


 Sign Out
Sign Out




The potential for sulbactam's preventing the destruction of penicillins and cephalosporins by resistant organisms was confirmed in whole-organism studies using resistant strains in which sulbactam exhibited marked synergy with penicillins and cephalosporins. As sulbactam also binds with some penicillin binding proteins, sensitive strains are also often rendered more susceptible to sulbactam/cefoperazone than to cefoperazone alone.
The combination of sulbactam and cefoperazone is active against all organisms sensitive to cefoperazone. In addition it demonstrates synergistic activity (up to four-fold reduction in minimum inhibitory concentrations for the combination versus those for each component) in a variety of organisms, most markedly the following: Haemophilus influenzae, Bacteroides species, Staphylococcus species, Acinetobacter calcoaceticus, Enterobacter aerogenes, Escherichia coli, Proteus mirabilis, Klebsiella pneumoniae, Morganella morganii, Citrobacter freundii, Enterobacter cloacae, Citrobacter diversus.
Sulbactam/cefoperazone is active in vitro against a wide variety of clinically significant organisms: Gram-Positive Organisms: Staphylococcus aureus, penicillinase and non-penicillinase-producing strains; Staphylococcus epidermidis, Streptococcus pneumoniae (formerly Diplococcus pneumoniae); Streptococcus pyogenes (Group A beta-hemolytic streptococci); Streptococcus agalactiae (Group B beta-hemolytic streptococci); Most other strains of beta-hemolytic streptococci; Many strains of Streptococcus faecalis (enterococcus).
Gram-Negative Organisms: Escherichia coli, Klebsiella species, Enterobacter species, Citrobacter species, Haemophilus influenzae, Proteus mirabilis, Proteus vulgaris, Morganella morganii (formerly Proteus morganii), Providencia rettgeri (formerly Proteus rettgeri), Providencia species, Serratia species (including S. marcescens), Salmonella and Shigella species, Pseudomonas aeruginosa and some other Pseudomonas species, Acinetobacter calcoaceticus, Neisseria gonorrhoeae, Neisseria meningitidis, Bordetella pertussis, Yersinia enterocolitica.
Anaerobic Organisms: Gram-negative bacilli (including Bacteroides fragilis, other Bacteroides species, and Fusobacterium species); Gram-positive and gram-negative cocci (including Peptococcus, Peptostreptococcus and Veillonella species); Gram-positive bacilli (including Clostridium, Eubacterium and Lactobacillus species).
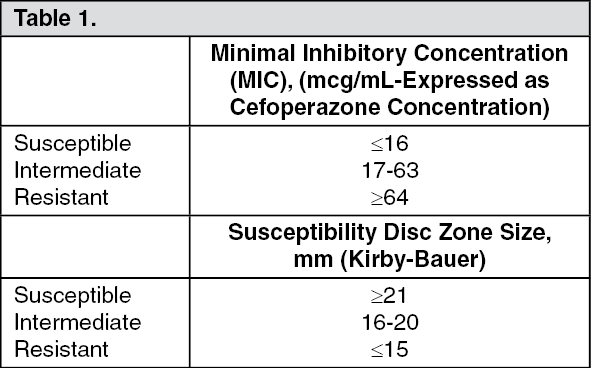
The following susceptibility ranges have been established for sulbactam/cefoperazone: (See Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor MIC determinations, serial dilutions of sulbactam/cefoperazone in a 1:1 sulbactam/cefoperazone ratio may be used with a broth or agar dilution method. Use of a susceptibility test disc containing 30 mcg of sulbactam and 75 mcg of cefoperazone is recommended. A report from the laboratory of "susceptible" indicates that the infecting organism is likely to respond to sulbactam/cefoperazone therapy, and a report of "Resistant" indicates that the organism is not likely to respond. A report of "Intermediate" suggests that the organism would be susceptible to sulbactam/cefoperazone if a higher dosage is used or if the infection is confined to tissues or fluids where high antibiotic levels are attained.
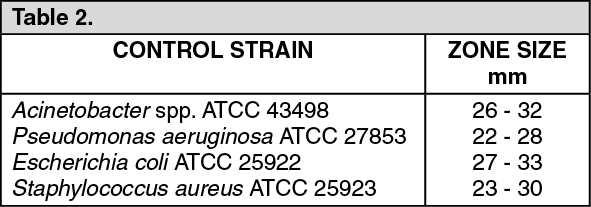
The following quality control limits are recommended for 30 mcg/75 mcg sulbactam/cefoperazone susceptibility discs: (See Table 2).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Approximately 84% of the sulbactam dose and 25% of the cefoperazone dose administered with sulbactam/cefoperazone is excreted by the kidney. Most of the remaining dose of cefoperazone is excreted in the bile. After sulbactam/cefoperazone administration the mean half-life for sulbactam is about 1 hour while that for cefoperazone is 1.7 hours. Serum concentrations have been shown to be proportional to the dose administered. These values are consistent with previously published values for the agents when given alone.
Mean peak sulbactam and cefoperazone concentrations after the administration of 2 grams of sulbactam/cefoperazone (1 g sulbactam, 1 g of cefoperazone) intravenously over 5 minutes were 130.2 and 236.8 mcg/ml, respectively. This reflects the larger volume of distribution for sulbactam (Vd = 18.0-27.6 L) compared to cefoperazone (Vd = 10.2-11.3 L).
Both sulbactam and cefoperazone distribute well into a variety of tissues and fluids including bile, gall bladder, skin, appendix, fallopian tubes, ovary, uterus, and others.
There is no evidence of any pharmacokinetic drug interaction between sulbactam and cefoperazone when administered together in the form of sulbactam/cefoperazone.
After multiple dosing no significant changes in the pharmacokinetics of either component of sulbactam/cefoperazone have been reported and no accumulation has been observed when administered every 8 to 12 hours.
Use in Hepatic Dysfunction: See Precautions.
Use in Renal Dysfunction: In patients with different degrees of renal function administered sulbactam/cefoperazone, the total body clearance of sulbactam was highly correlated with estimated creatinine clearance. Patients who are functionally anephric showed a significantly longer half-life of sulbactam (mean 6.9 and 9.7 hours in separate studies). Haemodialysis significantly altered the half-life, total body clearance, and volume of distribution of sulbactam. No significant differences have been observed in the pharmacokinetics of cefoperazone in renal failure patients.
Use in Elderly: The pharmacokinetics of sulbactam/cefoperazone have been studied in elderly individuals with renal insufficiency and compromised hepatic function. Both sulbactam and cefoperazone exhibited longer half-life, lower clearance, and larger volumes of distribution when compared to data from normal volunteers. The pharmacokinetics of sulbactam correlated well with the degree of renal dysfunction while for cefoperazone there was a good correlation with the degree of hepatic dysfunction.
Use in Children: Studies conducted in pediatrics have shown no significant changes in the pharmacokinetics of the components of sulbactam/cefoperazone compared to adult values. The mean half-life in children has ranged from 0.91 to 1.42 hours for sulbactam and from 1.44 to 1.88 hours for cefoperazone.
Toxicology: Preclinical Safety Data: Use in Pediatrics: Cefoperazone had adverse effects on the testes of prepubertal rats at all doses tested. Subcutaneous administration of 1,000 mg/kg per day (approximately 16 times the average adult human dose) resulted in reduced testicular weight, arrested spermatogenesis, reduced germinal cell population and vacuolation of Sertoli cell cytoplasm. The severity of lesions was dose dependent in the 100 to 1,000 mg/kg per day range; the low dose caused a minor decrease in spermatocytes. This effect has not been observed in adult rats. Histologically, the lesions were reversible at all but the highest dosage levels. However, these studies did not evaluate subsequent development of reproductive function in the rats. The relationship of these findings to humans is unknown.
When sulbactam/cefoperazone (1:1) was given subcutaneously to neonatal rats for 1 month reduced testicular weights and immature tubules were seen in groups given 300 + 300 mg/kg/day. Because there is a great individual variation in the degree of testicular maturation in rat pups and because immature testes were found in controls any relation to study drug is uncertain. No such findings were seen in infant dogs at doses over 10 times the average adult dose.