Pharmaco-therapeutic group: viral vaccines.
ATC code: J07BH01.
Pharmacology: Pharmacodynamics: Protective efficacy: In clinical trials, efficacy was demonstrated against gastro-enteritis due to rotavirus of the most common genotypes G1P[8], G2P[4], G3P[8], G4P[8] and G9P[8] and against uncommon rotavirus genotypes G8P[4] (severe gastro-enteritis) and G12P[6] (any gastro-enteritis). All of these strains are circulating worldwide.
The protective efficacy of Rotarix lyophilised formulation against any and severe rotavirus gastro-enteritis was evaluated in Europe, Latin America Africa and Asia.
Severity of gastro-enteritis was defined according to two different criteria: the Vesikari 20-point scale, which evaluates the full clinical picture of rotavirus gastro- enteritis by taking into account the severity and duration of diarrhoea and vomiting, the severity of fever and dehydration as well as the need for treatment or; the clinical case definition based on World Health Organization (WHO) criteria.
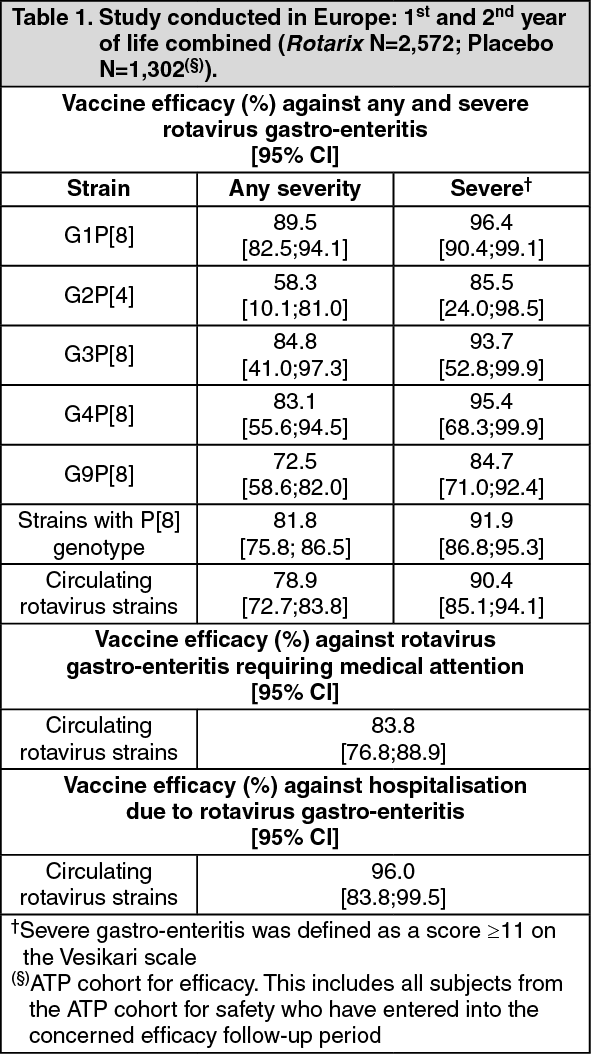
Protective efficacy in Europe and Latin America: After two doses of Rotarix, the protective vaccine efficacy observed in the studies conducted in Europe and Latin America during the first and second year of life combined is presented in table 1 and table 2. (See Table 1 and Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The vaccine efficacy against severe rotavirus gastro-enteritis was 38.6% (95% CI: <0.0;84.2) for G2P[4] strain. The number of cases, on which the estimates of efficacy against G2P[4] were based, were very small.
A pooled analysis of four efficacy studies, showed a 71.4% (95% CI: 20.1;91.1) efficacy against severe gastro-enteritis (Vesikari score ≥11) caused by rotavirus G2P[4] strain.
Since the immune response observed after 2 doses of Rotarix liquid formulation was comparable to the immune response observed after 2 doses of Rotarix lyophilised formulation, the levels of vaccine efficacy observed with the lyophilised formulation can be extrapolated to the liquid formulation.
Protective efficacy in Africa: A clinical study performed in Africa in more than 4,900 subjects evaluated Rotarix given at approximately 10 and 14 weeks of age (2 doses) or 6, 10 and 14 weeks of age (3 doses). The vaccine efficacy against severe rotavirus gastro-enteritis during the first year of life was 61.2% (95% CI: 44.0;73.2). The study was not powered to evaluate a difference in vaccine efficacy between the 2- and 3-dose regimens.
The protective vaccine efficacy observed against any and severe rotavirus gastro-enteritis is presented in Table 3. (See Table 3.)
Click on icon to see table/diagram/image
Sustained efficacy up to 3 years of age in Asia: A clinical study conducted in Asia (Hong Kong, Singapore and Taiwan) in more than 10000 subjects evaluated Rotarix given according to different schedules (2, 4 months of age; 3, 4 months of age).
After two doses of Rotarix, the protective vaccine efficacy observed up to 3 years of age is presented in table 4. (See Table 4.)
Click on icon to see table/diagram/image
Immune response: In different clinical studies conducted in Europe, Latin America and Asia, 1,957 infants received Rotarix lyophilised formulation and 1,006 infants received a placebo according to different vaccination schedules. The percentage of subjects initially seronegative for rotavirus (IgA antibody titres <20 U/ml (by ELISA)) with serum anti-rotavirus IgA antibody titers ≥20U/ml one or two months after the second dose of vaccine or placebo ranges from 77.9% to 100% and from 0% to 17.1% respectively.
In three comparative trials, the immune response elicited by Rotarix liquid formulation was comparable to the one elicited by Rotarix lyophilized formulation.
In a clinical study conducted in Africa, the immune response was evaluated in 332 infants who received Rotarix (N=221) or placebo (N=111) according to a 10 and 14 weeks schedule (2 doses) or 6, 10 and 14 weeks schedule (3 doses). The percentage of subjects initially seronegative for rotavirus (IgA antibody titres < 20 U/ml (by ELISA)) with serum anti- rotavirus IgA antibody titers ≥20 U/ml one month after the last dose of vaccine or placebo was 58.4% (pooled regimens) and 22.5%, respectively.
Immune response in preterm infants: In a clinical study conducted in preterm infants with the lyophilised formulation, Rotarix was immunogenic; 85.7% of subjects achieved serum anti-rotavirus IgA antibody titers ≥20U/ml (by ELISA) one month after the second dose of vaccine.
Safety in infants with human immunodeficiency (HIV) infection: In a clinical study, 100 infants with HIV infection were administered Rotarix lyophilised formulation or placebo. The safety profile was similar between Rotarix and placebo recipients.
Vaccine shedding: Excretion of the vaccine virus in the stools occurs after vaccination and lasts for 10 days on average with peak excretion around the 7th day. Viral antigen particles detected by ELISA were found in 50% of stools after the first dose and 4% of stools after the second dose. When these stools were tested for the presence of live vaccine strain, 17% were positive.
In two comparative controlled trials, vaccine shedding after vaccination with Rotarix liquid formulation was comparable to that observed after vaccination with Rotarix lyophilised formulation.
Effectiveness: In observational studies, vaccine effectiveness was demonstrated against severe gastro-enteritis leading to hospitalisation due to rotavirus of common genotypes G1P[8], G2P[4], G3P[8] and G9P[8] as well as the less common rotavirus genotype G9P[4] and G9P[6]. All of these strains are circulating worldwide.
Table 5 shows the results of several matched case-control studies conducted to evaluate the effectiveness of Rotarix against severe rotavirus gastro-enteritis leading to hospitalisation. (See Table 5.)
Click on icon to see table/diagram/image
Impact on mortality§: Impact studies with Rotarix conducted in Panama, Brazil and Mexico showed a decrease in all cause diarrhoea mortality ranging from 22% to 56% in children less than 5 years of age, within 2 to 3 years after vaccine introduction.
Impact on hospitalisation§: In a retrospective database study in Belgium conducted in children 5 years of age and younger, the direct and indirect impact of Rotarix vaccination on rotavirus-related hospitalisation ranged from 64% (95% CI: 49;76) to 80% (95% CI: 77;83) two years after vaccine introduction. Similar studies in Brazil, Australia and El Salvador showed a reduction of 45 to 88% .
In addition, two impact studies on all-cause diarrhoea hospitalisation conducted in Latin America showed a reduction of 38 to 40% four years after vaccine introduction.
§NOTE : Impact studies are meant to establish a temporal relationship but not a causal relationship between the disease and vaccination.
Clinical Studies: See Pharmacodynamics as previously mentioned.
Pharmacokinetics: Evaluation of pharmacokinetic properties is not required for vaccines.
Toxicology: Preclinical Safety Data: Preclinical data reveal no special hazard for humans based on conventional studies of repeated dose toxicity.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image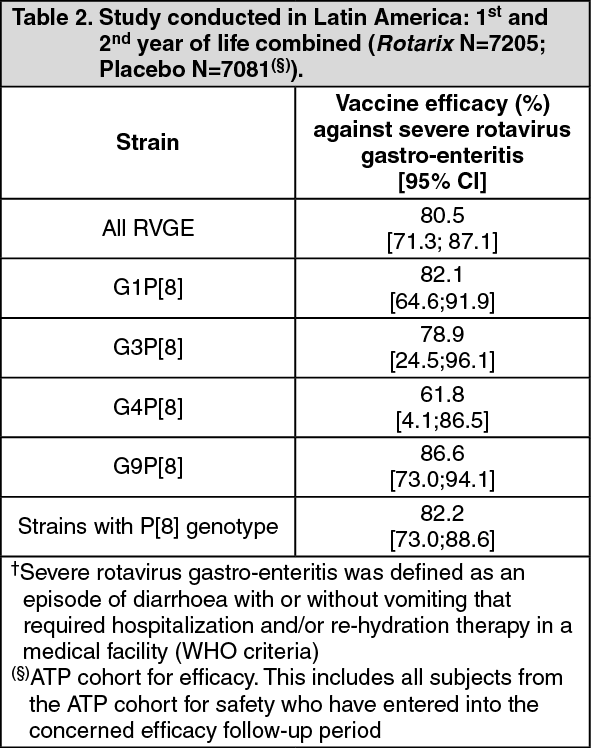 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image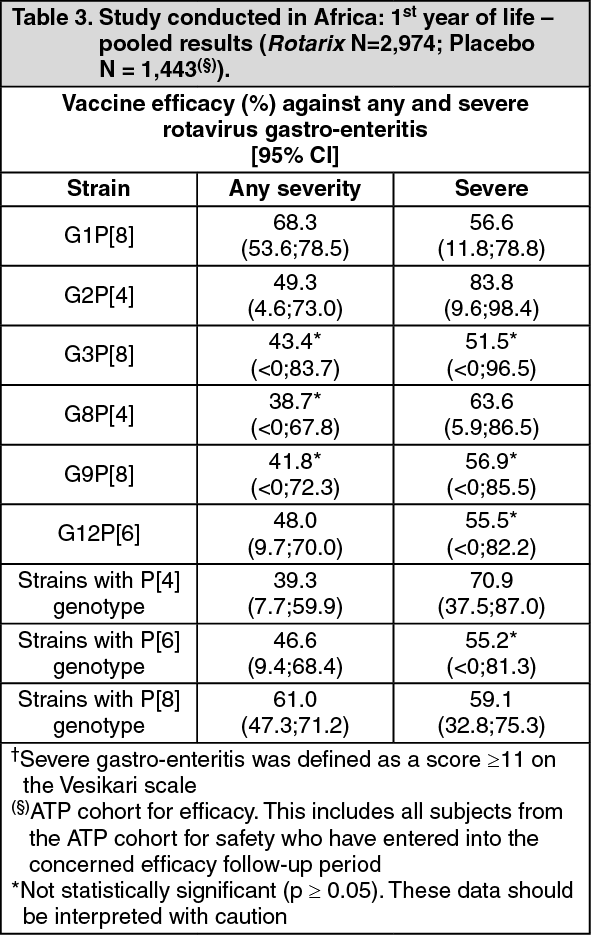 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image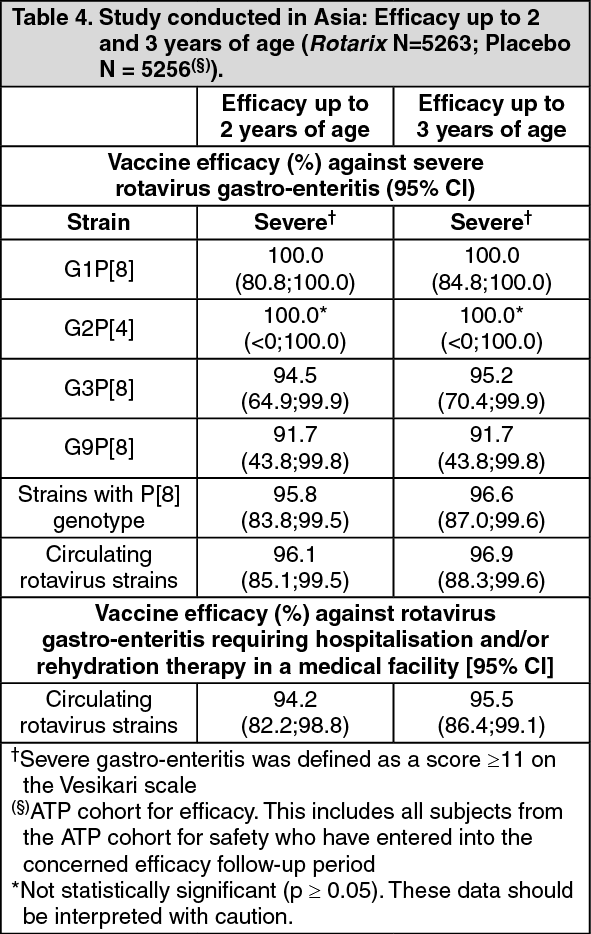 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image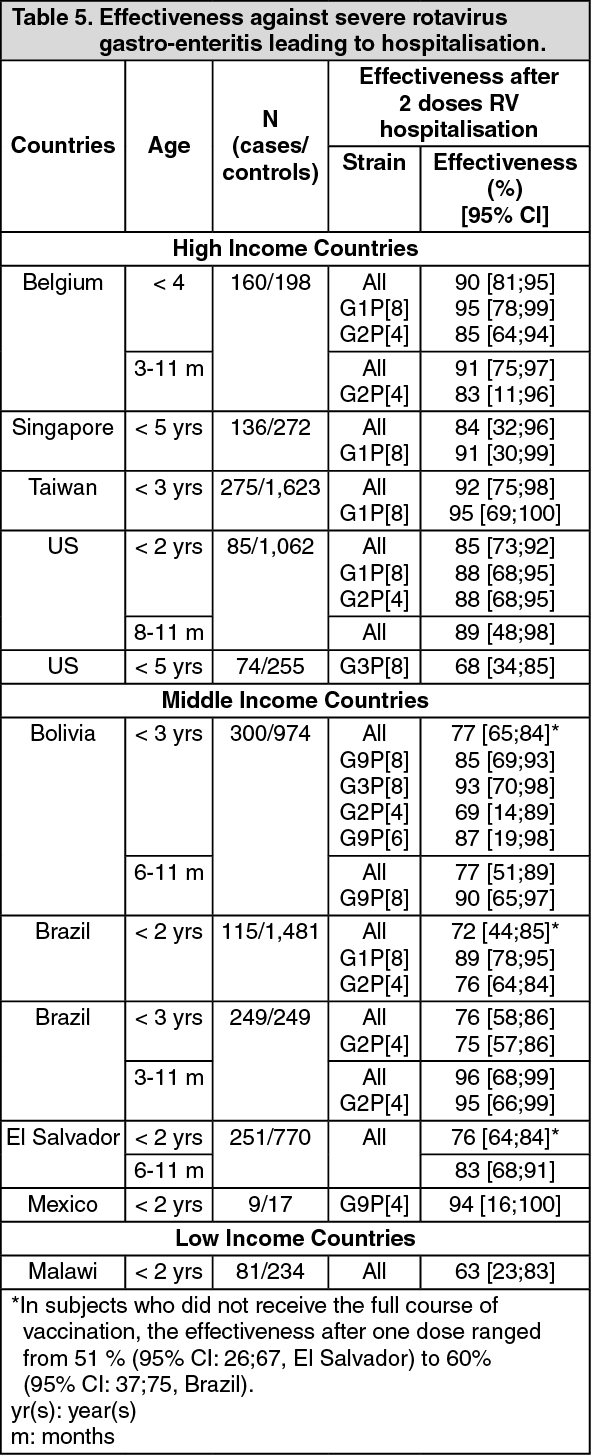 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image 1.5 mLecfc1dc1-0d35-4775-822a-9faa000a222d.GIF)

 Sign Out
Sign Out
