Myelodysplastic syndromes (MDS): Most Commonly Occurring Adverse Reactions: neutropenia, thrombocytopenia, anemia, fatigue, pyrexia, nausea, cough, petechiae, constipation, diarrhea, and hyperglycemia.
Blood and lymphatic system disorders: Neutropenia, Thrombocytopenia, Anemia NOS, Febrile neutropenia, Leukopenia NOS, Lymphadenopathy, Thrombocythemia, Anemia, Leukopenia, Pancytopenia, myelosuppression, splenomegaly.
Cardiac disorders: Pulmonary edema NOS, Cardiac failure congestive, Tachycardia, myocardial infarction, cardio-respiratory arrest, cardiomyopathy, atrial fibrillation, supraventricular tachycardia.
Eye disorders: Vision blurred.
Ear and Labyrinth disorders: Ear pain.
Gastrointestinal disorders: Nausea, Constipation, Diarrhea NOS, Vomiting NOS, Abdominal pain NOS, Oral mucosal petechiae, Stomatitis, Dyspepsia, Ascites, Gingival bleeding, Hemorrhoids, Loose stools, Tongue ulceration, Dysphagia, Oral soft tissue disorder NOS, Lip ulceration, Abdominal distension, Abdominal pain upper, Gastro-esophageal reflux disease, Glossodynia, Abdominal pain, Diarrhea, Oral pain, Toothache, Vomiting, gingival pain, upper gastrointestinal hemorrhage.
General disorders and administrative site disorders: Pyrexia, Edema peripheral, Rigors, Edema NOS, Pain NOS, Lethargy, Tenderness NOS, Fall, Chest discomfort, Intermittent pyrexia, Malaise, Crepitations NOS, Catheter site erythema, Catheter site pain, Injection site swelling, Asthenia, Chest pain, Chills, Fatigue, Mucosal inflammation, Edema, Pain, catheter site hemorrhage.
Hepatobiliary disorders: Hyperbilirubinemia, cholecystitis.
Infections and infestations: Pneumonia NOS, Cellulitis, Candidal infection NOS, Catheter related infection, Urinary tract infection NOS, Staphylococcal infection, Oral candidiasis, Sinusitis NOS, Bacteremia, Pneumonia, Sinusitis, Staphylococcal bacteremia, Tooth abscess, Upper respiratory tract infection, Urinary tract infection, fungal infection, sepsis, bronchopulmonary aspergillosis, peridiverticular abscess, respiratory tract infection, pseudomonal lung infection,
Mycobacterium avium complex infection.
Injury, poisoning and procedural complications: Transfusion reaction, Abrasion NOS, Contusion, post procedural pain, post procedural hemorrhage.
Investigations: Cardiac murmur NOS, Blood alkaline phosphatase NOS increased, Aspartate aminotransferase increased, Blood urea increased, Blood lactate dehydrogenase increased, Blood albumin decreased, Blood bicarbonate increased, Blood chloride decreased, Protein total decreased, Blood bicarbonate decreased, Blood bilirubin decreased, Blood bilirubin increased, Breath sounds abnormal, Weight decreased.
Metabolism and nutrition disorders: Hyperglycemia NOS, Hypoalbuminemia, Hypomagnesemia, Hypokalemia, Hyponatremia, Appetite decreased NOS, Anorexia, Hyperkalemia, Dehydration, Hyperglycemia.
Musculoskeletal and connective tissue disorders: Arthralgia, Pain in limb, Back pain, Chest wall pain. Musculoskeletal discomfort, Myalgia, Bone pain, Muscle spasms, Muscular weakness, musculoskeletal pain, Pain in extremity.
Nervous system disorders: Headache, Dizziness, Hypoesthesia, intracranial hemorrhage.
Psychiatric disorders: Insomnia, Confusional state, Anxiety, Depression, mental status changes.
Renal and urinary disorders: Dysuria, Urinary frequency, renal failure, urethral hemorrhage.
Respiratory, thoracic and Mediastinal disorders: Cough, Pharyngitis, Crackles lung, Breath sounds decreased, Hypoxia, Rales, Postnasal drip, Dyspnea, Epistaxis, Pharyngolaryngeal pain, Pleural effusion, Sinus congestion, hemoptysis, lung infiltration, pulmonary embolism, respiratory arrest, pulmonary mass.
Skin and subcutaneous tissue disorders: Ecchymosis, Rash NOS, Erythema, Skin lesion NOS, Pruritus, Alopecia, Urticaria NOS, Swelling face, Dry skin, Night sweats, Petechiae, Rash, Skin lesion.
Vascular disorders: Petechiae, Pallor, Hypotension NOS, Hematoma NOS, Hypertension, Hypotension.
Allergic Reaction: Hypersensitivity (anaphylactic reaction).
No overall difference in safety was detected between patients > 65 years of age and younger patients in these myelodysplasia studies. No significant gender differences in safety or efficacy were detected.
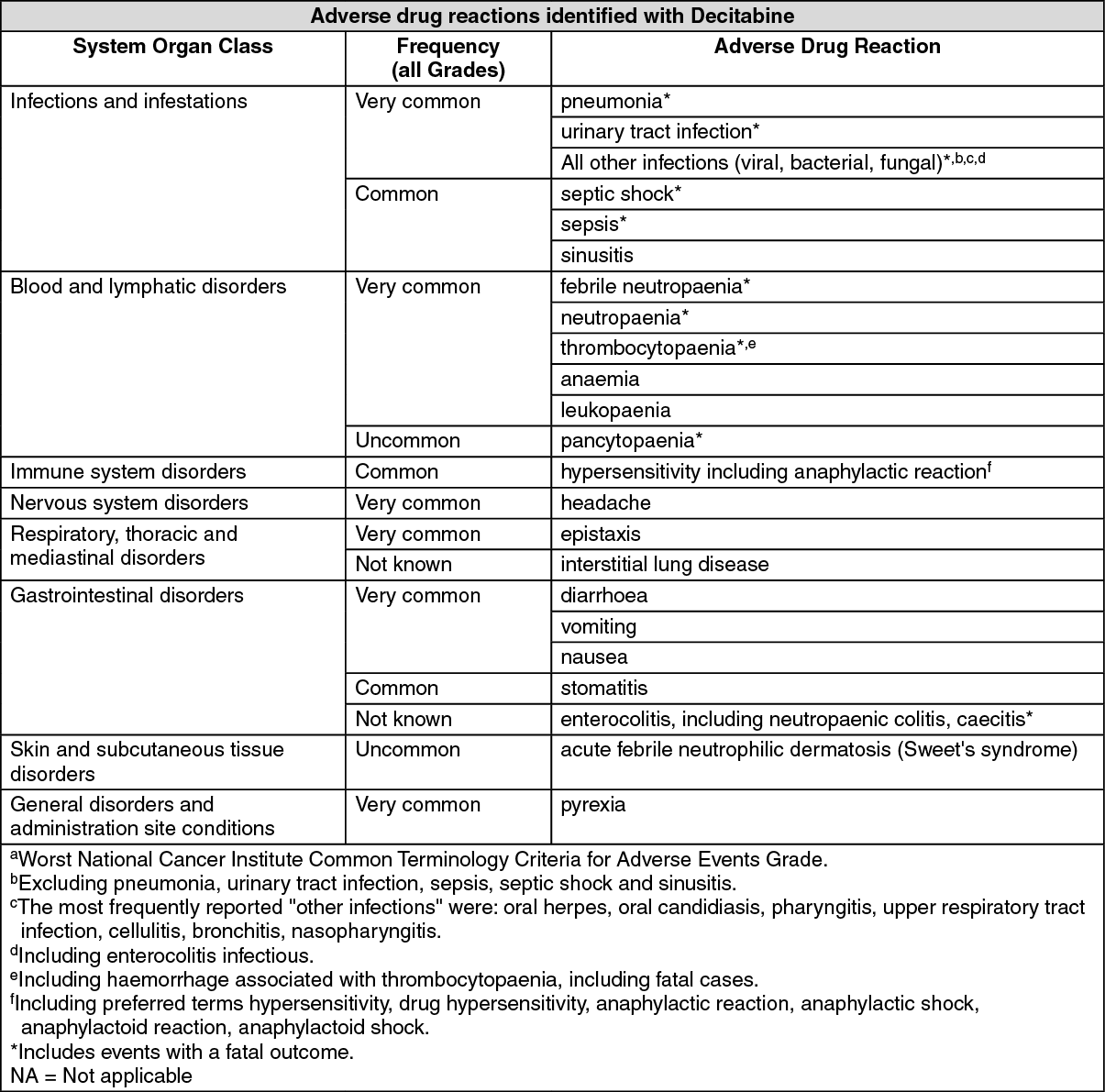
Acute myeloid leukemia (AML): Summary of the safety profile: The most common adverse drug reactions reported during treatment with decitabine are pyrexia, anaemia and thrombocytopaenia.
The most common Grade 3/4 adverse drug reactions included pneumonia, thrombocytopaenia, neutropaenia, febrile neutropaenia and anaemia.
It has been reported that patients treated with decitabine had adverse events with an outcome of death during treatment or within 30 days after the last dose of study drug.
In the decitabine treatment group, there was a higher incidence of treatment discontinuation due to adverse events in women compared to men.
Tabulated list of adverse drug reactions: Adverse drug reactions reported in AML patients treated with decitabine are summarised in the table as follows: Within each frequency grouping, adverse drug reactions are presented in order of decreasing seriousness. (See table.)
 Click on icon to see table/diagram/image
Description of selected adverse drug reactions:
Click on icon to see table/diagram/image
Description of selected adverse drug reactions: Haematologic adverse drug reactions: The most commonly reported haematologic adverse drug reactions associated with decitabine treatment included febrile neutropaenia, thrombocytopaenia, neutropaenia, anaemia and leukopaenia.
Serious bleeding-related adverse drug reactions, some of which lead to a fatal outcome, such as central nervous system (CNS) haemorrhage and gastrointestinal (GI) haemorrhage, in the context of severe thrombocytopaenia, were reported in patients receiving decitabine.
Haematological adverse drug reactions should be managed by routine monitoring of complete blood counts and early administration of supportive treatments as required. Supportive treatments include, administration of prophylactic antibiotics and/or growth factor support (e.g., G-CSF) for neutropaenia and transfusions for anaemia or thrombocytopaenia according to institutional guidelines.
Infections and infestations adverse drug reactions: Serious infection-related adverse drug reactions, with potentially fatal outcome, such as septic shock, sepsis, pneumonia, and other infections (viral, bacterial and fungal) were reported in patients receiving decitabine.
Gastrointestinal disorders: Occurrences of enterocolitis, including neutropaenic colitis, caecitis have been reported during treatment with decitabine. Enterocolitis may lead to septic complications and may be associated with fatal outcome.
Respiratory, thoracic and mediastinal disorders: Cases of interstitial lung disease (including pulmonary infiltrates, organising pneumonia and pulmonary fibrosis) without signs of infectious aetiology have been reported in patients receiving decitabine.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
