, risk of hyperkalaemia, worsening of renal function and cardiovascular morbidity and mortality increase.
Extracorporeal treatments: Extracorporeal treatments leading to contact of blood with negatively charged surfaces such as dialysis or haemofiltration with certain high-flux membranes (e.g. polyacrylonitril membranes) and low density lipoprotein apheresis with dextran sulphate due to increased risk of severe anaphylactoid reactions (see Contraindications). If such treatment is required, consideration should be given to using a different type of dialysis membrane or a different class of antihypertensive agent.
Sacubitril/valsartan: The concomitant use of perindopril with sacubitril/valsartan is contraindicated, as the concomitant inhibition of neprilysin (NEP) and ACE may increase the risk of angioedema. Sacubitril/valsartan must not be started until 36 hours after taking the last dose of perindopril therapy. Perindopril therapy must not be started until 36 hours after the last dose of sacubitril/valsartan (see Contraindications and Precautions).
Concomitant use not recommended (see Precautions): Estramustine: Risk of increased adverse effects such as angioneurotic oedema (angioedema).
Potassium-sparing diuretics (e.g. triamterene, amiloride), potassium (salts): Hyperkalaemia (potentially lethal), especially in conjunction with renal impairment (additive hyperkalaemic effects). ACE inhibitors must not be associated with hyperkalaemic substances, except in hypokalaemia.
The combination of Viacoram with the previously mentioned drugs is not recommended (see Precautions). If concomitant use is nonetheless indicated, they should be used with caution and with frequent monitoring of serum potassium. For use of spironolactone in heart failure, see as follows.
Lithium: Reversible increases in serum lithium concentrations and toxicity have been reported during concomitant administration of lithium with ACE inhibitors. Use of Viacoram with lithium is not recommended, but if the combination proves necessary, careful monitoring of serum lithium levels should be performed (see Precautions).
Dantrolene (infusion): In animals, lethal ventricular fibrillation and cardiovascular collapse are observed in association with hyperkalaemia after administration of verapamil and intravenous dantrolene. Due to risk of hyperkalaemia, it is recommended that the co-administration of Viacoram containing amlodipine, a calcium channel blocker, be avoided in patients susceptible to malignant hyperthermia and in the management of malignant hyperthermia.
Concomitant use which requires special care: Antidiabetic agents (insulins, oral hypoglycaemic agents): Epidemiological studies have suggested that concomitant administration of ACE inhibitors and antidiabetic medicines (insulins, oral hypoglycaemic agents) may cause an increased blood-glucose lowering effect with risk of hypoglycaemia. This phenomenon appeared to be more likely to occur during the first weeks of combined treatment and in patients with renal impairment.
Baclofen: Increased antihypertensive effect. Monitor blood pressure and adapt antihypertensive dosage if necessary.
Non-potassium-sparing diuretics: Patients on diuretics, and especially those who are volume and/or salt depleted, may experience excessive reduction in blood pressure after initiation of therapy with an ACE inhibitor. The possibility of hypotensive effects can be reduced by discontinuation of the diuretic, by increasing volume or salt intake prior to initiating Viacoram.
In arterial hypertension, when prior diuretic therapy can have caused salt/volume depletion, the diuretic must be discontinued before initiating Viacoram, in which case a non-potassium-sparing diuretic can be thereafter reintroduced.
Renal function (creatinine levels) must be monitored during the first few weeks of Viacoram therapy.
Potassium-sparing diuretics (eplerenone, spironolactone): With eplerenone or spironolactone at doses between 12.5 mg to 50 mg by day and with low doses of ACE inhibitors: In the treatment of class II-IV heart failure (NYHA) with an ejection fraction <40%, and previously treated with ACE inhibitors and loop diuretics, risk of hyperkalaemia, potentially lethal, especially in case of non-observance of the prescription recommendations on this combination.
Before initiating the combination, check the absence of hyperkalaemia and renal impairment.
A close monitoring of the kalaemia and creatininemia is recommended in the first month of the treatment once a week at the beginning and, monthly thereafter.
Non-steroidal anti-inflammatory medicinal products (NSAIDs) including aspirin ≥3 g/day: When ACE-inhibitors are administered simultaneously with non-steroidal anti-inflammatory drugs (i.e. acetylsalicylic acid at anti-inflammatory dosage regimens, COX-2 inhibitors and non-selective NSAIDs), attenuation of the antihypertensive effect may occur. Concomitant use of Viacoram and NSAIDs may lead to an increased risk of worsening of renal function, including possible acute renal failure, and an increase in serum potassium, especially in patients with poor pre-existing renal function. The combination should be administered with caution, especially in the elderly. Patients should be adequately hydrated and consideration should be given to monitoring renal function after initiation of concomitant therapy, and periodically thereafter.
Ciclosporin: Hyperkalaemia may occur during concomitant use of ACE inhibitors with ciclosporin. Monitoring of serum potassium is recommended.
Heparin: Hyperkalaemia may occur during concomitant use of ACE inhibitors with heparin. Monitoring of serum potassium is recommended.
Racecadotril: ACE inhibitors (e.g. perindopril) are known to cause angioedema. This risk may be elevated when used concomitantly with racecadotril (a drug used against acute diarrhoea) (see Precautions).
mTOR inhibitors (e.g. sirolimus, everolimus, temsirolimus): Patients taking concomitant mTOR inhibitors therapy may be at increased risk for angioedema (see Precautions).
Gliptins (e.g. linagliptin, saxagliptin, sitagliptin, vildagliptin): Increased risk of angioedema, due to dipeptidyl peptidase IV (DPP-IV) decreased activity by the gliptin, in patients co-treated with an ACE inhibitor.
CYP3A4 inducers: Upon co-administration of known inducers of the CYP3A4, the plasma concentration of amlodipine may vary. Therefore, blood pressure should be monitored and dose regulation considered both during and after concomitant medication particularly with strong CYP3A4 inducers (e.g. rifampicin, Hypericum perforatum).
CYP3A4 inhibitors: Concomitant use of amlodipine with strong or moderate CYP3A4 inhibitors (protease inhibitors, azole antifungals, macrolides like erythromycin or clarithromycin, verapamil or diltiazem) may give rise to significant increase in amlodipine exposure. The clinical translation of these PK variations may be more pronounced in the elderly. Clinical monitoring and Viacoram dose adjustment may thus be required.
There is an increased risk of hypotension in patients receiving clarithromycin with amlodipine. Close observation of patients is recommended when amlodipine is co-administered with clarithromycin.
Concomitant use which requires some care: Antihypertensive agents (such as beta-blockers) and vasodilators: Concomitant use of these agents may increase the hypotensive effects of Viacoram. Concomitant use with nitroglycerine and other nitrates or other vasodilators, may further reduce blood pressure and therefore should be considered with caution.
Tricyclic antidepressants/Antipsychotics/Anaesthetics: Concomitant use of certain anaesthetic medicinal products, tricyclic antidepressants and antipsychotics with Viacoram may result in further reduction of blood pressure.
Sympathomimetics: Sympathomimetics may reduce the antihypertensive effects of Viacoram.
Corticosteroids, tetracosactide: Reduction in antihypertensive effect (salt and water retention due to corticosteroids).
Alpha-blockers (prazosin, alfuzosin, doxazosin, tamsulosin, terazosin): Increased antihypertensive effect and increased risk of orthostatic hypotension.
Amifostine: May potentiate the antihypertensive effect of amlodipine.
Gold: Nitritoid reactions (symptoms include facial flushing, nausea, vomiting and hypotension) have been reported rarely in patients on therapy with injectable gold (sodium aurothiomalate) and concomitant ACE inhibitor therapy including perindopril.
Grapefruit: Administration of Viacoram with grapefruit or grapefruit juice is not recommended as amlodipine bioavailability may be increased in some patients resulting in increased blood pressure lowering effects.
Tacrolimus: There is a risk of increased tacrolimus blood levels when co-administered with amlodipine. In order to avoid toxicity of tacrolimus, administration of amlodipine in a patient treated with tacrolimus requires monitoring of tacrolimus blood levels and dose adjustment of tacrolimus when appropriate.
Mechanistic Target of Rapamycin (mTOR) Inhibitors: mTOR inhibitors such as sirolimus, temsirolimus, and everolimus are CYP3A substrates. Amlodipine is a weak CYP3A inhibitor. With concomitant use of mTOR inhibitors, amlodipine may increase exposure of mTOR inhibitors.
Ciclosporine: No drug interaction studies have been conducted with ciclosporine and amlodipine in healthy volunteers or other populations with the exception of renal transplant patients, where variable trough concentration increases (average 0% - 40%) of ciclosporine were observed. Consideration should be given for monitoring ciclosporine levels in renal transplant patients on amlodipine, and ciclosporine dose reductions should be made as necessary.
Incompatibilities: Not applicable.
Special precautions for disposal: No special requirements.
Store below 30°C.
Shelf life: 3 years.
Tablet container of 10 tablets: Once opened, Viacoram should be used within 10 days.
Tablet container of 30 tablets: Once opened, Viacoram should be used within 30 days.
C09BB04 - perindopril and amlodipine ; Belongs to the class of ACE inhibitors and calcium channel blockers. Used in the treatment of cardiovascular diseases.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image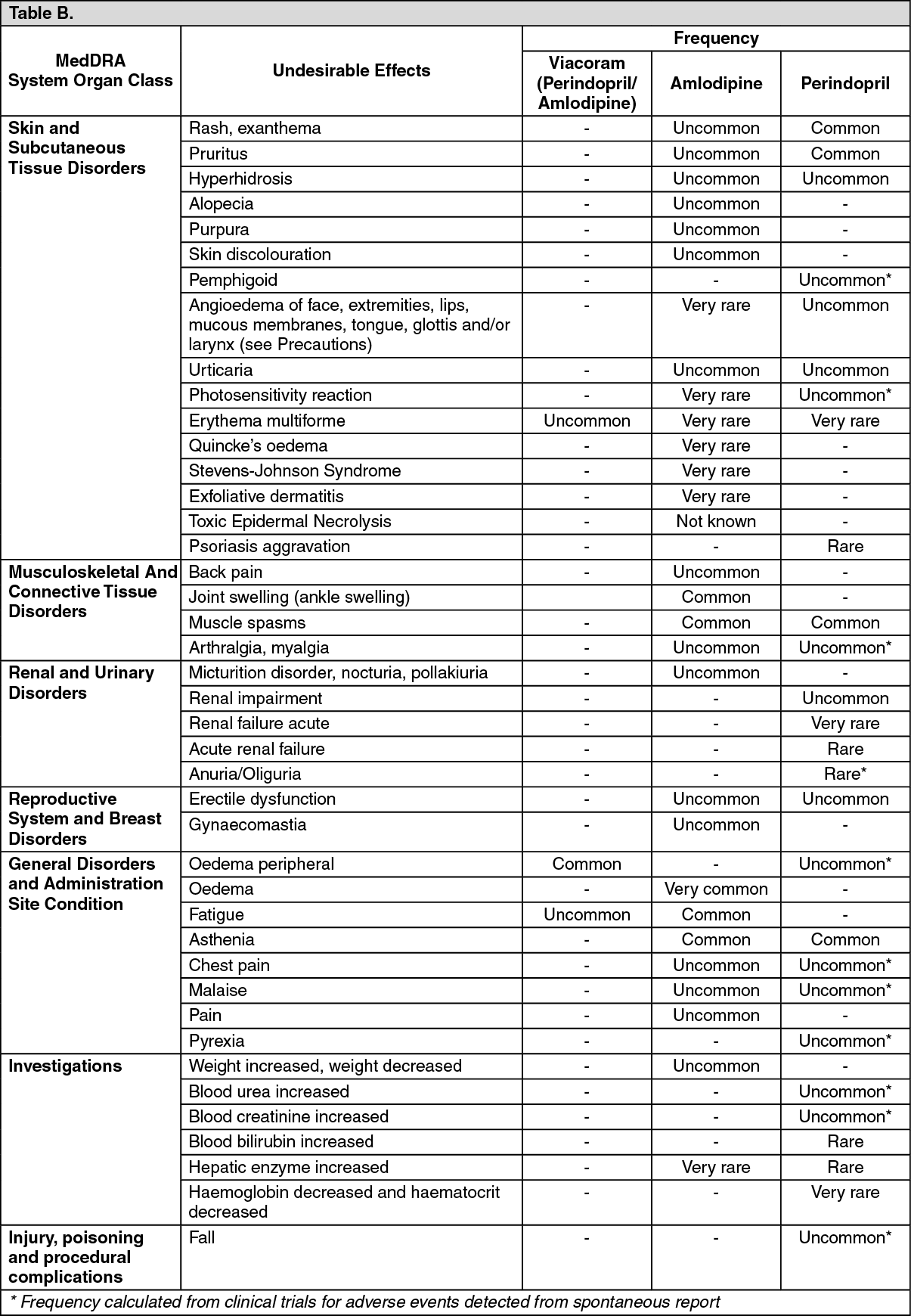 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
