Route of administration: Intravenous, as bolus injection or infusion.
Induction of General Anaesthesia: Adults: In unpremedicated and premedicated patients, it is recommended that propofol should be titrated (approximately 4 ml [40 mg] every 10 seconds in an average healthy adult by bolus injection or infusion) against the response of the patient until the clinical signs show the onset of anaesthesia. Most adult patients aged less than 55 years are likely to require 1.5 to 2.5 mg/kg of propofol. The total dose required can be reduced by lower rates of administration (2 to 5 ml/min [20 to 50 mg/min]). Over this age, the requirement will generally be less. In patients of ASA Grades 3 and 4, lower rates of administration should be used (approximately 2 ml [20 mg] every 10 seconds).
Elderly Patients: In elderly patients, the dose requirement for induction of anaesthesia with propofol is reduced. The reduction should take into account of the physical status and age of the patient. The reduced dose should be given at a slower rate and titrated against the response.
Children: Propofol is not recommended for induction of anaesthesia in children aged less than 1 month.
When used to induce anaesthesia in children, it is recommended that propofol be given slowly until the clinical signs show the onset of anaesthesia. The dose should be adjusted for age and/or weight. Most patients over 8 years of age are likely to require approximately 2.5 mg/kg of propofol for induction of anaesthesia. Under this age the requirement may be more. Lower dosage is recommended for children of ASA grades 3 and 4.
Maintenance of General Anaesthesia: Adults: Anaesthesia can be maintained by administering propofol either by continuous infusion or by repeat bolus injections to prevent the clinical signs of light anaesthesia. Recovery from anaesthesia is typically rapid and it is therefore important to maintain propofol administration until the end of the procedure.
Continuous Infusion: The required rate of administration varies considerably between patients, but rates in the region of 4 to 12 mg/kg/h usually maintain satisfactory anesthesia.
Repeat Bolus Injections: If a technique involving repeat bolus injections is used, increments of 25 mg (2.5 ml) to 50 mg (5.0 ml) may be given according to clinical need.
Elderly Patients: When propofol is used for maintenance of anaesthesia the rate of infusion or 'target concentration' should also be reduced. Patients of ASA grades 3 and 4 will require further reductions in dose and dose rate. Rapid bolus administration (single or repeated) should not be used in the elderly as this may lead to cardiorespiratory depression.
Children: Propofol is not recommended for maintenance of anaesthesia in children less than 1 month old.
Anaesthesia can be maintained by administering propofol by infusion or repeat bolus injection to prevent the clinical signs of light anaesthesia. The required rate of administration varies considerably between patients, but rates in the region of 9 to 15 mg/kg/h usually achieve satisfactory anaesthesia. Younger children, less than 3 years, may have higher dosage requirements within the range of recommended dosages, as compared with older paediatric patients. Dosage should be adjusted individually and particular attention paid to the need for adequate analgesia. A maximum duration of use of approximately 60 minutes should not be exceeded except where there is a specific indication for longer use e.g. malignant hyperthermia where volatile agents must be avoided.
Sedation during Intensive Care: Adults: For sedation during intensive care it is advised that propofol should be administered by continuous infusion. The infusion rate should be determined by the desired depth of sedation. In most patients sufficient sedation can be obtained with a dosage of 0.3 - 4 mg/kg/h of propofol. Propofol is not indicated for sedation in intensive care of patients of 16 years of age or younger.
Propofol may be diluted with 5% Dextrose.
It is recommended that blood lipid levels be monitored should propofol be administered to patients thought to be at particular risk of fat overload. If the duration of sedation is in excess of 3 days, lipids should be monitored in all patients.
Elderly Patients: When propofol is used for sedation the rate of infusion should also be reduced. Patients of ASA grades 3 and 4 will require further reductions in dose and dose rate. Rapid bolus administration (single or repeated) should not be used in the elderly as this may lead to cardiorespiratory depression.
Children: Propofol is contraindicated for the sedation of ventilated children aged 16 years or younger receiving intensive care.
Sedation for Surgical and Diagnostic Procedures: Adults: To provide sedation for surgical and diagnostic procedures, rates of administration should be individualized and titrated to clinical response. Most patients will require 0.5 to 1 mg/kg over 1 to 5 minutes for onset of sedation.
Maintenance of sedation may be accomplished by titrating propofol infusion to the desired level of sedation - most patients will require 1.5 to 4.5 mg/kg/h. In addition to the infusion, bolus administration of 10 to 20 mg may be used if a rapid increase in the depth of sedation is required. In patients of ASA Grades 3 and 4 the rate of administration and dosage may need to be reduced.
Elderly Patients: When propofol is used for sedation the rate of infusion or 'target concentration' should also be reduced. Patients of ASA grades 3 and 4 will require further reductions in dose and dose rate. Rapid bolus administration (single or repeated) should not be used in the elderly as this may lead to cardiorespiratory depression.
Children: Propofol is not recommended for sedation in children as safety and efficacy have not been demonstrated.
Administration: Propofol has no analgesic properties and therefore supplementary analgesic agents are generally required in addition to propofol.
Propofol can be used for infusion undiluted or diluted with 5% Dextrose (Intravenous Infusion BP) only, in PVC infusion bags or glass infusion bottles. Dilutions, which must not exceed 1 in 5 (2 mg propofol per ml) should be prepared aseptically immediately before administration and must be used within 6 hours of preparation.
It is recommended that, when using diluted propofol, the volume of 5% Dextrose removed from the infusion bag during the dilution process is totally replaced in volume by propofol emulsion.
The dilution may be used with a variety of infusion control techniques, but a giving set used alone will not avoid the risk of accidental uncontrolled infusion of large volumes of diluted propofol. A burette, drop counter or volumetric pump must be included in the infusion line. The risk of uncontrolled infusion must be taken into account when deciding the maximum amount of propofol in the burette.
When propofol is used undiluted to maintain anaesthesia, it is recommended that equipment such as syringe pumps or volumetric infusion pumps should always be used to control infusion rates.
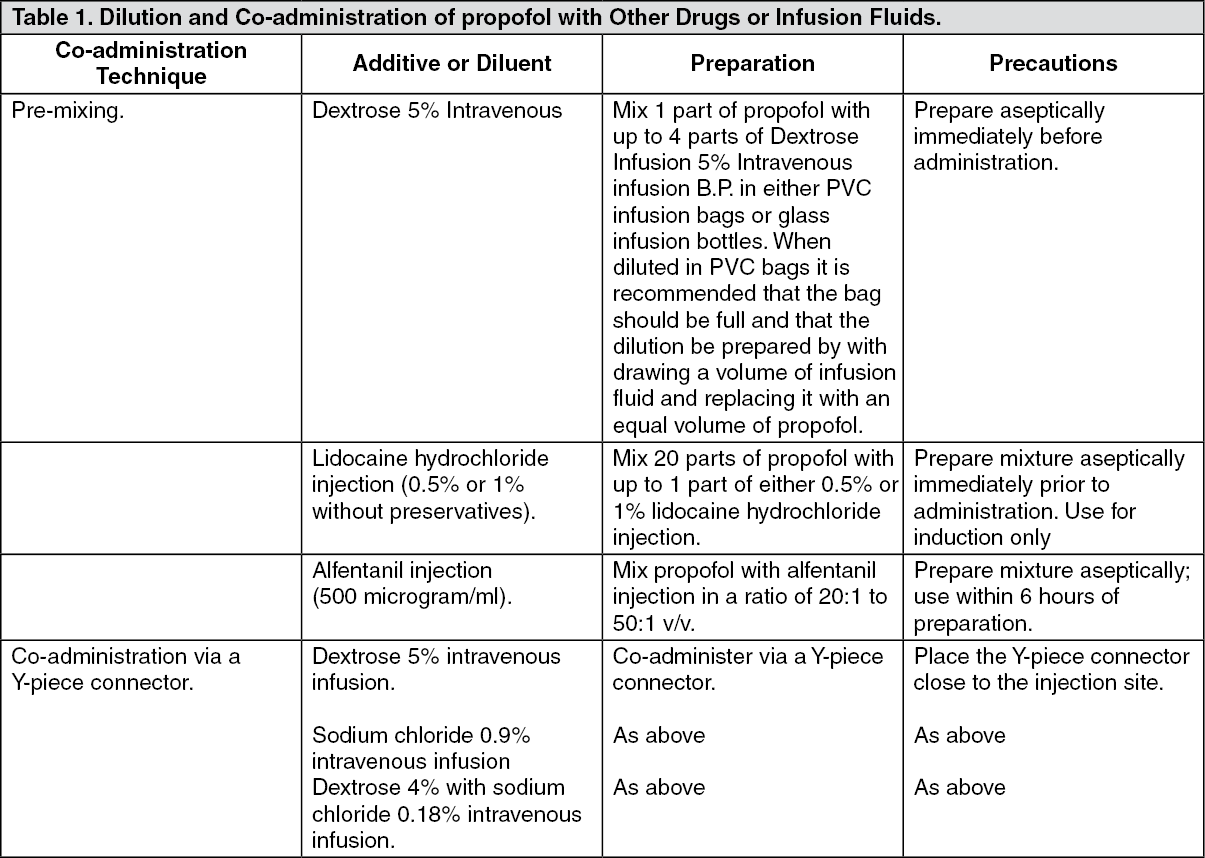
Propofol may be administered via a Y-piece close to the injection site into infusions of the following: Dextrose 5% Intravenous Infusion B.P.; Sodium Chloride 0.9% Intravenous Infusion B.P.; Dextrose 4% with Sodium Chloride 0.18% Intravenous Infusion B.P.
Propofol may be premixed with alfentanil injection containing 500 micrograms/ml alfentanil in the ratio of 20:1 to 50:1 v/v. Mixtures should be prepared using sterile technique and used within 6 hours of preparation.
In order to reduce pain on initial injection, Propofol may be mixed with preservative-free Lidocaine Injection 0.5% or 1%. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
