


 Sign Out
Sign Out




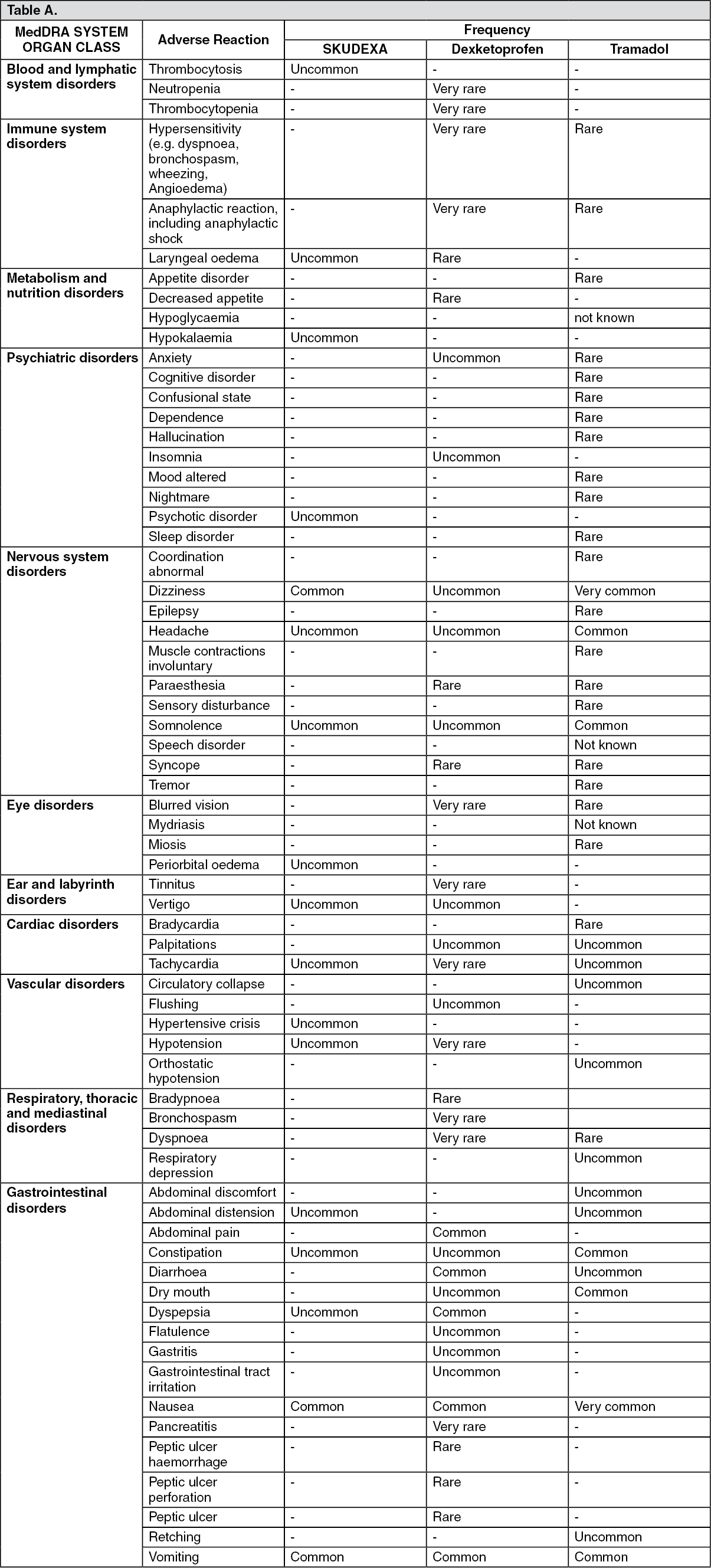
The frequencies are defined as follows: Very common: ≥ 1/10; Common: ≥ 1/100 to <1/10; Uncommon: ≥1/1000 to <1/100; Rare: ≥ 1/10 000 to <1/1000; Very rare (< 1/10,000); Not known: cannot be estimated from the available data. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image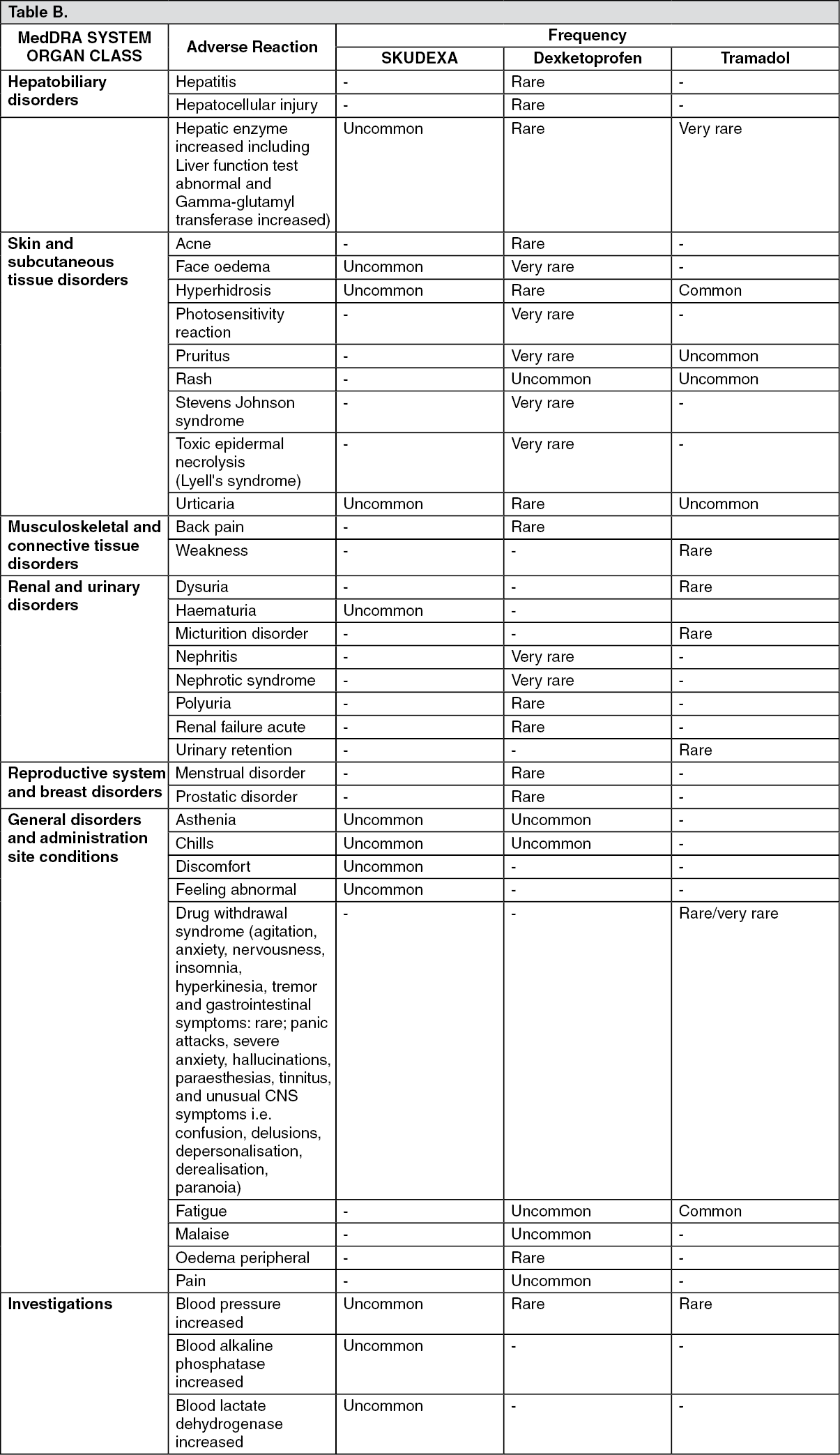 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDexketoprofen-tramadol: In clinical studies the most commonly observed adverse reactions were vomiting, nausea and dizziness (2.9%, 2.7% and 1.1% of patients, respectively).
Dexketoprofen: Gastrointestinal: The most commonly-observed adverse events are gastrointestinal in nature. Peptic ulcers, perforation or gastrointestinal bleeding, sometimes fatal, particularly in the elderly, may occur (see Precautions). Nausea, vomiting, diarrhoea, flatulence, constipation, dyspepsia, abdominal pain, melaena, haematemesis, ulcerative stomatitis, exacerbation of colitis and Crohn's disease (see Precautions) have been reported following administration. Less frequently, gastritis has been observed. Oedema, hypertension and cardiac failure have been reported in association with NSAIDs treatment.
As with other NSAIDs the following undesirable effects may appear aseptic meningitis, which might predominantly occur in patients with systemic lupus erythematosus or mixed connective tissue disease; haematological reactions (purpura, aplastic and haemolytic anaemia, and rarely agranulocytosis and medullar hypoplasia).
Bullous reactions including Stevens Johnson Syndrome and Toxic Epidermal Necrolysis (very rare).
Clinical trial and epidemiological data suggest that use of some NSAIDs (particularly at high doses and in long term treatment) may be associated with a small increase in the risk of arterial thrombotic events (for example myocardial infarction or stroke) (see Precautions).
Tramadol: The most commonly reported adverse reactions due to tramadol are nausea and dizziness, both occurring in more than 10% of patients.
If the recommended doses are considerably exceeded and other centrally depressant substances are administered concomitantly (see Interactions) respiratory depression may occur.
Worsening of asthma has been reported, though a causal relationship has not been established.
Epileptiform convulsions occurred mainly after administration of high doses of tramadol or after concomitant treatment with drugs, which can lower the seizure threshold or themselves induce cerebral convulsions (see Precautions and Interactions).
Symptoms of withdrawal reactions, similar to those occurring during opiate withdrawal, may occur as follows; agitation, anxiety, nervousness, insomnia, hyperkinesia, tremor and gastrointestinal symptoms.
Other symptoms that have very rarely been seen with tramadol discontinuation include: panic attacks, severe anxiety, hallucinations, paraesthesias, tinnitus, and unusual CNS symptoms (i.e. confusion, delusions, depersonalisation, derealisation, paranoia).
View ADR Monitoring Form