Posology: One dose consists in the administration of 0.5 mL of vaccine via the intramuscular route. The intradermal (ID) route may be used as an alternative. One intradermal dose consists of 0.1 mL of reconstituted vaccine, i.e. 1/5 of the intramuscular dose.
Pre-exposure vaccination: Three doses of VERORAB are administered by intramuscular route at days (D) D0, D7 and D28. The dose scheduled at D28 can be administered at D21. If necessary.
The doses are administered either by IM or ID route. The Intradermal route must not be used for immunocompromised individuals (see Contraindications). Intramuscular injections are preferable if antimalarial chemoprophylaxis (e.g. chloroquine) is being used concurrently or there is a possibility of an immune-compromised state (antibody response may be impaired if the intradermal method is used).
Booster doses are determined based on the risk of exposure and on serological tests in accordance with official recommendations.
VERORAB can be administered as a booster injection after primary vaccination with a cell culture rabies vaccine (a rabies vaccine prepared in VERO cells or prepared in human diploid cells (HDCV)).
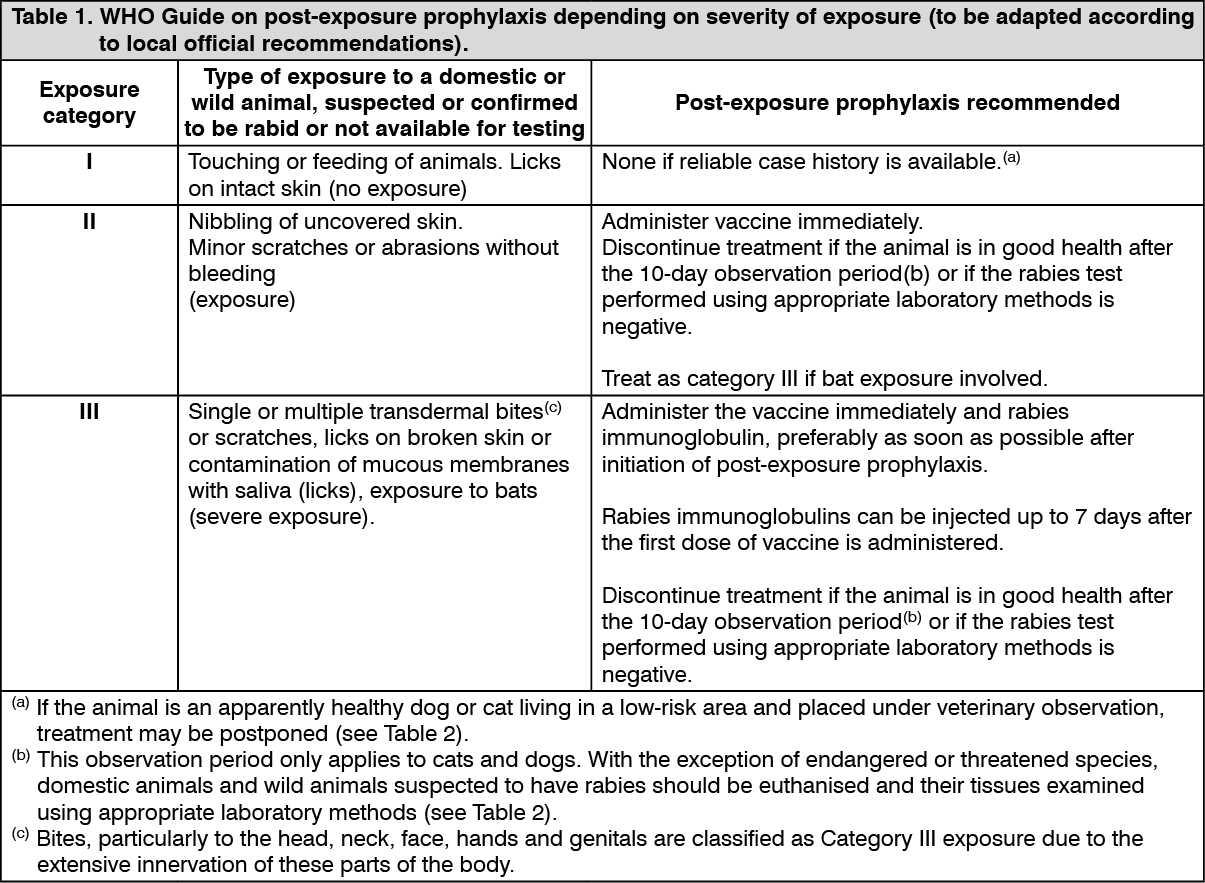
Post-exposure vaccination: Post-exposure prophylaxis includes local non-specific treatment of the wound, vaccination and, where appropriate, passive immunization with rabies immunoglobulins.
Post-exposure prophylaxis should be initiated as soon as possible after suspected exposure to rabies. In all cases, proper wound care (careful washing of all bites and scratches with soap or detergent and copious amounts of water and/or virucidal agents) must be performed immediately or as soon as possible after exposure. It must be performed before administration of vaccine or rabies immunoglobulins, when they are indicated. Post-exposure prophylaxis should be adjusted to the exposure category, the condition of the animal (see Table 2) and the vaccination status of the patient, in accordance with official recommendations (see Table 1, WHO recommendations).
Post-exposure prophylaxis should be performed as soon as possible after exposure under medical supervision and only at a rabies centre.
If necessary, post-exposure prophylaxis can be supplemented by tetanus prophylaxis and antibiotic therapy to prevent the development of infections other than rabies. (See Tables 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Post-exposure prophylaxis of non-immunised subjects:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Post-exposure prophylaxis of non-immunised subjects: Essen regimen: The vaccine should be administered by intramuscular route at D0, D3, D7, D14 and D28 (5 injections of 0.5 ml). Or; Zagreb regimen (schedule 2-1-1): The vaccine should be administered by intramuscular route: one dose in the right deltoid and one dose in the left deltoid at D0, then one dose in the deltoid at D7 and one dose at D21 (4 injections of 0.5 mL). In young children, the vaccine should be administered in the anterolateral region of the thigh muscle. Or; The 2-site intradermal regimen (known as updated Thai Red Cross regimen, 2-2-2-0-2), which prescribes 1 injection of 0.1 mL at 2 sites on days 0, D3, D7, and D28. The Intradermal route must not be used for immunocompromised individuals (see Contraindications).
Whatever the regimen used, vaccination must not be discontinued unless the contact animal is declared free from rabies after veterinary supervision (see Table 2).R abies immunoglobulins should be administered concomitantly with the vaccine, in case of category III exposure (WHO classification, see Table 1). If possible, the vaccine should be administered contralaterally to the immunoglobulin administration sites.
Refer to the Summary of Characteristics of the rabies immunoglobulins used.
Post-exposure prophylaxis for already immunised subjects: In accordance with official recommendations, this applies to subjects who have already received pre exposure prophylaxis or post-exposure prophylaxis or who discontinued post-exposure prophylaxis after receiving at least two doses of vaccine prepared in cell culture.
Subjects who are already immunised should receive 1 dose of vaccine (0.5 mL by intramuscular route) at D0 and 1 dose on D3.
Rabies immunoglobulins are not indicated in this case.
Intradermal schedule: This vaccine is of sufficient potency to allow its safe use in the WHO recommended intradermal post-exposure regimen in countries where relevant national authorities have approved the intradermal route for rabies post-exposure treatment.
Immunocompromised subjects: Pre-exposure prophylaxis: In immunocompromised subjects, blood tests for neutralising antibodies should be performed 2 to 4 weeks following the vaccination to assess the possible need for an additional dose of the vaccine.
Post-exposure prophylaxis: In immunocompromised subjects, a complete vaccine regimen should be administered post-exposure. Rabies immunoglobulins should be administered concomitantly with the vaccine in the event of any category II or III exposure (see table 1).
Paediatric population: VERORAB can be administered to children and to adults using the same posology.
Method of administration: Precautions to be taken before handling or administering the medicinal product.
The vaccine is administered via the intramuscular route, in the anterolateral region of the thigh muscle in infants and young children and in the deltoid muscle in older children and adults.
The intradermal (ID) injection may be used as an alternative, in upper arm or forearm.
Do not inject in the buttocks region.
Do not inject via the intravascular route.
For instructions on reconstitution of the medicinal product before administration, see Contraindications




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image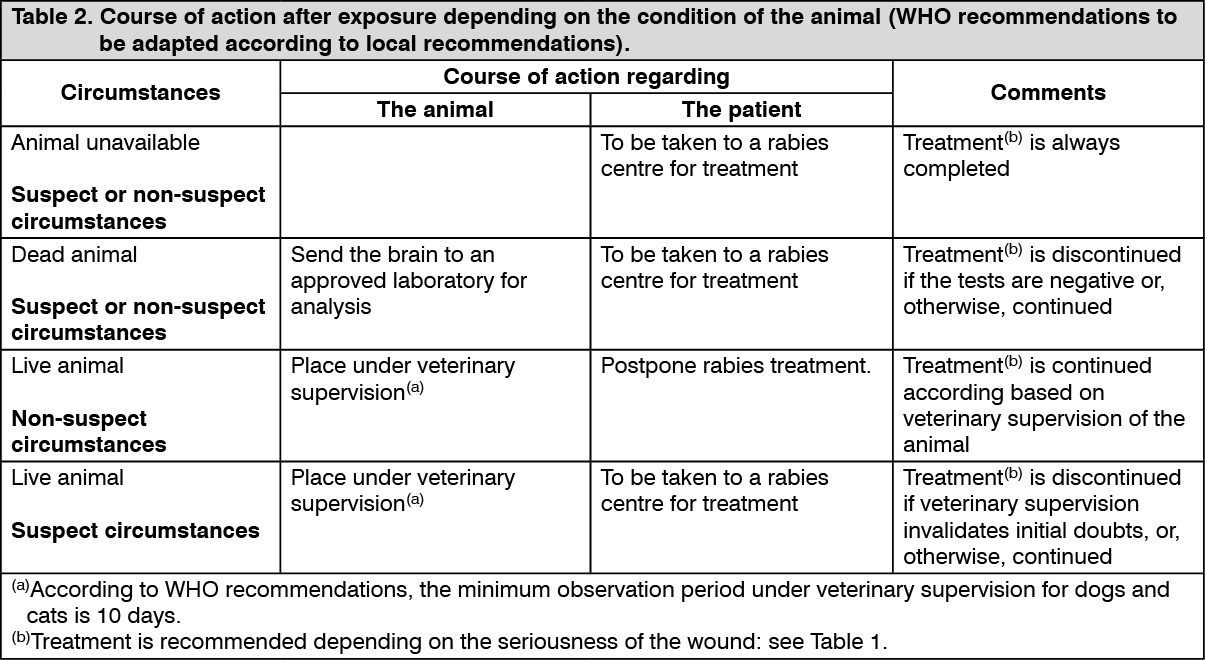 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image (pre-filled syringe)10b520bb-d998-43bc-b2b8-a16a00ea75d5.GIF)

 Sign Out
Sign Out
