Pharmaco-therapeutic group: pneumococcal vaccines.
ATC code: J07AL52.
Pharmacology: Pharmacodynamics: Efficacy and effectiveness in clinical trials: In a large-scale phase III/IV, double-blind, cluster-randomized, controlled, clinical trial in Finland (FinIP), children received either Synflorix or control vaccines according to a 3+1 or 2+1 infant schedule (3-4-5 months of age or 3-5 months of age with booster at 11 months). In the catch-up cohorts, children 7-11 months of age or 12-18 months of age at first vaccine dose received either Synflorix or control vaccines according to the appropriate-for-age Synflorix vaccination schedule.
In a large-scale phase III, randomized, double-blind clinical trial (Clinical Otitis Media and Pneumonia Study - COMPAS), infants aged 6-16 weeks received either Synflorix or the control vaccine according to a 3+1 schedule (2-4-6 months of age with booster at 15-18 months).
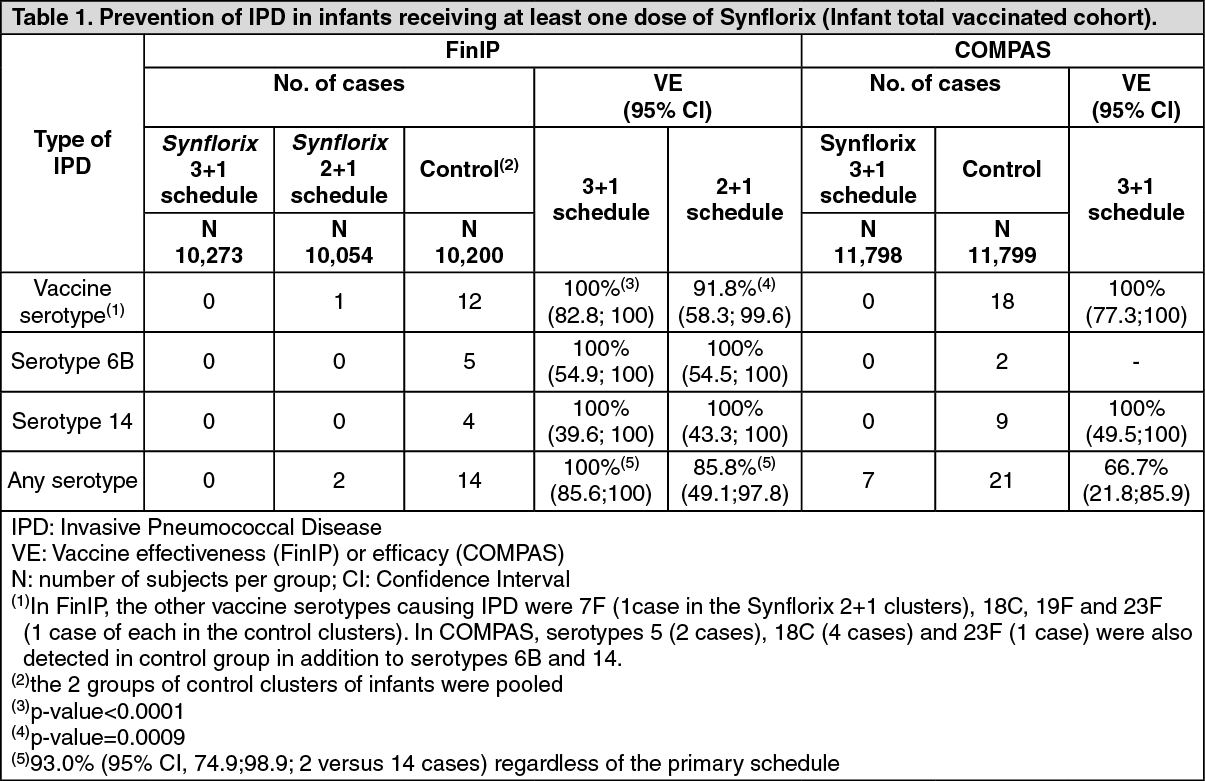
Invasive Pneumococcal Disease (IPD): Infant cohort below 7 months of age at enrolment: Vaccine effectiveness (in FinIP) or efficacy (in COMPAS) was demonstrated in preventing culture-confirmed IPD due to vaccine serotypes (Table 1). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Catch-up cohorts: Among the 15,447 children in the catch-up cohorts, there were no culture-confirmed IPD cases in the Synflorix groups while 7 IPD cases were observed in the control groups (2 and 5 cases in the 7-11 months and 12-18 months cohorts respectively).
Pneumonia: Vaccine efficacy of Synflorix against likely bacterial Community Acquired Pneumonia (CAP), i.e. radiologically confirmed CAP cases with either alveolar consolidation/pleural effusion on the chest X-ray, or with non alveolar infiltrates but with C reactive protein (CRP) ≥ 40 mg/L, was demonstrated in the according-to-protocol (ATP) cohort (immunized with at least the 3-dose primary series) as the primary objective of COMPAS during a follow up of 38 months from study start: 22.0% (95% CI: 7.7; 34.2); P value ≤ 0.002; 240 cases/10,295 subjects in the Synflorix group versus 304 cases/10,201 subjects in the control group.
Vaccine efficacy against CAP with alveolar consolidation or pleural effusion was 25.7% (95% CI: 8.4; 39.6) and against clinically suspected CAP referred for X-ray was 6.7% (95% CI: 0.7; 12.3).
During an observation period of 48 months from study start, vaccine efficacy against likely bacterial CAP was 18.2% (95% CI: 4.1; 30.3), against CAP with alveolar consolidation or pleural effusion 22.4% (95% CI: 5.7; 36.1) and against clinically suspected CAP referred for X-ray 7.3% (95% CI: 1.6; 12.6).
In the FinIP study, vaccine effectiveness in reducing hospital-diagnosed pneumonia cases was 26.7% (95% CI: 4.9; 43.5) in the 3+1 infant schedule and 29.3% (95% CI: 7.5; 46.3) in the 2+1 infant schedule. Vaccine effectiveness was 33.2% (95% CI: 3.0; 53.4) in the 7-11 month cohort and 22.4% (95% CI: -8.7; 44.8) in the 12-18 month cohort.
Acute Otitis Media (AOM): (See Tables 2 and 3.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
No increase in the incidence of AOM due to non-vaccine/non-vaccine related serotypes, or due to other bacterial pathogens was observed in either COMPAS (based on the few cases reported) or POET trial.
Impact on antimicrobial prescriptions: In the FinIP infant total vaccinated cohort, vaccination with Synflorix reduced outpatient prescriptions for amoxicillin, the most frequently prescribed antibiotic for AOM, by 7.9% (95% CI: 2.0; 13.4) in the 3+1 schedule and 7.5% (95% CI: 0.9; 13.6) in the 2+1 schedule. In the Synflorix groups, there was a trend for a reduction in any outpatient antimicrobial prescriptions and in antimicrobial prescriptions usually recommended for otitis media and respiratory infections.
Impact on nasopharyngeal carriage (NPC): The effect of Synflorix on NPC was studied in the nested study of FinIP (5,092 subjects) and in COMPAS (1,921 subjects). In both studies, Synflorix significantly reduced vaccine type carriage (combined and 6B, 19F and 23F individually) with a trend for increase after booster vaccination in non-vaccine/non-vaccine related type NPC resulting in net decrease in overall pneumococcal carriage. In the nested study, a significant reduction was also observed for vaccine serotype 14 and for serotype 19A.
In a clinical study assessing NPC in HIV positive infants (HIV+/+, N = 83) and HIV negative infants born from an HIV positive mother (HIV+/-, N = 101), the HIV exposure or infection did not appear to alter the effect of Synflorix on pneumococcal carriage when compared to the effect in HIV negative infants born from an HIV negative mother (HIV-/-, N = 100).
Effectiveness in post-marketing surveillance: In Brazil, Synflorix was introduced into the national immunization program (NIP) in March 2010, using a 3+1 schedule in infants with a catch-up campaign in children up to 2 years of age. Based on almost 3 years of surveillance following Synflorix introduction, a matched case-control study reported a significant decrease in culture or PCR confirmed IPD due to any vaccine serotype (83.8% (95% CI: 65.9; 92.3)) and IPD due to serotype 19A (82.2% (95% CI: 10.7; 96.4)).
In Finland, Synflorix was introduced into NIP in September 2010, with a 2+1 schedule in infants without catch-up campaign. The relative rate reduction of IPD incidence in children ≤ 5 years of age during the first 3 years after NIP introduction was evaluated. Before and after NIP comparison suggests a significant decrease in the incidence of any culture confirmed IPD (80% (95% CI: 72; 85)), any vaccine serotype IPD (92% (95% CI: 86; 95)) and IPD due to serotype 19A (62% (95% CI: 20; 85)).
In Quebec, Canada, Synflorix was introduced into the infant immunization programme (2 primary doses to infants < 6 months of age and a booster dose at 12 months) following 4.5 years of use of 7-valent Pneumococcal Conjugate Vaccine (PCV). Based on 1.5 years of surveillance following Synflorix introduction, with over 90% coverage in the vaccine-eligible age group, a decrease in vaccine serotype IPD incidence (largely due to changes in serotype 7F disease) was observed with no concomitant increase in non-vaccine serotype IPD incidence, leading to an overall decrease in IPD incidence in the target age group compared to the incidence reported during the preceding period.
Immunogenicity data: Immunologic non-inferiority to 7-valent PCV: In a head-to-head comparative trial with 7-valent PCV, non-inferiority of the immune response to Synflorix measured by ELISA was demonstrated for all serotypes, except for 6B and 23F. The clinical relevance of these differences is unclear, as Synflorix was observed to be effective against IPD caused by serotype 6B in a clinical study (see Table 1). The percentage of vaccinees reaching the ELISA antibody threshold (i.e. 0.20 μg/ml) for serotypes 1, 5 and 7F in Synflorix was at least as good as the aggregate 7-valent PCV response against the 7 common serotypes. The proportion of functional antibody responders (OPA titre ≥ 8) to all serotypes contained in each vaccine were high (> 87.7%) with the exception of serotype 1 for Synflorix post-primary (65.7%). Immunological memory was shown for all vaccine serotypes after a booster dose in the second year of life.
It has also been demonstrated that Synflorix induces an immune response to serotype 19A with 6.1 fold increases in both antibody GMC and OPA GMT observed 1 month after a booster dose compared to pre-booster concentrations.
Immunogenicity in infants from 6 weeks to 6 months of age: In clinical trials, the immunogenicity of Synflorix was evaluated after a 2- or 3-dose primary course according to different schedules (6-14 weeks, 2-4, 3-5 months of age or 6-10-14 weeks, 2-3-4, 3-4-5, 2-4-6 months of age) and after a booster dose given at least 6 months after the last primary dose and from the age of 9 months onwards.
In a clinical study which evaluated the immunogenicity of Synflorix in 2-dose or 3-dose primed subjects, there was no significant difference between the two groups in the percentages of subjects reaching ELISA antibody threshold. A lower percentage of subjects reaching OPA threshold was observed for some vaccine serotypes and serotype 19A in 2-dose primed subjects. In both schedules, a booster response indicative of immunological priming was observed for each vaccine serotype and serotype 19A.
A 3-dose primary schedule has shown higher response against protein D compared to a 2-dose primary schedule. However, the clinical relevance of this observation remains unknown.
A study in South Africa assessed the immunogenicity of Synflorix given as a booster dose at 9 to 10 months of age after a 3-dose (6-10-14 weeks of age) or 2-dose (6-14 weeks of age) priming. The booster dose induced marked increases in antibody GMCs and OPA GMTs for each vaccine serotype and serotype 19A in both groups, indicative of immunological priming.
Immune memory: After a single challenge dose of Synflorix in the 4th year of life, similar anamnestic immune response was observed for all vaccine serotypes and serotype 19A. Anamnestic immune responses to protein D were shown with both schedules.
Immunogenicity in unvaccinated infants and children ≥ 7 months of age (catch-up): In studies in previously unvaccinated 7-11 months children (2+1 schedule) and children 12 months up to 5 years of age (2 dose schedule), antibody GMCs and OPA GMTs for vaccine serotypes and serotype 19A were similar or higher than those induced by 3-dose primary infant series. A similar immune response was observed for protein D in 2 to 5 years old children and infants after a 3-dose primary series.
Immunogenicity in preterm infants: Immunogenicity of Synflorix in very preterm and preterm (gestation period of 27-30 weeks and 31-36 weeks respectively) as well as full term infants was evaluated (3 primary doses at 2, 4, 6 months of age with a booster dose at 15-18 months of age).
After primary vaccination, for each vaccine serotype the proportion of subjects with ELISA antibody concentrations ≥ 0.20 μg/ml and OPA titres ≥ 8 was similar regardless of maturity. With respect to full term, similar immunogenicity was observed in preterm groups except lower antibody GMCs for vaccine serotypes 4, 5, 9V and serotype 19A and lower OPA GMT for serotype 5. Immunological memory was shown for each vaccine serotype and serotype 19A one month after the booster dose.
Immunogenicity in special populations: In a clinical study in South Africa, Synflorix was given to HIV+/+ (asymptomatic or mild disease), HIV+/- and HIV-/- infants (3 primary doses at 6-10-14 weeks of age with a booster dose at 9-10 months of age). Group comparisons (HIV+/+ and HIV+/- versus HIV-/-) suggest comparable immune responses for most vaccine serotypes, serotype 19A and protein D, except a trend for lower post primary OPA response in HIV+/+ group for most vaccine serotypes with unknown clinical relevance. Immunological memory was shown for each vaccine serotype and serotype 19A after the booster dose.
A clinical study in Burkina Faso in children with or without SCD receiving vaccination according to their age (<6 months, 7-11 months, 12-23 months of age) suggests that the immunogenicity of Synflorix is not influenced by SCD.
Immunogenicity and safety of Synflorix were assessed in a limited number of subjects with congenital or acquired asplenia, splenic dysfunction or complement deficiencies: 6 subjects 2-5 years of age and 40 subjects 6-17 years of age (Synflorix is indicated up to 5 years of age). Synflorix was shown to be immunogenic and no new safety concerns were observed in this study.
Toxicology: Pre-clinical Safety Data: A repeated dose toxicity study of pneumococcal conjugate vaccine in rabbit revealed no evidence of any significant local or systemic toxic effects.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image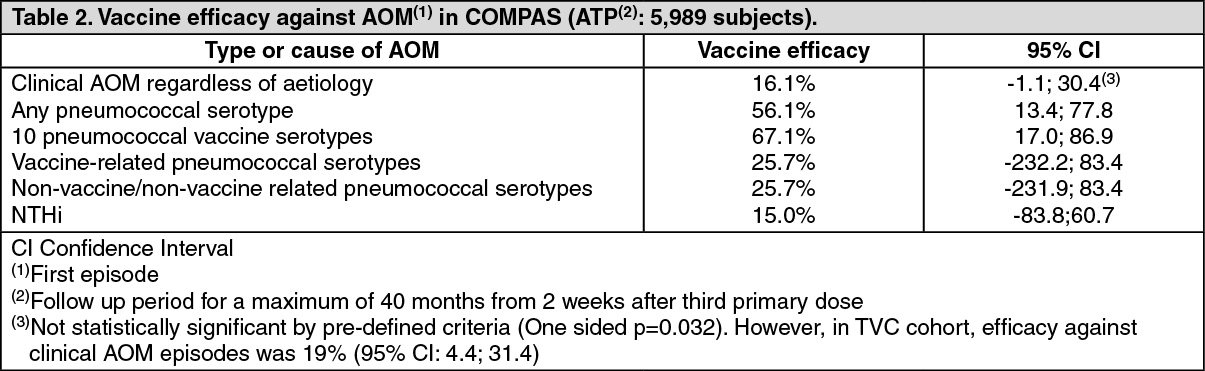 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image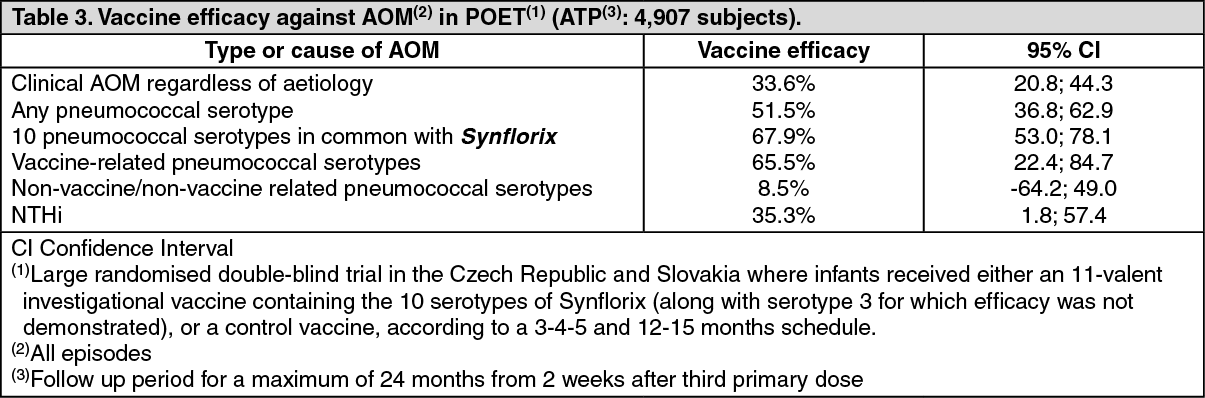 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image (pre-filled syringe) 0.5 mL09a429df-de7d-41e5-9b7c-9faa0009dd0f.GIF)

 Sign Out
Sign Out
