Pharmacotherapeutic group: angiotensin II receptor blocker, plain (telmisartan), combinations with dihydropyridine derivatives (amlodipine).
ATC Code: C09DB04.
Pharmacology: Mode of action: TWYNSTA combines two antihypertensive compounds with complementary mechanisms to control blood pressure in patients with essential hypertension: an angiotensin II receptor blocker, telmisartan, and a dihydropyridinic calcium channel blocker, amlodipine.
The combination of these substances has an additive antihypertensive effect, reducing blood pressure to a greater degree than either component alone.
TWYNSTA once daily produces effective and consistent reductions in blood pressure across the 24-hour therapeutic dose range.
Telmisartan:
Telmisartan is an orally effective and specific angiotensin II receptor (type AT1) blocker. Telmisartan displaces angiotensin II with very high affinity from its binding site at the AT1 receptor subtype, which is responsible for the known actions of angiotensin II. Telmisartan does not exhibit any partial agonist activity at the AT1 receptor. Telmisartan selectively binds the AT1 receptor. The binding is long lasting.
Telmisartan does not show affinity for other receptors, including AT2 and other less characterised AT receptors. The functional role of these receptors is not known, nor is the effect of their possible overstimulation by angiotensin II, whose levels are increased by telmisartan. Plasma aldosterone levels are decreased by telmisartan. Telmisartan does not inhibit human plasma renin or block ion channels. Telmisartan does not inhibit angiotensin converting enzyme (kininase II), the enzyme which also degrades bradykinin. Therefore, it is not expected to potentiate bradykinin-mediated adverse effects.
In man, an 80 mg dose of telmisartan almost completely inhibits the angiotensin II evoked blood pressure increase. The inhibitory effect is maintained over 24 hours and still measurable up to 48 hours.
Amlodipine: Amlodipine is a calcium ion influx inhibitor of the dihydropyridine group (slow channel blocker or calcium ion blocker) and inhibits the transmembrane influx of calcium ions into cardiac and vascular smooth muscle.
The mechanism of the antihypertensive action of amlodipine is due to a direct relaxant effect on vascular smooth muscle, leading to reductions in peripheral vascular resistance and in blood pressure. Experimental data indicate that amlodipine binds to both dihydropyridine and non-dihydropyridine binding sites. Amlodipine is relatively vessel-selective, with a greater effect on vascular smooth muscle cells than on cardiac muscle cells.
Pharmacodynamics: Telmisartan: After the first dose of telmisartan, the antihypertensive activity gradually becomes evident within 3 hours. The maximum reduction in blood pressure is generally attained 4 weeks after the start of treatment and is sustained during long-term therapy.
The antihypertensive effect persists constantly over 24 hours after dosing and includes the last 4 hours before the next dose as shown by ambulatory blood pressure measurements. This is confirmed by trough to peak ratios consistently above 80 % seen after doses of 40 and 80 mg of telmisartan in placebo controlled clinical studies. There is an apparent trend to a dose relationship to a time to recovery of baseline SBP. In this respect data concerning DBP are inconsistent.
In patients with hypertension telmisartan reduces both systolic and diastolic blood pressure without affecting pulse rate.
The antihypertensive efficacy of telmisartan is comparable to that of agents representative of other classes of antihypertensive drugs (demonstrated in clinical trials comparing telmisartan to amlodipine, atenolol, enalapril, hydrochlorothiazide, losartan, lisinopril, ramipril and valsartan).
Upon abrupt cessation of treatment with telmisartan, blood pressure gradually returns to pre-treatment values over a period of several days without evidence of rebound hypertension.
Telmisartan treatment has been shown in clinical trials to be associated with statistically significant reductions in Left Ventricular Mass and Left Ventricular Mass Index in patients with hypertension and Left Ventricular Hypertrophy.
Telmisartan treatment has been shown in clinical trials (including comparators like losartan, ramipril and valsartan) to be associated with statistically significant reductions in proteinuria (including microalbuminuria and macroalbuminuria) in patients with hypertension and diabetic nephropathy.
The incidence of dry cough was significantly lower in patients treated with telmisartan than in those given angiotensin converting enzyme inhibitors in clinical trials directly comparing the two antihypertensive treatments.
Amlodipine: In patients with hypertension, once daily dosing provides clinically significant reductions of blood pressure in both the supine and standing positions throughout the 24 hour interval. Due to the slow onset of action, acute hypotension is not a feature of amlodipine administration.
In hypertensive patients with normal renal function, therapeutic doses of amlodipine resulted in a decrease in renal vascular resistance and an increase in glomerular filtration rate and effective renal plasma flow, without change in filtration fraction or proteinuria.
Clinical Trials: Telmisartan:
Prevention of cardiovascular morbidity and mortality: ONTARGET (ONgoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial) compared the effects of telmisartan, ramipril and the combination of telmisartan and ramipril on cardiovascular outcomes in 25620 patients aged 55 years or older with a history of coronary artery disease, stroke, peripheral vascular disease, or diabetes mellitus accompanied by evidence of end-organ damage (e.g. retinopathy, left ventricular hypertrophy, macro- or microalbuminuria), which represents a broad cross-section of cardiovascular high risk patients.
Patients were randomized to one of the three following treatment groups: telmisartan 80 mg (n = 8542), ramipril 10 mg (n = 8576), or the combination of telmisartan 80 mg plus ramipril 10 mg (n = 8502), and followed for a mean observation time of 4.5 years. The population studied was 73% male, 74% Caucasian, 14% Asian and 43% were 65 years of age or older. Hypertension was present in nearly 83% of randomized patients: 69% of patients had a history of hypertension at randomization and an additional 14% had actual blood pressure readings above 140/90 mm Hg. At baseline, the total percentage of patients with a medical history of diabetes was 38% and an additional 3% presented with elevated fasting plasma glucose levels. Baseline therapy included acetylsalicylic acid (76%), statins (62%), beta-blockers (57%), calcium channel blockers (34%), nitrates (29%) and diuretics (28%).
The primary endpoint was a composite of cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, or hospitalization for congestive heart failure.
Adherence to treatment was better for telmisartan than for ramipril or the combination of telmisartan and ramipril, although the study population had been pre-screened for tolerance to treatment with an ACE-inhibitor. The analysis of adverse events leading to permanent treatment discontinuation and of serious adverse events showed that cough and angioedema were less frequently reported in patients treated with telmisartan than in patients treated with ramipril, whereas hypotension was more frequently reported with telmisartan.
Telmisartan had similar efficacy to ramipril in reducing the primary endpoint. The incidence of the primary endpoint was similar in the telmisartan (16.7%), ramipril (16.5%) and telmisartan plus ramipril combination (16.3%) arms. The hazard ratio for telmisartan vs. ramipril was 1.01 (97.5% CI 0.93 - 1.10, p (non-inferiority) = 0.0019). The treatment effect was found to persist following corrections for differences in systolic blood pressure at baseline and over time. There was no difference in the primary endpoint based on age, gender, race, baseline therapies or underlying disease.
Telmisartan was also found to be similarly effective to ramipril in several pre-specified secondary endpoints, including a composite of cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke, the primary endpoint in the reference study HOPE (The Heart Outcomes Prevention Evaluation Study), which had investigated the effect of ramipril vs. placebo. The hazard ratio of telmisartan vs. ramipril for this endpoint in ONTARGET was 0.99 (97.5% CI 0.90 - 1.08, p (non-inferiority) = 0.0004).
Combining telmisartan with ramipril did not add further benefit over ramipril or telmisartan alone. In addition, there was a significantly higher incidence of hyperkalaemia, renal failure, hypotension and syncope in the combination arm. Therefore, the use of a combination of telmisartan and ramipril is not recommended in this population.
Amlodipine:
Amlodipine has not been associated with any adverse metabolic effects or changes in plasma lipids and is suitable for use in patients with asthma, diabetes, and gout.
Use in Patients with Heart Failure: Haemodynamic studies and exercise based controlled clinical trials in NYHA Class II-IV heart failure patients have shown that amlodipine did not lead to clinical deterioration as measured by exercise tolerance, left ventricular ejection fraction and clinical symptomatology.
A placebo controlled study (PRAISE) designed to evaluate patients in NYHA Class III-IV heart failure receiving digoxin, diuretics and ACE inhibitors has shown that amlodipine did not lead to an increase in risk of mortality or combined mortality and morbidity with heart failure.
In a follow-up, long term, placebo controlled study (PRAISE-2) of amlodipine in patients with NYHA III and IV heart failure without clinical symptoms or objective findings suggestive or underlying ischaemic disease, on stable doses of ACE inhibitors, digitalis, and diuretics, amlodipine had no effect on total cardiovascular mortality. In this same population amlodipine was associated with increased reports of pulmonary oedema.
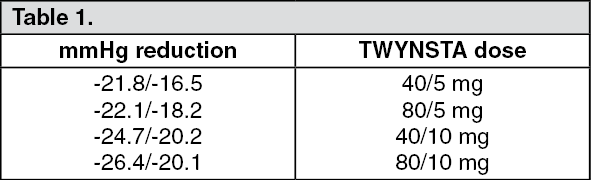
Fixed dose combination (TWYNSTA): In an 8-week multicenter, randomised, double-blind, placebo-controlled, parallel group factorial study 1461 patients with mild to severe hypertension (mean seated diastolic blood pressure ≥95 and <110 mmHg) underwent a 3-4 week placebo run-in period in order to wash out all antihypertensive medications before they were randomised to a double-blind active treatment. Treatment with each combination dose of TWYNSTA resulted in significantly greater diastolic and systolic blood pressure reductions and higher control rates compared to the respective monotherapy components.
The telmisartan/amlodipine combinations showed dose-related reductions in systolic/diastolic blood pressure across the therapeutic dose range: (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The proportions of patients reaching a diastolic blood pressure <90 mmHg with a telmisartan/amlodipine combination were: (See Table 2.)
Click on icon to see table/diagram/image
A subset of 1050 patients in the factorial design study had moderate to severe hypertension (DBP ≥100 mmHg). In these patients who are likely to need more than one antihypertensive agent to achieve blood pressure goal, the observed mean changes in systolic/diastolic blood pressure with a combination therapy containing amlodipine 5 mg (-22.2/-17.2 mmHg with 40/5 mg; -22.5/-19.1 mmHg with 80/5 mg) were comparable to or greater than those seen with amlodipine 10 mg (-21.0/-17.6 mmHg). Additionally, combination therapy showed notably lower oedema rates (1.4% with 40/5 mg; 0.5% with 80/5 mg; 17.6% with amlodipine 10 mg).
The majority of the antihypertensive effect was attained within 2 weeks after initiation of therapy.
Automated ambulatory blood pressure monitoring (ABPM) performed in a subset of 562 patients confirmed the results seen with in-clinic systolic and diastolic blood pressure reductions consistently over the entire 24-hours dosing period.
In a further multicentre, double-blind, active-controlled study, a total of 1097 patients with mild to severe hypertension who were not adequately controlled on amlodipine 5 mg received TWYNSTA (40/5 mg or 80/5 mg) or amlodipine alone (5 mg or 10 mg). After 8 weeks of treatment, each of the combination was statistically significantly superior to both amlodipine monotherapy doses in reducing systolic and diastolic blood pressures: (See Table 3.)
Click on icon to see table/diagram/image
The proportions of patients with normalisation of blood pressure (trough seated diastolic blood pressure <90 mmHg at the end of the trial) were 56.7% with TWYNSTA 40/5 mg and 63.8% with TWYNSTA 80/5 mg compared to 42.0% with amlodipine 5 mg and 56.7% with amlodipine 10 mg.
Oedema related events (peripheral oedema, generalised oedema, and oedema) were significantly lower in patients who received TWYNSTA (40/5 mg or 80/5 mg) as compared to patients who received amlodipine 10 mg (4.4% vs. 24.9%, respectively).
In another multicentre, double-blind, active-controlled study, a total of 947 patients with mild to severe hypertension who were not adequately controlled on amlodipine 10 mg received TWYNSTA (40/10 mg or 80/10 mg) or amlodipine alone (10 mg). After 8 weeks, each of the combination treatments was statistically significantly superior to amlodipine monotherapy in reducing diastolic and systolic blood pressures: (See Table 4.)
Click on icon to see table/diagram/image
The proportions of patients with normalisation of blood pressure (trough seated diastolic blood pressure <90 mmHg at the end of the trial) were 63.7% with TWYNSTA 40/10 mg and 66.5% with TWYNSTA 80/10 mg compared to 51.1% with amlodipine 10 mg.
In two corresponding open-label long-term follow up studies performed over a further 6 months the effect of TWYNSTA was maintained over the trial period.
In patients not adequately controlled on amlodipine 5 mg, TWYNSTA achieved similar (40/5 mg) or better (80/5mg) blood pressure control compared to amlodipine 10 mg with significantly less oedema.
In patients adequately controlled on amlodipine 10 mg but who experience unacceptable oedema, TWYNSTA 40/5 mg or 80/5 mg may achieve similar blood pressure control with less oedema.
The antihypertensive effect of TWYNSTA was similar irrespective of age and gender, and was similar in patients with and without diabetes.
TWYNSTA has not been studied in any patient population other than hypertension. Telmisartan has been studied in a large outcome study in 25620 patients with high cardiovascular risk (ONTARGET). Amlodipine has been studied in patients with chronic stable angina, vasospastic angina and angiographically documented coronary artery disease.
Pharmacokinetics: Pharmacokinetics of the fixed dose combination: The rate and extent of absorption of TWYNSTA are equivalent to the bioavailability of telmisartan and amlodipine when administered as individual tablets.
Pharmacokinetic of the single components: Absorption: Absorption of telmisartan is rapid although the amount absorbed varies. The mean absolute bioavailability for telmisartan is about 50%.
When telmisartan is taken with food, the reduction in the area under the plasma concentration-time curve (AUC) of telmisartan varies from approximately 6% (40 mg dose) to approximately 19% (160 mg dose). By 3 hours after administration plasma concentrations are similar whether telmisartan is taken fasting or with food.
The small reduction in AUC is not expected to cause a reduction in the therapeutic efficacy.
After oral administration of therapeutic doses of amlodipine alone, peak plasma concentrations of amlodipine are reached in 6-12 hours. Absolute bioavailability has been calculated as between 64% and 80%. Amlodipine bioavailability is unaffected by food ingestion.
Distribution: Telmisartan is largely bound to plasma protein (> 99.5 %), mainly albumin and alpha-1 acid glycoprotein. The mean steady state apparent volume of distribution (Vss) is approximately 500 L.
The volume of distribution of amlodipine is approximately 21 L/kg. In vitro studies with amlodipine have shown that approximately 97.5% of circulating drug is bound to plasma proteins in hypertensive patients.
Biotransformation: Telmisartan is metabolised by conjugation to the glucuronide of the parent compound. No pharmacological activity has been shown for the conjugate.
Amlodipine is extensively (approximatively 90%) metabolised by the liver to inactive metabolites.
Elimination: Telmisartan is characterised by biexponential decay pharmacokinetics with a terminal elimination half-life of > 20 hours.
After oral (and intravenous) administration telmisartan is nearly exclusively excreted with the faeces, exclusively as unchanged compound. Cumulative urinary excretion is < 2% of dose. Total plasma clearance (CL
tot) is high (approximately 900 ml/min compared with hepatic blood flow (about 1500 mL/min).
Amlodipine elimination from plasma is biphasic, with a terminal elimination half-life of approximately 30 to 50 hours. Steady-state plasma levels are reached after continuous administration for 7-8 days. Ten percent of original amlodipine and 60% of amlodipine metabolites are excreted in urine.
Linearity: The maximum plasma concentration (C
max) and, to a smaller extent, area under the plasma concentration-time curve (AUC) increase disproportionately with dose. There is no evidence of clinically relevant accumulation of telmisartan.
PK in Specific Populations:
Paediatric population (age below 18 years): No pharmacokinetic data for TWYNSTA are available in the paediatric population.
Gender differences: Gender differences in plasma concentrations of telmisartan were observed, C
max and AUC being approximately 3- and 2-fold higher, respectively, in females compared to males without relevant influence on efficacy.
Geriatric patients: The pharmacokinetics of telmisartan do not differ between younger and geriatric patients.
Time to peak plasma amlodipine concentrations is similar in young and elderly patients. In elderly patients, amlodipine clearance tends to decline, causing increases in the area under the curve (AUC) and elimination half-life.
Renal impairment: Lower plasma concentrations of telmisartan were observed in patients with renal insufficiency undergoing dialysis. Telmisartan is highly bound to plasma protein in renal-insufficient subjects and cannot be removed by dialysis. The elimination half-life is not changed in patients with renal impairment.
The pharmacokinetics of amlodipine are not significantly influenced by renal impairment.
Hepatic impairment: Pharmacokinetic studies in patients with hepatic impairment showed an increase in absolute bioavailability of telmisartan up to nearly 100%. The elimination half-life is not changed in patients with hepatic impairment.
Patients with hepatic insufficiency have decreased clearance of amlodipine with resulting increase of approximately 40-60% in AUC.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image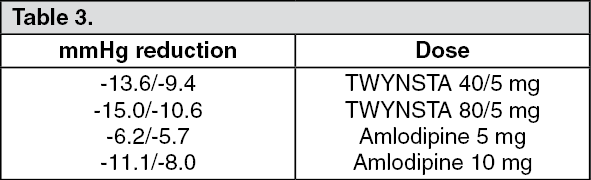 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
