


 Sign Out
Sign Out

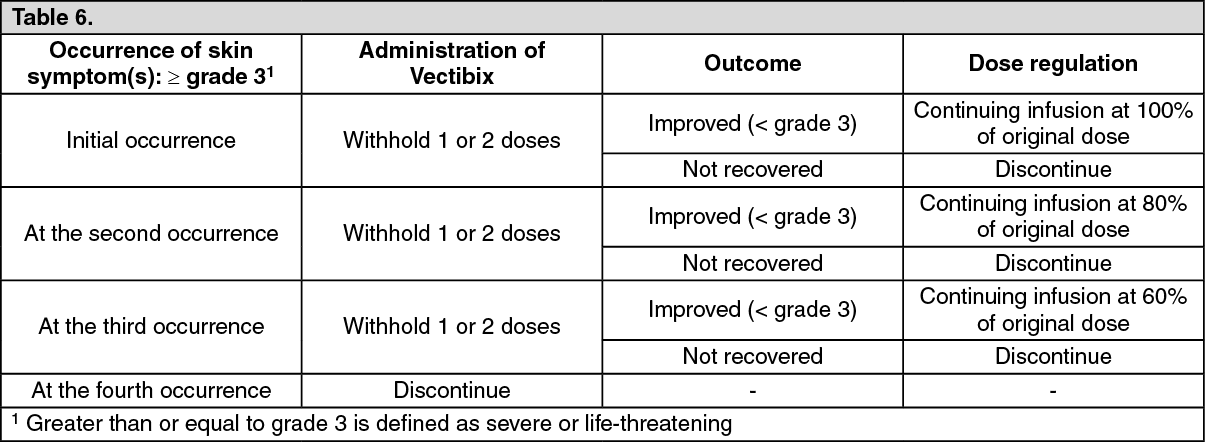
Dermatologic reactions and soft tissue toxicity: Dermatologic related reactions, a pharmacologic effect observed with epidermal growth factor receptor (EGFR) inhibitors, are experienced with nearly all patients (approximately 94%) treated with Vectibix. Severe (NCI-CTC grade 3) skin reactions were reported in 23% and life-threatening (NCI-CTC grade 4) skin reactions in < 1% of patients who received Vectibix monotherapy and in combination with chemotherapy (n = 2,224) (see Adverse Reactions). If a patient develops dermatologic reactions that are grade 3 (CTCAE v 4.0) or higher, or that are considered intolerable, the following dose modification is recommended: (see Table 6).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn clinical studies, subsequent to the development of severe dermatologic reactions (including stomatitis), infectious complications including sepsis and necrotising fasciitis, in rare cases leading to death, and local abscesses requiring incisions and drainage were reported. Patients who have severe dermatologic reactions or soft tissue toxicity or who develop worsening reactions whilst receiving Vectibix should be monitored for the development of inflammatory or infectious sequelae (including cellulitis and necrotising fasciitis), and appropriate treatment promptly initiated. Life threatening and fatal infectious complications including necrotising fasciitis and sepsis have been observed in patients treated with Vectibix. Rare cases of Stevens-Johnson syndrome and toxic epidermal necrolysis have been reported in patients treated with Vectibix in the post-marketing setting. Withhold or discontinue Vectibix in the event of dermatologic or soft tissue toxicity associated with severe or life-threatening inflammatory or infectious complications.
Treatment and management of dermatologic reactions should be based on severity and may include a moisturiser, sunscreen (SPF > 15 UVA and UVB), and topical steroid cream (not stronger than 1% hydrocortisone) applied to affected areas, and/or oral antibiotics (e.g. doxycycline). It is also recommended that patients experiencing rash/dermatological toxicities wear sunscreen and hats and limit sun exposure as sunlight can exacerbate any skin reactions that may occur. Patients may be advised to apply moisturiser and sunscreen to face, hands, feet, neck, back and chest every morning during treatment, and to apply the topical steroid to face, hands, feet, neck, back and chest every night during treatment.
Pulmonary complications: Patients with a history of, or evidence of, interstitial pneumonitis or pulmonary fibrosis were excluded from clinical studies. Cases of interstitial lung disease (ILD), both fatal and non-fatal, have been reported, mainly from the Japanese population. In the event of acute onset or worsening pulmonary symptoms, Vectibix treatment should be interrupted and a prompt investigation of these symptoms should occur. If ILD is diagnosed, Vectibix should be permanently discontinued and the patient should be treated appropriately. In patients with a history of interstitial pneumonitis or pulmonary fibrosis, the benefits of therapy with panitumumab versus the risk of pulmonary complications must be carefully considered.
Electrolyte disturbances: Progressively decreasing serum magnesium levels leading to severe (grade 4) hypomagnesaemia have been observed in some patients. Patients should be periodically monitored for hypomagnesaemia and accompanying hypocalcaemia prior to initiating Vectibix treatment, and periodically thereafter for up to 8 weeks after the completion of treatment (see Adverse Reactions). Magnesium repletion is recommended, as appropriate.
Other electrolyte disturbances, including hypokalaemia, have also been observed. Monitoring as above and repletion as appropriate of these electrolytes is also recommended.
Infusion related reactions: Across monotherapy and combination mCRC clinical studies (n = 2,224), infusion-related reactions (occurring within 24 hours of an infusion) were reported in Vectibix-treated patients, including severe infusion-related reactions (NCI-CTC grade 3 and grade 4).
In the post-marketing setting, serious infusion-related reactions have been reported, including rare post-marketing reports with a fatal outcome. If a severe or life-threatening reaction occurs during an infusion or at any time post-infusion [e.g. presence of bronchospasm, angioedema, hypotension, need for parenteral treatment, or anaphylaxis], Vectibix should be permanently discontinued (see Contraindications and Adverse Reactions).
In patients experiencing a mild or moderate (CTCAE v 4.0 grades 1 and 2) infusion-related reaction the infusion rate should be reduced for the duration of that infusion. It is recommended to maintain this lower infusion rate in all subsequent infusions.
Hypersensitivity reactions occurring more than 24 hours after infusion have been reported including a fatal case of angioedema that occurred more than 24 hours after the infusion. Patients should be informed of the possibility of a late onset reaction and instructed to contact their physician if symptoms of a hypersensitivity reaction occur.
Acute renal failure: Acute renal failure has been observed in patients who develop severe diarrhoea and dehydration. Patients who experience severe diarrhoea should be instructed to consult a healthcare professional urgently.
Vectibix in combination with irinotecan, bolus 5-fluorouracil, and leucovorin (IFL) chemotherapy: Patients receiving Vectibix in combination with the IFL regimen [bolus 5-fluorouracil (500 mg/m2), leucovorin (20 mg/m2) and irinotecan (125 mg/m2)] experienced a high incidence of severe diarrhoea (see Adverse Reactions). Therefore administration of Vectibix in combination with IFL should be avoided (see Interactions).
Vectibix in combination with bevacizumab and chemotherapy regimens: Shortened progression-free survival time and increased deaths were observed in the patients receiving Vectibix in combination with bevacizumab and chemotherapy. A greater frequency of pulmonary embolism, infections (predominantly of dermatologic origin), diarrhoea, electrolyte imbalances, nausea, vomiting and dehydration was also observed in the treatment arms using Vectibix in combination with bevacizumab and chemotherapy. Vectibix should not be administered in combination with bevacizumab containing chemotherapy (see Interactions and Pharmacology: Pharmacodynamics under Actions).
Vectibix in combination with oxaliplatin-based chemotherapy in patients with mutant RAS mCRC or for whom RAS tumour status is unknown: The combination of Vectibix with oxaliplatin-containing chemotherapy is contraindicated for patients with mutant RAS mCRC or for whom RAS mCRC status is unknown (see Contraindications and Pharmacology: Pharmacodynamics under Actions).
A shortened progression-free survival (PFS) and overall survival (OS) time were observed in patients with mutant KRAS (exon 2) tumours and additional RAS mutations (KRAS [exons 3 and 4] or NRAS [exons 2, 3, 4]) who received panitumumab in combination with infusional 5-fluorouracil, leucovorin, and oxaliplatin (FOLFOX) versus FOLFOX alone (see Pharmacology: Pharmacodynamics under Actions).
RAS mutational status should be determined using a validated test method by an experienced laboratory (see Dosage & Administration). If Vectibix is to be used in combination with FOLFOX then it is recommended that mutational status be determined by a laboratory that participates in a RAS External Quality Assurance programme or wild-type status be confirmed in a duplicate test.
Ocular toxicities: Serious cases of keratitis and ulcerative keratitis, which may lead to corneal perforation, have been reported. Patients presenting with signs and symptoms suggestive of keratitis such as acute or worsening: eye inflammation, lacrimation, light sensitivity, blurred vision, eye pain and/or red eye should be referred promptly to an ophthalmology specialist.
If a diagnosis of ulcerative keratitis is confirmed, treatment with Vectibix should be interrupted or discontinued. If keratitis is diagnosed, the benefits and risks of continuing treatment should be carefully considered.
Vectibix should be used with caution in patients with a history of keratitis, ulcerative keratitis or severe dry eye. Contact lens use is also a risk factor for keratitis and ulceration.
Patients with ECOG 2 performance status treated with Vectibix in combination with chemotherapy: For patients with ECOG 2 performance status, assessment of benefit-risk is recommended prior to initiation of Vectibix in combination with chemotherapy for treatment of mCRC. A positive benefit-risk balance has not been documented in patients with ECOG 2 performance status.
Warning for excipients: This medicinal product contains 3.45 mg sodium per mL, equivalent to 0.17% of the WHO recommended maximum daily intake of 2 g sodium for an adult.
Effects on ability to drive and use machines: Vectibix may have a minor influence on the ability to drive and use machines. If patients experience treatment-related symptoms affecting their vision and/or ability to concentrate and react, it is recommended that they do not drive or use machines until the side effect subsides.
Use in Elderly: No overall differences in safety or efficacy were observed in elderly patients (≥ 65 years of age) treated with Vectibix monotherapy. However, an increased number of serious adverse events were reported in elderly patients treated with Vectibix in combination with FOLFIRI or FOLFOX chemotherapy compared to chemotherapy alone (see Adverse Reactions).