Pharmacology: Mechanism of action: Varilrix produces an attenuated clinically inapparent varicella infection in susceptible subjects. The presence of antibodies is accepted to be an indication of protection.
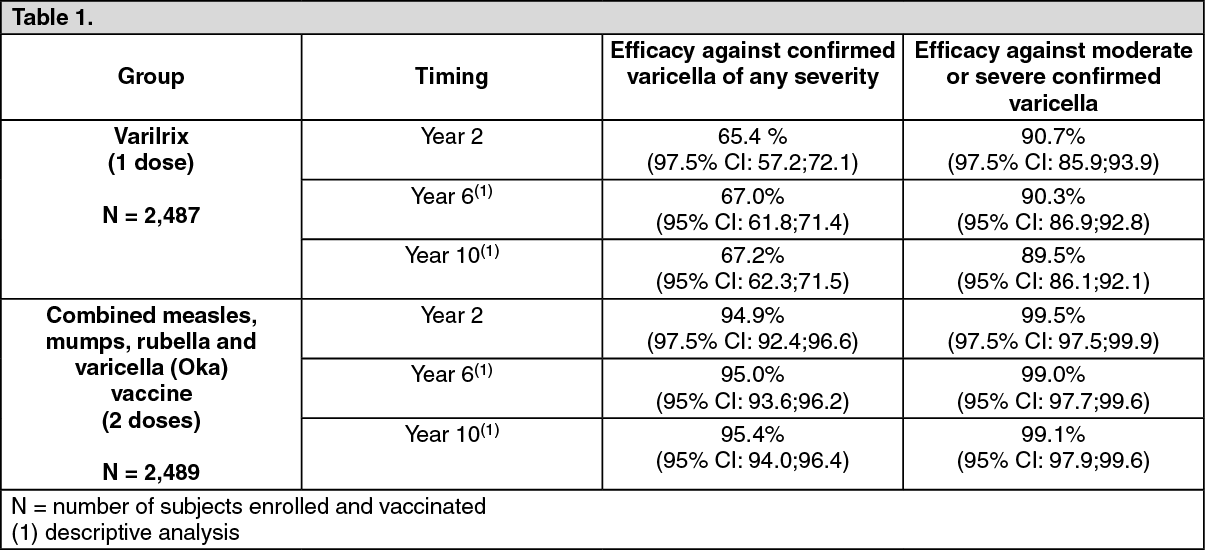
Pharmacodynamics: Efficacy and effectiveness: The efficacy of GlaxoSmithKline's Oka varicella vaccines in preventing confirmed varicella disease (by Polymerase Chain Reaction (PCR) or exposure to varicella case) has been evaluated in a large active controlled multicountry clinical trial in which children aged 12-22 months received one dose of Varilrix or two doses of combined measles, mumps, rubella and varicella (Oka) vaccine. Vaccine efficacy against confirmed varicella of any severity and against moderate or severe confirmed varicella was demonstrated after a primary follow-up period of 2 years (median duration 3.2 years). Persistent efficacy was observed in the same study during the long-term follow-up periods of 6 years (median duration 6.4 years) and 10 years (median duration 9.8 years). The data are presented in the Table 1 as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The effectiveness of one dose of Varilrix was estimated in different settings (outbreaks, case-control and database studies) and ranged from 20%-92% against any varicella disease and from 86%-100% against moderate or severe disease.
The impact of one dose of Varilrix in reducing varicella hospitalisations and ambulatory visits among children were respectively 81% and 87% overall.
Effectiveness data suggest a higher level of protection and a decrease in breakthrough varicella following two doses of vaccine than following one dose.
Immune response after subcutaneous administration: Healthy subjects: In children aged 11 months to 21 months, the seroconversion rate when measured by ELISA (50 mIU/ml) 6 weeks after vaccination was 89.6% after one vaccine dose and 100% after the second vaccine dose.
In children aged 9 months to 12 years, the overall seroconversion rate when measured by Immunofluorescence Assay (IFA) 6 weeks after vaccination was >98% after one vaccine dose.
In children aged 9 months to 6 years, the seroconversion rate when measured by IFA 6 weeks after vaccination was 100% after a second vaccine dose. A marked increase of antibody titres was observed following the administration of a second dose (5 to 26-fold GMT increase).
In subjects aged 13 years and above, the seroconversion rate when measured by IFA 6 weeks after vaccination was 100% after the second vaccine dose. One year after vaccination, all subjects tested were still seropositive.
In clinical trials, the majority of vaccinated subjects who were subsequently exposed to wild-type virus were either completely protected from clinical chickenpox or developed a milder form of the disease (i.e. low number of vesicles, absence of fever).
There are insufficient data to assess the rate of protection against complications of chickenpox such as encephalitis, hepatitis or pneumonia.
High-risk patients: There are only very limited data from clinical trials available in patients at high risk of varicella. The overall seroconversion rate in these patients was found to be ≥80%.
In high-risk patients, periodic measurement of varicella antibodies after immunisation may be indicated in order to identify those who may benefit from re-immunisation.
Transmission of the Oka vaccine virus as shown by virus isolation and identification has been demonstrated in four cases in siblings of immuno-compromised vaccinees who had a vesicular eruption. Whenever those siblings of immuno-compromised vaccinees developed themselves a post-exposure rash, it was always very mild.
Immune response after intramuscular administration: The immunogenicity of Varilrix administered intramuscularly is based on a comparative study where 283 healthy children aged 11 to 21 months received GSK's combined measles, mumps, rubella and varicella vaccine (containing the same varicella strain as Varilrix) either by subcutaneous or intramuscular route. Comparable immunogenicity was demonstrated for both administration routes.
Clinical Studies: See Pharmacodynamics as previously mentioned.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
