Preparation for inhalation in form of inhalation solution. Sterile nebuliser suspension. White to off-white suspension in plastic single dose units.
Talgan Nebulizer suspension 0.5 mg/2 ml: Each ml nebuliser suspension contains 0.25 mg of Budesonide.
Talgan Nebulizer suspension 1 mg/2 ml: Each ml nebuliser suspension contains 0.50 mg of Budesonide.
Pharmacology: Pharmacodynamics: Budesonide is a glucocorticosteroid which possesses a high local anti-inflammatory action, with a lower incidence and severity of adverse effects than those seen with oral corticosteroids.
The precise mechanism of action of glucocorticosteroids in the treatment of asthma is not fully understood. Anti-inflammatory effects (including T-cells, eosinophilic cells and mast cells) such as inhibition of the release of inflammatory mediators and inhibition of cytokine-mediated immune response, are probably important. The strength of budesonide, measured as affinity for glucocorticoid receptors, is approximately 15 times stronger than that of prednisolone. Glucocorticoids reduce airway inflammation and thus reduce airway hyper-responsiveness to a variety of stimuli, as well as to effectively prevent exercise-induced asthma.
Regular treatment with glucocorticoids improves lung function, reduces the number of acute exacerbations and reduces surrogate markers of airway inflammation including decreased eosinophils in sputum and decreased exhaled NO.
The most important aspect of inhaled glucocorticoids is that they exert their effects locally and have much reduced systemic exposure thus reducing side effects substantially. Following inhalation the proportion of drug absorbed and which together with the swallowed fraction could resulted in undesired systemic effects, e.g. suppression of the hypothalamic-pituitary-adrenal (HPA) axis, osteoporosis and insulin sensitivity depends on the individual compound properties and metabolic liability.
Pharmacokinetics: Absorption: In adults the systemic availability of budesonide following administration of Talgan Inhalation Suspension via a jet nebuliser is approximately 15% of the nominal dose and 40% to 70% of the dose delivered to the patients. A minor fraction of the systemically available drug comes from swallowed drug. The maximal plasma concentration, occurring about 10 to 30 min after start of nebulisation is approximately 4 nmol/L after a single dose of 2 mg. Most of budesonide delivered to the lungs is systemically absorbed.
Distribution: Budesonide has a volume of distribution of approximately 3 L/kg. Plasma protein binding averages 85-90%.
Biotransformation: Budesonide is mainly eliminated by metabolism. Budesonide undergoes an extensive degree (~90%) of biotransformation on first passage through the liver to metabolites of low glucocorticosteroid activity. The glucocorticosteroid activity of the major metabolites, 6β-hydroxybudesonide and 16α-hydroxyprednisolone, is less than 1% of that of budesonide. The metabolism of budesonide is primarily mediated by CYP3A, a subfamily of cytochrome P450. Negligible metabolic inactivation has been observed in human lung and serum preparations.
Elimination: The metabolites of budesonide are excreted as such or in conjugated form mainly via the kidneys. No unchanged budesonide has been detected in the urine. Budesonide has high systemic clearance (approximately 1.2 L/min) in healthy adults, and the terminal half-life of budesonide after IV dosing averages 2-3 hours.
Linearity: The kinetics of budesonide are dose-proportional at clinically relevant doses.
Paediatric population: Budesonide has a systemic clearance of approximately 0.5 L/min in 4-6 years old asthmatic children. Per kg body weight children have a clearance which is approximately 50% greater than in adults. The terminal half-life of budesonide after inhalation is approximately 2.3 hours in asthmatic children. This is about the same as in healthy adults.
Talgan Nebulizer Suspension contains the potent non-halogenated corticosteroid, budesonide for use in bronchial asthma in patients where the use of a pressurised inhaler or dry powder formulation is unsatisfactory or inappropriate.
Recommended Dosage: BRONCHIAL ASTHMA: Talgan Nebulizer Suspension should be administered from a suitable nebuliser. The dose delivered to the patient varies between 40-60% of the nominal dose depending on the nebulising equipment used. The nebulisation time and the dose delivered are dependent on flow rate, volume of nebuliser chamber and volume fill. A suitable fill for most nebulisers is 2-4 mL.
Dosage initially, or during periods of severe asthma, or while reducing oral corticosteroids.
Adults: 1-2 mg twice daily.
Children: 0.5-1 mg twice daily.
Maintenance: The maintenance dose should be individualised and should be the lowest dose, which keeps the patient symptom-free. Recommended doses are: Adults 0.5-1 mg twice daily.
Children: 0.25-0.5 mg twice daily.
Patient Instructions: It is essential that the patient is instructed that Talgan is a preventative agent, which must be taken regularly and is not to be used as sole therapy to relieve an acute asthma attack.
The patient should be instructed in the proper use of the inhaler device considered appropriate for his/her particular needs. A full set of instructions are provided with each pack of Talgan.
Patients also receiving bronchodilators by inhalation should be advised to use the bronchodilator before Talgan in order to enhance its penetration into the bronchial tree. Several minutes should elapse between the uses of the two inhalers.
Clinical Management: Patients - not oral corticosteroid dependent: Treatment with the recommended doses of Talgan usually gives a therapeutic effect within 10 days.
In patients with excessive mucus secretion in the bronchi, an initial short course (about 2 weeks) of an oral corticosteroid, commencing with a high dose and gradually reducing, should be given in addition to Talgan. Treatment should be continued for at least one month before determining the maximal response to a given dose of Talgan.
Patients - oral corticosteroid dependent: Transfer of patients dependent on oral corticosteroids to Talgan requires special care because of slow normalisation of the disturbed hypothalamic-pituitary-adrenal function caused by extended treatment with oral corticosteroids (see Oral Corticosteroid usage and Potential systemic effects of inhaled corticosteroids - HPA axis suppression and adrenal insufficiency under Precautions).
When Talgan treatment is initiated, the patient's asthma should be in a relatively stable phase. A high dose of Talgan should then be given in combination with the previously used oral corticosteroid dose for about 2 weeks. The dose of oral corticosteroid should then be reduced gradually (for example 1 mg prednisolone or equivalent every four days, however, the exact rate of reduction will depend on individual clinical response) to the lowest possible level. The dose of Talgan should not be changed while the patient remains on oral corticosteroids.
In many cases, it may be possible to completely replace the oral corticosteroid with inhaled Talgan. In other patients, a low oral steroid maintenance dose may be necessary. Some patients may experience uneasiness during the withdrawal of oral corticosteroids due to the decreased systemic corticosteroid effect. The physician may need to actively support the patient and to stress the reason for the Talgan treatment.
The length of time needed for the body to regain sufficient natural corticosteroid production is often extended and may be as long as 12 months. Transferred patients should carry a warning card indicating that they may need supplementary systemic corticosteroids during periods of stress, such as severe infection, trauma or surgery. During such times it may be necessary to give additional oral corticosteroids.
During transfer from oral therapy to Talgan, a lower systemic steroid action is experienced. Earlier allergic symptoms may recur (eg. rhinitis, eczema, conjunctivitis) or patients may suffer from tiredness, headache, muscle and joint pain, lassitude and depression or occasionally nausea and vomiting. In these cases, further medical support may be required.
Route of administration: Respiratory (inhalation).
Talgan nebuliser suspension contains 0.1 mg/ml disodium edetate which has been shown to cause bronchoconstriction at levels above 1.2 mg/ml. Acute overdose with Talgan should not present a clinical problem.
History of hypersensitivity to budesonide or any of the excipients.
Special care is needed in patients with pulmonary tuberculosis and viral infections of the airways.
Non steroid-dependent patients: A therapeutic effect is usually reached within 10 days. In patients with excessive mucus secretion in the bronchi, a short (about 2 weeks) additional oral corticosteroid regimen can be given initially. After the course of the oral drug, Talgan nebuliser suspension alone should be sufficient therapy.
Steroid-dependent patients: When transfer from oral corticosteroid to treatment with Talgan nebuliser suspension is initiated, the patient should be in a relatively stable phase. Talgan nebuliser suspension is then given, in combination with the previously used oral steroid dose, for about 10 days.
After that, the oral steroid dose should be gradually reduced (by, for example, 2.5 mg prednisolone or the equivalent each month), to the lowest possible level. In many cases, it is possible to completely substitute Talgan nebuliser suspension for the oral corticosteroid. During transfer from oral therapy to Talgan nebuliser suspension, a generally lower systemic corticosteroid action will be experienced, which may result in the appearance of allergic or arthritic symptoms such as rhinitis, eczema and muscle and joint pain. Specific treatment should be initiated for these conditions. A general insufficient glucocorticosteroid effect should be suspected if, in rare cases, symptoms such as tiredness, headache, nausea and vomiting should occur. In these cases a temporary increase in the dose of oral glucocorticosteroids is sometimes necessary. As with other inhalation therapy, paradoxical bronchospasm may occur, with an immediate increase in wheezing after dosing. If a severe reaction occurs, treatment should be reassessed and an alternative therapy instituted if necessary.
Prolonged treatment with high doses of inhaled corticosteroids, particularly higher than the recommended doses, may result in clinically significant adrenal suppression. Additional systemic corticosteroid cover should be considered during periods of stress or elective surgery. Systemic effects may occur with any inhaled corticosteroids, particularly at high doses prescribed for long periods. These effects are much less likely to occur with inhalation treatment than with oral corticosteroids. Possible systemic effects include Cushing's syndrome, Cushingoid features, adrenal suppression, growth retardation in children and adolescents, decrease in bone mineral density, cataract and glaucoma. It is important, therefore, that the dose of inhaled corticosteroid is titrated to the lowest dose at which effective control of asthma is maintained.
Talgan nebuliser suspension is not intended for rapid relief of acute episodes of asthma where an inhaled short-acting bronchodilator is required. If patients find short-acting bronchodilator treatment ineffective, or they need more inhalations than usual, medical attention must be sought. In this situation consideration should be given to the need for or an increase in their regular therapy, e.g., higher doses of inhaled budesonide or the addition of a long acting beta agonist, or for a course of oral glucocorticosteroid.
Reduced liver function may affect the elimination of glucocorticosteroids. The plasma clearance following an intravenous dose of budesonide however was similar in cirrhotic patients and in healthy subjects. After oral ingestion systemic availability of budesonide was increased by compromised liver function due to decreased first pass metabolism. The clinical relevance of this to treatment with Talgan nebuliser suspension is unknown as no data exist for inhaled budesonide, but increases in plasma levels and hence an increased risk of systemic adverse effects could be expected.
Oral administration of ketoconazole and itraconazole (known inhibitors of CYP3A4 activity in the liver and in the intestinal mucosa causes an increase in the systemic exposure to budesonide. Concomitant treatment with ketoconazole and itraconazole or other potent CYP3A4 inhibitors should be avoided (see Interactions). If this is not possible, the time interval between administrations of the interacting drugs should be as long as possible. A reduction in the dose of budesonide should also be considered.
Influence on growth: It is recommended that the height of children receiving prolonged treatment with inhaled corticosteroids is regularly monitored. If growth is slowed, therapy should be re-evaluated with the aim of reducing the dose of inhaled corticosteroid, if possible, to the lowest dose at which effective control of asthma is maintained. The benefits of the corticosteroid therapy and the possible risks of growth suppression must be carefully weighed. In addition, consideration should be given to referring the patient to a paediatric respiratory specialist.
The nebuliser chamber should be cleaned after every administration. Wash the nebuliser chamber and mouthpiece or face-mask in hot water using a mild detergent. Rinse well and dry, by connecting the nebuliser chamber to the compressor or air inlet.
Effects on Ability to Drive and Use Machine: Talgan does not affect the ability to drive or use machinery.
Results from most studies have not been able to detect an increased teratogenic risk associated with the use of inhaled budesonide. The administration of budesonide during pregnancy requires that the benefits for the mother be weighed against the risk for the foetus. Inhaled glucocorticosteroids should be considered in preference to oral glucocorticosteroids because of the lower systemic effects at the doses required to achieve similar pulmonary responses. Budesonide is excreted in breast milk. However, at therapeutic doses of Talgan nebuliser suspension, no effects on the suckling child are anticipated. Talgan nebuliser suspension can be used during breastfeeding.
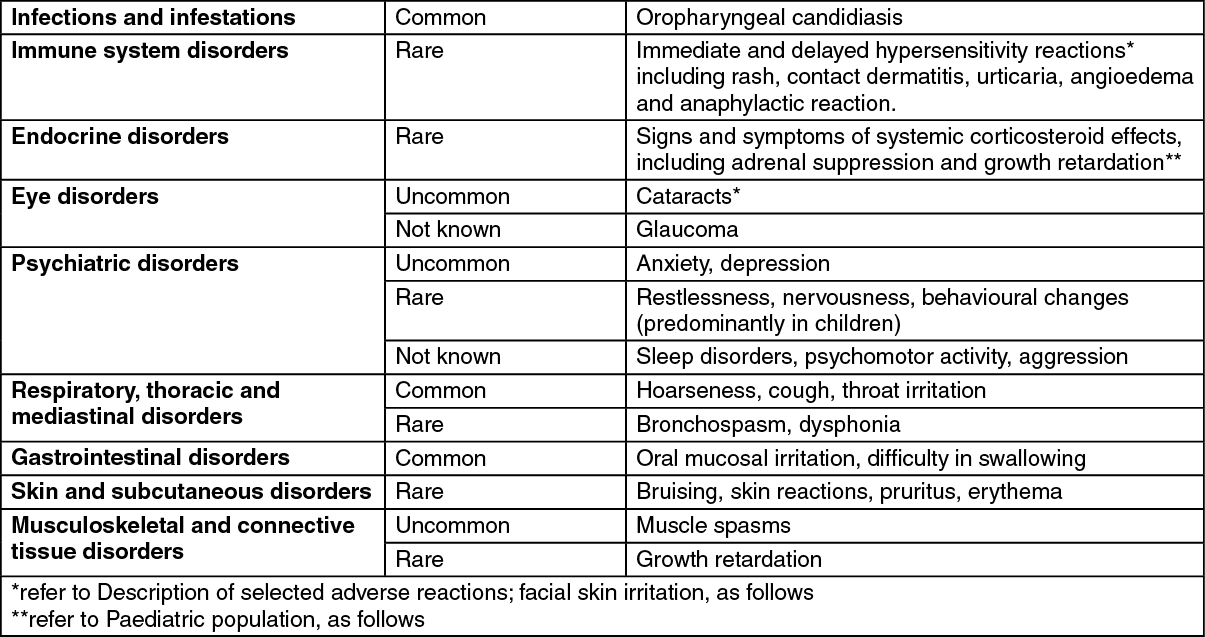
The following adverse drug reactions may occur: (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Occasionally, signs or symptoms of systemic glucocorticosteroid-side effects may occur particularly at higher doses prescribe for prolonged patients. These effects are much less likely to occur than with oral corticosteroids and probably depending on dose, exposure time, concomitant and previous corticosteroid exposure, and individual sensitivity. Possible systemic effects include adrenal suppression, growth retardation in children and adolescents, decreased in bone mineral density, cataract and glaucoma.
Description of selected adverse reactions: The candida infection in the oropharynx is due to drug deposition. Advising the patient to rinse the mouth out with water after each dosing will minimise the risk.
As with other inhalation therapy, paradoxical bronchospasm may occur in very rare cases.
Facial skin irritation has occurred in some cases when a nebuliser with a face mask has been used. To prevent irritation, the facial skin should be washed with water after use of the face mask.
The metabolism of budesonide is primarily mediated by CYP3A4, one of the cytochrome P450 enzymes. Inhibitors of this enzyme, e.g. ketoconazole and itraconazole, can therefore increase the risk of systemic side effects (see Precautions and Side Effects). Other potent inhibitors of CYP3A4 are also likely to markedly increase plasma concentrations levels of budesonide. Therefore, the combination of Talgan with potent CYP3A inhibitors should be avoided and if it is not possible, the period between treatments should be as long as possible. A reduction of the budesonide dose could be considered.
Raised plasma concentrations of and enhanced effects of corticosteroids have been observed in women also treated with oestrogens and contraceptive steroids, but no effect has been observed with budesonide and concomitant intake of low dose combination oral contraceptives.
The suppressive effect on adrenal function is additive if used concomitantly with systemic or intranasal steroids. Because adrenal function may be suppressed, an ACTH stimulation test for diagnosing pituitary insufficiency might show false results (low values).
Instructions for Use: Instruction for correct use of Talgan nebuliser suspension: The plastic single dose unit should be detached from the strip, shaken gently and opened by twisting off the wing tab. The contents of the plastic single dose unit should be gently squeezed into the nebuliser cup. The empty plastic unit should be thrown away and the top of the nebuliser cup replaced. Talgan nebuliser suspension should be administered via a jet nebuliser equipped with a mouthpiece or suitable face mask. The nebuliser should be connected to an air compressor with an adequate air flow (6-8 L/min), and the fill volume should be 2-4 ml.
Note: It is important to instruct the patient: to carefully read the instructions for use in the patient information leaflet which are packed together with each nebuliser; that Ultrasonic nebulisers are not suitable for the administration of Talgan nebuliser suspension and therefore are not recommended; to rinse the mouth out with water after inhaling the prescribed dose to minimise the risk of oropharyngeal thrush; to wash the facial skin with water after using the face mask to prevent irritation; to adequately clean and maintain the nebuliser according to the manufacturer's instructions.
The dosage of Talgan nebuliser suspension should be adjusted to the need of the individual.
Do not store above 30°C. Store in the original package to protect from light.
After opening of the pouch: Do not store above 30°C. Store in their original sachet to protect from light.
Shelf Life: 36 months.
After opening of the pouch: 3 months.
Use immediately after opening of the container. Discard any unused portion.
R03BA02 - budesonide ; Belongs to the class of other inhalants used in the treatment of obstructive airway diseases, glucocorticoids.
Talgan inhalation soln 0.25 mg/mL
2 mL x 20 × 1's
Talgan inhalation soln 0.5 mg/mL
2 mL x 20 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
