Fluocinolone acetonide 0.01%, hydroquinone 4%, tretinoin 0.05%.
Each gram of TRI-LUMA Cream contains Active: fluocinolone acetonide 0.01 % (0.1 mg), hydroquinone 4% (40 mg), and tretinoin 0.05% (0.5 mg).
TRI-LUMA Cream (fluocinolone acetonide 0.01%, hydroquinone 4%, tretinoin 0.05%) contains fluocinolone acetonide, USP, hydroquinone, USP, and tretinoin, USP, in a hydrophilic cream base for topical application.
Fluocinolone acetonide is a synthetic fluorinated corticosteroid for topical dermatological use and is classified therapeutically as an anti-inflammatory. It is a white crystalline powder that is odourless and stable in light.
The chemical name for fluocinolone acetonide is: (6α-,11β,16α)-6,9-difluoro-11,21-dihydroxy-16,17-[(1-methylethylidene)bis(oxy)]-pregna-1,-4-diene-3,20-dione.
The molecular formula is C24H30F2O6 and molecular weight is 452.50.
Hydroquinone is classified therapeutically as a depigmenting agent. It is prepared from the reduction of p-benzoquinone with sodium bisulfite. It occurs as fine white needles that darken on exposure to air.
The chemical name for hydroquinone is: 1,4-benzenediol.
The molecular formula is C6H6O2 and molecular weight is 110.11.
Tretinoin is all-trans-retinoic acid formed from the oxidation of the aldehyde group of retinene to a carboxyl group. It occurs as yellow to light-orange crystals or crystalline powder with a characteristic odor of ensilage. It is highly reactive to light and moisture and should be stored at a cool temperature. Tretinoin is classified therapeutically as a keratolytic. The chemical name for tretinoin is: (all-E)-3,7-dimethyl-9-(2,6,6-trimethyl-1-cyclohexen-1-yl)-2,4,6,8-nonatetraenoic acid.
The molecular formula is C20H28O2 and molecular weight is 300.44.
Excipients/Inactive Ingredients: butylated hydroxytoluene, cetyl alcohol, citric acid, glycerin, magnesium aluminum silicate, methyl gluceth-10, methyl-paraben , Arlacel 165, propylparaben 0.02% (0.2mg), purified water, sodium metabisulfite, stearic acid, and stearyl alcohol.
Pharmacology: Pharmacodynamics: One of the components in TRI-LUMA Cream, hydroquinone, is a depigmenting agent, and may interrupt one or more steps in the tyrosine-tyrosinase pathway of melanin synthesis. However, the mechanism of action of the active ingredients in TRI-LUMA Cream in the treatment of melasma is unknown.
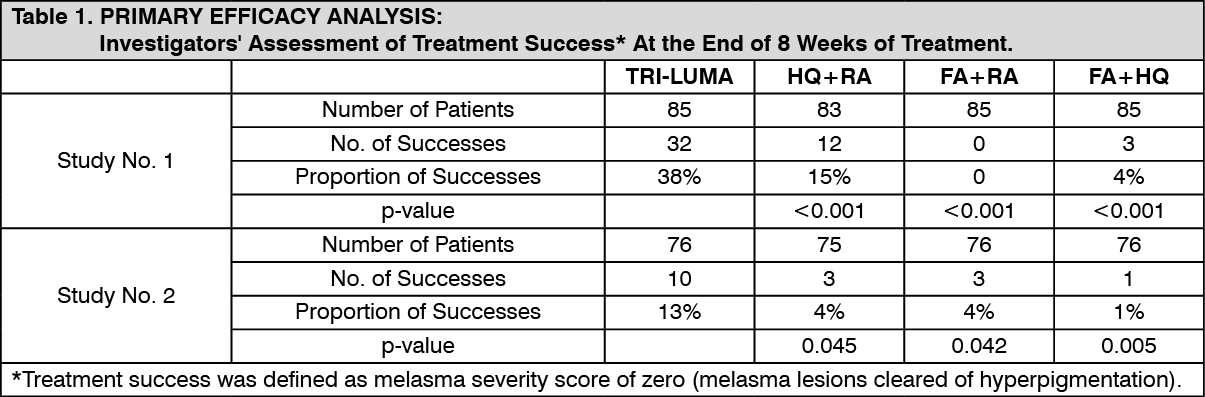
Clinical Studies: Two adequate and well-controlled efficacy and safety studies were conducted in 641 patients between the ages of 21 to 75 years, having skin phototypes I-IV and moderate to severe melasma of the face. TRI-LUMA Cream was compared with the 3 possible combinations of 2 of the 3 active ingredients [(1) hydroquinone 4% (HQ) + tretinoin 0.05% (RA); (2) fluocinolone acetonide 0.01% (FA) + tretinoin 0.05% (RA); (3) fluocinolone acetonide 0.01% (FA) + hydroquinone 4% (HQ)], contained in the same vehicle as TRI-LUMA Cream. Patients were instructed to apply their study medication each night, after washing their face with a mild soapless cleanser, for 8 weeks. Instructions were given to apply a thin layer
of study medication to the hyperpigmented lesion, making sure to cover the entire lesion including the outside borders extending to the normal pigmented skin. Patients were provided a mild moisturizer for use as needed. A sunscreen with SPF 30 was also provided with instructions for daily use. Protective clothing and avoidance of sunlight exposure to the face was recommended. Patients were evaluated for melasma severity at Baseline and at Weeks 1 ,2, 4, and 8 of treatment. Primary efficacy was based on the proportion of patients who had an investigators' assessment of treatment success, defined as the clearing of melasma at the end of the eight-week treatment period. The majority of patients enrolled in the two studies were white (approximately 66%) and female (approximately 98%). TRILUMA Cream was demonstrated to be significantly more effective than any of the other combinations of the active ingredients. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
p-value is from Cochran-Mantel-Haenszel chi-square statistics controlling for pooled investigator and comparing TRI-LUMA Cream to the other treatment groups. In the Investigators' assessment of melasma severity at Day 56 of treatment, the following table shows the clinical improvement profile for all patients treated with TRI-LUMA Cream based on severity of their melasma at the start of treatment. (See Table 2.)
Click on icon to see table/diagram/image
Assessment Scale: Cleared (melasma lesions approximately equivalent to surrounding normal skin or with minimal residual hyper-pigmentation); Mild (slightly darker than the surrounding normal skin); Moderate (moderately darker than the surrounding normal skin); Severe (markedly darker than the surrounding normal skin). Patients experienced improvement of their melasma with the use of TRI-LUMA Cream as early as 4 weeks. However, among 7 patients who had clearing at the end of 4 weeks of treatment with TRI-LUMA Cream, 4 of them did not maintain the remission after an additional 4 weeks of treatment.
After 8 weeks of treatment with the study drug, patients entered into an open-label extension period in which TRI-LUMA Cream was given on an as-needed basis for the treatment of melasma. The remission periods appeared to shorten between progressive courses of treatment. Additionally, few patients maintained complete clearing of melasma (approximately 1 to 2%).
Pharmacokinetics: Percutaneous absorption of unchanged tretinoin, hydroquinone and fluocinolone acetonide into the systemic circulation of two groups of healthy volunteers (Total n = 59) was found to be minimal following 8 weeks of daily application of 1g (Group I, n = 45) or 6g (Group II, n = 14) of TRI-LUMA Cream.
For tretinoin, quantifiable plasma concentrations were obtained in 57.78% (26 out of 45) of Group I and 57.14% (8 out of 14) of Group II subjects. The exposure to tretinoin as reflected by the C
max values ranged from 2.01 to 5.34 ng/mL (Group I) and 2.0 to 4.99 ng/mL (Group II). Thus, daily application of TRI-LUMA Cream resulted in a minimal increase of normal endogenous levels of tretinoin. The circulating tretinoin levels represent only a portion of total tretinoin-associated retinoids, which would include metabolites of tretinoin and that sequestered into peripheral tissues.
For hydroquinone, quantifiable plasma concentrations were obtained in 18% (8 out of 44) Group I subjects. The exposure to hydroquinone as reflected by the C
max values ranged from 25.55 to 86.52 ng/mL. All Group II subjects (6g dose) had post-dose plasma hydroquinone concentrations below the quantitation limit. For Fluocinolone acetonide, Groups I and II subjects had all post-dose plasma concentrations below quantitation limit.
TRI-LUMA cream short-term treatment of moderate to severe melasma of the face, in the
presence of measures for sun avoidance, including the use of sunscreens.
The following are important statements relating to the indication and usage of TRI-LUMA Cream: TRI-LUMA cream, a combination drug product containing corticosteroid, retinoid, and bleaching agent, was proven safe for the intermittent treatment of melasma, with cumulative treatment time of at least 180 days. Because melasma usually recurs upon discontinuation of TRI-LUMA Cream, patients can be re-treated with TRI-LUMA until melasma is resolved. Patients need to avoid sunlight exposure, use sunscreen with appropriate SPF, wear protective clothing, and change to non-hormonal forms of birth control, if hormonal methods are used.
In clinical trials used to support the use of TRI-LUMA Cream in the treatment of melasma, patients were instructed to avoid sunlight exposure to the face, wear protective clothing and use a sunscreen with SPF 30 each day. They were to apply the study medication each night, after washing their face with a mild soapless cleanser.
The safety and efficacy of TRI-LUMA Cream in patients of skin types V and VI have not been studied. Excessive bleaching resulting in undesirable cosmetic effect in patients with darker skin cannot be excluded.
The safety and efficacy of TRI-LUMA Cream in the treatment of hyperpigmentation conditions other than melasma of the face have not been studied.
Because pregnant and lactating women were excluded from, and women of child-bearing potential had to use birth control measures in the clinical trials, the safety and efficacy of TRI-LUMA Cream in pregnant women and nursing mothers have not been established. Therefore, it is not recommended for use in pregnant women. (See Use in Pregnancy under PRECAUTIONS).
TRI-LUMA Cream should be applied once daily at night. It should be applied at least 30 minutes before bedtime.
Gently wash the face and neck with a mild cleanser. Rinse and pat the skin dry. Apply a thin film of the cream to the hyperpigmented areas of melasma including about ½ inch of normal appearing skin surrounding each lesion. Rub lightly and uniformly into the skin. Do not use occlusive dressing.
During the day, use a sunscreen of SPF 30, and wear protective clothing. Avoid excessive sunlight exposure. Patients may use moisturizers and/or cosmetics during the day.
Therapeutic effects may be observed as early as 4 weeks. Treatment should be discontinued when melasma is resolved.
When melasma recurs, treat with TRI-LUMA Cream until the condition clears.
If excessive marked redness, peeling, or discomfort occurs at the application site, TRI-LUMA should be used less frequently or discontinued altogether. This will not have any systemic consequence as the percutaneous absorption of the active ingredients in Tri-Luma into the systemic circulation in healthy volunteers (N=59) was to be found minimal following 8 weeks of daily application of 1g or 6g of Tri-Luma. A symptomatic treatment might be prescribed as appropriate.
TRI-LUMA Cream is contraindicated in individuals with a history of hypersensitivity, allergy, or intolerance to this product or any of its components, in pregnancy, and in women planning a pregnancy.
TRI-LUMA Cream contains sodium metabisulfite, a sulfite that may cause allergic-type reactions including anaphylactic symptoms and life-threatening asthmatic episodes in susceptible people.
TRI-LUMA Cream contains hydroquinone, which may produce exogenous ochronosis, a gradual blue-black darkening of the skin, whose occurrence should prompt discontinuation of therapy. The majority of patients developing this condition are Black, but it may also occur in Caucasians and Hispanics.
Cutaneous hypersensitivity to the active ingredients of TRI-LUMA Cream has been reported in the literature. In a patch test study to determine sensitization potential in 221 healthy volunteers, three volunteers developed sensitivity reactions to TRI-LUMA Cream or its components.
General: TRI-LUMA Cream contains hydroquinone and tretinoin that may cause mild to moderate irritation. Local irritation, such as skin reddening, peeling, mild burning sensation, dryness, and pruritus may be expected at the site of application. Transient skin reddening or mild burning sensation does not preclude treatment. If a reaction suggests hypersensitivity or chemical irritation, the use of the medication should be discontinued.
TRI-LUMA Cream also contains the corticosteroid fluocinolone acetonide. Systemic absorption of topical corticosteroids can produce reversible hypothalamic-pituitary-adrenal (HPA) axis suppression with the potential for glucocorticosteroid insufficiency after withdrawal of treatment. Manifestations of Cushing's syndrome, hyperglycemia, and glucosuria can also be produced by systemic absorption of topical corticosteroid while on treatment. If HPA axis suppression is noted, the use of TRI-LUMA Cream should be discontinued. Recovery of HPA axis function generally occurs upon discontinuation of topical corticosteroids.
Visual disturbance may be reported with systemic and topical corticosteroid use. If a patient presents with symptoms such as blurred vision or other visual disturbances, the patient should be considered for referral to an ophthalmologist for evaluation of possible causes, which may include cataract, glaucoma or rare diseases such as central serous chorioretinopathy (CSCR) which have been reported after use of systemic and topical corticosteroids.
Information for Patients: Exposure to sunlight, sunlamp, or ultraviolet light should be avoided. Patients who are consistently exposed to sunlight or skin irritants either through their work environment or habits should exercise particular caution. Sunscreen and protective covering (such as the use of a hat) over the treated areas should be used. Sunscreen use is an essential aspect of melasma therapy, as even minimal sunlight sustains melanocytic activity.
Weather extremes, such as heat or cold, may be irritating to patients treated with TRI-LUMA Cream. Because of the drying effect of this medication, a moisturizer may be applied to the face in the morning after washing.
Application of TRI-LUMA Cream should be kept away from the eyes, nose, or angles of the mouth, because the mucosa is much more sensitive than the skin to the irritant effect. If local irritation persists or becomes severe, application of the medication should be discontinued, and the health care provider consulted. Allergic contact dermatitis, blistering, crusting, and severe burning or swelling of the skin and irritation of the mucous membranes of the eyes, nose, and mouth require medical attention. If the medication is applied excessively, marked redness, peeling, or discomfort may occur.
This medication is to be used as directed by the health care provider and should not be used for any disorder other than that for which it is prescribed.
Laboratory Tests: The following tests may be helpful in evaluating patients for HPA axis suppression: ACTH or cosyntropin stimulation test, A.M. plasma cortisol test, Urinary free cortisol test.
Carcinogenesis, Mutagenesis, Impairment of Fertility: Long-term animal studies to determine the carcinogenic potential of TRI-LUMA Cream have not been conducted. Studies of hydroquinone in animals have demonstrated some evidence of carcinogenicity. The carcinogenic potential of hydroquinone in humans is unknown. Studies in hairless albino mice suggest that concurrent exposure to tretinoin may enhance the tumorigenic potential of carcinogenic doses of UVB and UVA light from a solar simulator. This effect has been confirmed in a later study in pigmented mice, and dark pigmentation did not overcome the enhancement of photocarcinogenesis by 0.05% tretinoin. Although the significance of these studies to humans is not clear, patients should minimize exposure to sunlight or artificial ultraviolet irradiation sources. Mutagenicity studies were not conducted with this combination of active ingredients. Published studies have demonstrated that hydroquinone is a mutagen and a clastogen. Treatment with hydroquinone has resulted in positive findings for genetic toxicity in the Ames assay in bacterial strains sensitive to oxidizing mutagens, in in vitro studies in mammalian cells, and in the in vivo mouse micronucleus assay. Tretinoin has been shown to be negative for mutagenesis in the Ames assay. Additional information regarding the genetic toxicity potential of tretinoin and of fluocinolone acetonide is not available.
A dermal reproductive fertility study was conducted in SD rats using a 10-fold dilution of the clinical formulation. No effect was seen on the traditional parameters used to assess fertility, although prolongation of estrus was observed in some females, and there was a trend towards an increase in pre- and post-implantation loss that was not statistically significant.
No adequate study of fertility and early embryonic toxicity of the full-strength drug product has been pertormed. In a six-month study in minipigs, small testes and severe hypospermia were found when males were treated topically with the full strength drug product.
Use in Pregnancy: Teratogenic Effects: TRI-LUMA Cream contains the teratogen, tretinoin, which may cause embryo-fetal death, altered fetal growth, congenital malformations, and potential neurologic deficits. It is difficult to interpret the animal studies on teratogenicity with TRI-LUMA Cream, because the availability of the dermal applications in these studies cannot be assured, and comparison with clinical dosing is not possible. There are no adequate and well-controlled studies in pregnant women. Orally administered retinoids have been associated with congenital abnormalities. When used in accordance with the prescribing information, topically administered retinoids are generally assumed to result in low systemic exposure due to minimal dermal absorption. However, there could be individual factors (e.g. damaged skin barrier, excessive use) that contribute to an increased systemic exposure. TRI-LUMA is contraindicated in pregnancy, or in women planning a pregnancy. If the product is used during pregnancy, or if the patient becomes pregnant while taking this drug, treatment should be discontinued.
Clinical considerations relevant to actual or potential inadvertent exposure during pregnancy: In clinical trials involving TRI-LUMA Cream in the treatment of facial melasma, women of child-bearing potential initiated treatment only after having had a negative pregnancy test and used effective birth control measures during therapy. Thus, safety and efficacy of TRI-LUMA Cream in pregnancy has not been established. In general, use of drugs should be reduced to a minimum in pregnancy. If a patient has been inadvertently exposed to TRI-LUMA Cream in pregnancy, she should be counseled on the risk of teratogenesis due to this exposure. The risk of teratogenesis due to topical exposure to TRI-LUMA Cream may be considered low. However, exposure during the period of organogenesis in the first trimester is theoretically more likely to produce adverse outcome than in later pregnancy.
The prescriber should have the following clinical considerations in making prescribing decisions: The potential developmental effects of tretinoin are serious but the risk from topical administration is small.
Exposure during the period for organogenesis in the first trimester is theoretically more likely to produce adverse outcome than in later pregnancy.
The risk to the mother for not treating melasma should be determined by the physician with the patient. Mild forms of melasma may not necessarily require drug treatment. TRI-LUMA Cream is indicated for the treatment of moderate to severe melasma. Melasma may also be managed with other forms of therapy such as topical hydroquinone in the presence of sunlight avoidance, or stopping the use of hormonal birth control methods. If possible, delaying treatment with TRI-LUMA Cream until after delivery should be considered.
There are no adequate and well-controlled studies in pregnant women. Therefore, the use of TRI-LUMA in pregnant women is not recommended.
Data Discussion: Tretinoin is considered to be highly teratogenic upon systemic administration. Animal reproductive studies are not available with topical hydroquinone. Corticosteroids have been shown to be teratogenic in laboratory animals when administered systemically at relatively low dosage levels. Some corticosteroids have been shown to be teratogenic after dermal application in laboratory animals.
Human Data: In clinical trials involving TRI-LUMA Cream in the treatment of facial melasma, women of child-bearing potential initiated treatment only after having had a negative pregnancy test, and used effective birth control measures during therapy. However, 15 women became pregnant during treatment with TRI-LUMA Cream. Of these pregnancies, 6 resulted in healthy babies, 6 outcomes still unknown, 2 were reported as miscarriages, and 1 case was lost to follow-up.
Epidemiologic studies have not confirmed an increase in birth defects associated with the use of topical tretinoin. However, there may be limitations to the sensitivity of epidemiologic studies in the detection of certain forms of fetal injury, such as subtle neurologic or intelligence deficits.
Animal Data: In a dermal application study using TRI-LUMA Cream in pregnant rabbits, there was an increase in the number of in utero deaths and a decrease in fetal weights in litters from dams treated topically with the drug product.
In a dermal application study in pregnant rats treated with TRI-LUMA Cream during organogenesis there was evidence of teratogenicity of the type expected with tretinoin. These morphological alterations included cleft palate, protruding tongue, open eyes, umbilical hernia, and retinal folding or dysplasia.
In a dermal application study on the gestational and postnatal effects of a 10-fold dilution of TRI-LUMA Cream in rats, an increase in the number of stillborn pups, lower pup body weights, and delay in preputial separation were observed. An increase in overall activity was seen in some treated litters at postnatal day 22 and in all treated litters at five weeks, a pattern consistent with effects previously noted in animals exposed in utero with retinoic acids. No adequate study of the late gestational and postnatal effects of the full-strength TRI-LUMA Cream has been performed.
It is difficult to interpret these animal studies on teratogenicity with TRI-LUMA Cream, because the availability of the dermal applications in these studies cannot be assured, and comparison with clinical dosing is not possible.
All pregnancies have a risk of birth defect, loss, or other adverse event regardless of drug exposure. Typically, estimates of increased fetal risk from drug exposure rely heavily on animal data. However, animal studies do not always predict effects in humans. Even if human data are available, such data may not be sufficient to determine whether there is an increased risk to the fetus. Drug effects on behavior, cognitive function, and fertility in the offspring are particularly difficult to assess.
Use in Lactation: Corticosteroids, when systemically administered, appear in human milk. It is not known whether topical application of TRI-LUMA Cream could result in sufficient systemic absorption to produce detectable quantities of fluocinolone acetonide, hydroquinone, or tretinoin in human milk. Because many drugs are secreted in human milk, caution should be exercised when TRI-LUMA Cream is administered to a nursing woman. Care should be taken to avoid contact between the infant being nursed and TRI-LUMA Cream.
Use in Children: Safety and effectiveness of TRI-LUMA Cream in pediatric patients have not been established.
Use in the Elderly: Clinical studies of TRI-LUMA Cream did not include sufficient number of subjects aged 65 and over to determine whether they respond differently from younger subjects. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal or cardiac function, and of concomitant disease or other drug therapy.
Pregnancy: Teratogenic Effects: TRI-LUMA Cream contains the teratogen, tretinoin, which may cause embryo-fetal death, altered fetal growth, congenital malformations, and potential neurologic deficits. It is difficult to interpret the animal studies on teratogenicity with TRI-LUMA Cream, because the availability of the dermal applications in these studies cannot be assured, and comparison with clinical dosing is not possible. There are no adequate and well-controlled studies in pregnant women. Orally administered retinoids have been associated with congenital abnormalities. When used in accordance with the prescribing information, topically administered retinoids are generally assumed to result in low systemic exposure due to minimal dermal absorption. However, there could be individual factors (e.g. damaged skin barrier, excessive use) that contribute to an increased systemic exposure. TRI-LUMA is contraindicated in pregnancy, or in women planning a pregnancy. If the product is used during pregnancy, or if the patient becomes pregnant while taking this drug, treatment should be discontinued.
Clinical considerations relevant to actual or potential inadvertent exposure during pregnancy: In clinical trials involving TRI-LUMA Cream in the treatment of facial melasma, women of child-bearing potential initiated treatment only after having had a negative pregnancy test and used effective birth control measures during therapy. Thus, safety and efficacy of TRI-LUMA Cream in pregnancy has not been established. In general, use of drugs should be reduced to a minimum in pregnancy. If a patient has been inadvertently exposed to TRI-LUMA Cream in pregnancy, she should be counseled on the risk of teratogenesis due to this exposure. The risk of teratogenesis due to topical exposure to TRI-LUMA Cream may be considered low. However, exposure during the period of organogenesis in the first trimester is theoretically more likely to produce adverse outcome than in later pregnancy.
The prescriber should have the following clinical considerations in making prescribing decisions: The potential developmental effects of tretinoin are serious but the risk from topical administration is small.
Exposure during the period for organogenesis in the first trimester is theoretically more likely to produce adverse outcome than in later pregnancy.
The risk to the mother for not treating melasma should be determined by the physician with the patient. Mild forms of melasma may not necessarily require drug treatment. TRI-LUMA Cream is indicated for the treatment of moderate to severe melasma. Melasma may also be managed with other forms of therapy such as topical hydroquinone in the presence of sunlight avoidance, or stopping the use of hormonal birth control methods. If possible, delaying treatment with TRI-LUMA Cream until after delivery should be considered.
There are no adequate and well-controlled studies in pregnant women therefore, the use of TRI-LUMA in pregnant women is not recommended.
Data Discussion: Tretinoin is considered to be highly teratogenic upon systemic administration. Animal reproductive studies are not available with topical hydroquinone. Corticosteroids have been shown to be teratogenic in laboratory animals when administered systemically at relatively low dosage levels. Some corticosteroids have been shown to be teratogenic after dermal application in laboratory animals.
Human Data: In clinical trials involving TRI-LUMA Cream in the treatment of facial melasma, women of child-bearing potential initiated treatment only after having had a negative pregnancy test, and used effective birth control measures during therapy. However, 15 women became pregnant during treatment with TRI-LUMA Cream. Of these pregnancies, 6 resulted in healthy babies, 6 outcomes still unknown, 2 were reported as miscarriages, and 1 case was lost to follow-up.
Epidemiologic studies have not confirmed an increase in birth defects associated with the use of topical tretinoin. However, there may be limitations to the sensitivity of epidemiologic studies in the detection of certain forms of fetal injury, such as subtle neurologic or intelligence deficits.
Animal Data: In a dermal application study using TRI-LUMA Cream in pregnant rabbits, there was an increase in the number of in utero deaths and a decrease in fetal weights in litters from dams treated topically with the drug product.
In a dermal application study in pregnant rats treated with TRI-LUMA Cream during organogenesis there was evidence of teratogenicity of the type expected with tretinoin. These morphological alterations included cleft palate, protruding tongue, open eyes, umbilical hernia, and retinal folding or dysplasia.
In a dermal application study on the gestational and postnatal effects of a 10-fold dilution of TRI-LUMA Cream in rats, an increase in the number of stillborn pups, lower pup body weights, and delay in preputial separation were observed. An increase in overall activity was seen in some treated litters at postnatal day 22 and in all treated litters at five weeks, a pattern consistent with effects previously noted in animals exposed in utero with retinoic acids. No adequate study of the late gestational and postnatal effects of the full-strength TRI-LUMA Cream has been performed.
It is difficult to interpret these animal studies on teratogenicity with TRI-LUMA Cream, because the availability of the dermal applications in these studies cannot be assured, and comparison with clinical dosing is not possible.
All pregnancies have a risk of birth defect, loss, or other adverse event regardless of drug exposure. Typically, estimates of increased fetal risk from drug exposure rely heavily on animal data. However, animal studies do not always predict effects in humans. Even if human data are available, such data may not be sufficient to determine whether there is an increased risk to the fetus. Drug effects on behavior, cognitive function, and fertility in the offspring are particularly difficult to assess.
Nursing Mothers: Corticosteroids, when systemically administered, appear in human milk. It is not known whether topical application of TRI-LUMA Cream could result in sufficient systemic absorption to produce detectable quantities of fluocinolone acetonide, hydroquinone, or tretinoin in human milk. Because many drugs are secreted in human milk, caution should be exercised when TRI-LUMA Cream is administered to a nursing woman. Care should be taken to avoid contact between the infant being nursed and TRI-LUMA Cream.
In the controlled clinical trials, adverse events were monitored in the 161 patients who used TRI-LUMA Cream once daily during an 8-week treatment period. There were 102 (63%) patients who experienced at least one treatment-related adverse event during these studies. In the long term clinical study, from a total of 314 patients treated with TRI-LUMA cream for at least 180 cumulative days, there were 202 (64%) patients who experienced at least one treatment-related adverse event No significant increase in severity or incidence of adverse events was observed from long-term use of TRI-LUMA cream compared with events reported during the 8-week controlled clinical studies. The most frequently reported adverse events that were observed from the controlled clinical trials and the long term safety were erythema,
desquamation, and burning at the site of application. The number and percentages of these events were markedly lower in the long-term study than in the controlled clinical studies. The majority of these events were mild to moderate in severity.
Adverse events reported by at least 1% of patients and judged by the investigators to be reasonably related to treatment with TRI-LUMA Cream from the controlled clinical studies and the long-term study are summarized (in decreasing order of frequency). (See Tables 3 and 4.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The severity, incidence and type of adverse events experienced from 6 months cumulative use were not significantly different from the events reported for all patients. The incidence of application site pigmentation changes that occurred in both the controlled and long-term safety studies included 11 occurrences of hypopigmentation in 27 patients. The following local adverse reactions have been reported infrequently with topical corticosteroids. They may occur more frequently with the use of occlusive dressings, especially with higher potency corticosteroids. These reactions are listed in an approximate decreasing order of occurrence: burning, itching, irritation, dryness, folliculitis, acneiform eruptions, hypopigmentation,
perioral dermatitis, allergic contact dermatitis, secondary infection, skin atrophy, striae, miliaria, blurred vision. TRI-LUMA Cream contains hydroquinone, which may produce exogenous ochronosis, a gradual blue-black darkening of the skin whose occurrence should prompt discontinuation of therapy. Cutaneous hypersensitivity to the active ingredients of TRI-LUMA Cream has been reported in the literature. In a patch test study to determine sensitization potential in 221 healthy volunteers, three volunteers developed sensitivity reactions to TRI-LUMA Cream or its component.
Patient should avoid medicated or abrasive soaps and cleansers, soaps and cosmetics with drying effects, products with high concentration of alcohol and astringent and other irritants or keratolytic drugs while on TRI-LUMA Cream treatment. Patients are cautioned on concomitant use of medications that are known to be photosensitizing.
Keep tightly closed. Store in a refrigerator (2-8 °C). Protect from freezing.
D11AX - Other dermatologicals ; Used in the treatment of dermatological diseases.
Tri-Luma cream
15 g x 1's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image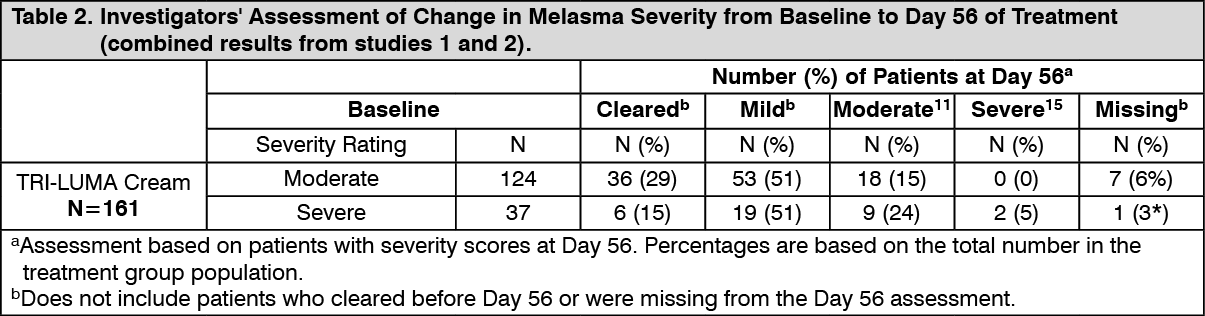 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image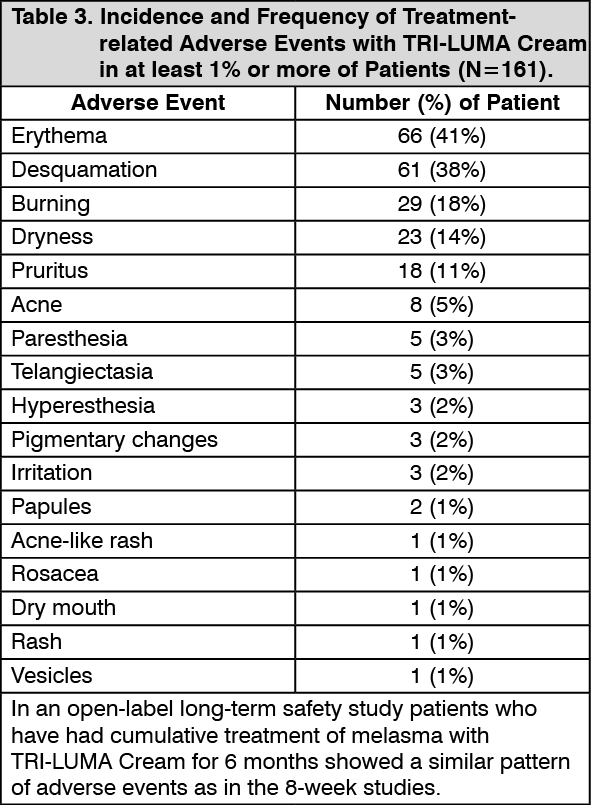 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image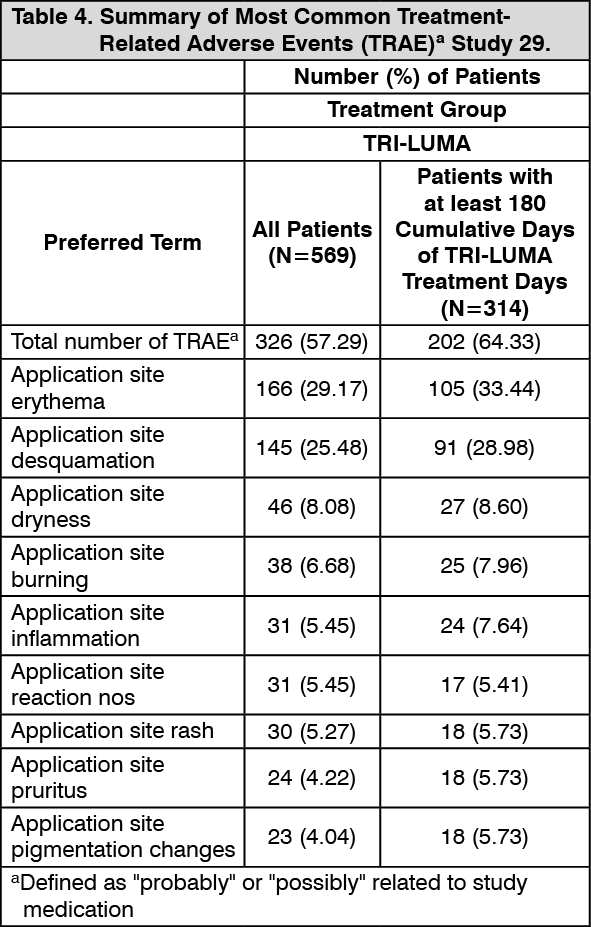 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
