Pharmacotherapeutic group: Antivirals for systemic use, direct-acting antivirals (DAAs).
Pharmacology: Pharmacodynamics: Mechanism of action: Ravidasvir is an inhibitor of non-structural protein 5A (NS5A), a multifunctional protein that is an essential component of the HCV replication complex. Ravidasvir inhibits replication of variant HCV replicons encoding resistance mutations for the other major classes of HCV DAAs. HCV variants with reduced susceptibility to ravidasvir remain fully susceptible to other classes of HCV inhibitors.
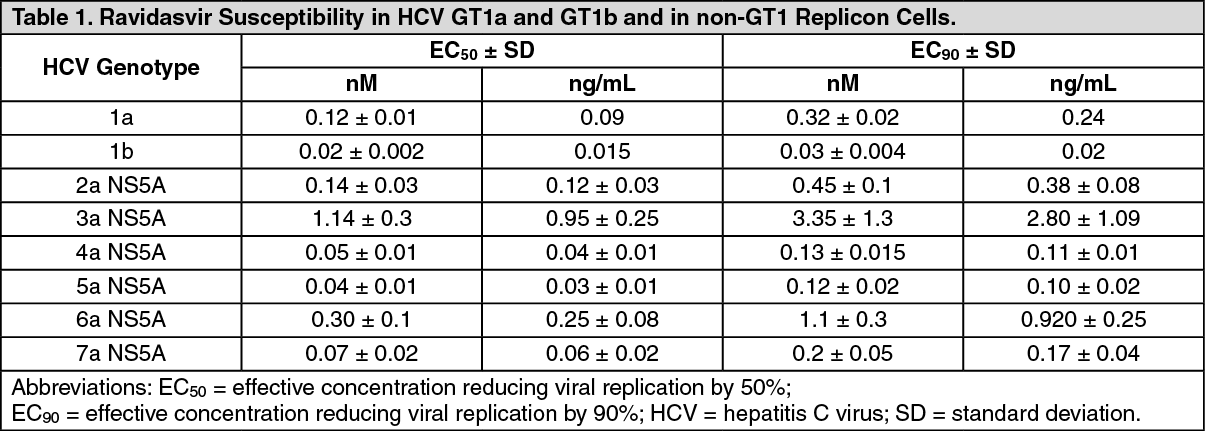
Antiviral activity: The 50% effective concentration (EC
50) values and 90% effective concentration (EC
90) values of ravidasvir for various HCV genotypes 1a and 1b and in non-genotype 1 replicon cells are presented in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Increasing the concentration of human serum from 1% to 40% led to a 9- to 11-fold shift in EC
50 and EC
90 values for genotypes 1a and 1b, consistent with the high protein binding observed in equilibrium dialysis studies.
Combination index values calculated for paired inhibitors indicate additive effects when ravidasvir is combined with NS3 protease inhibitor (ITMN-191), interferon-α and non-nucleoside polymerase inhibitor (HCV-796) and additive to synergistic effects when combined with a NS5B nucleoside polymerase inhibitor (PSI-6130). No antagonism was observed.
No significant inhibitory activity was observed against a panel of RNA and DNA viruses such as bovine viral diarrheal virus (BVDV), human rhino virus (HRV)-16 and influenza-B (Flu-B), confirming that ravidasvir is a specific inhibitor of HCV replication.
Resistance: In cell cultures: Replicons of HCV genotypes 1a and 1b and a panel of genotype 1b chimera replicons containing critical segments of the NS5A gene of HCV genotypes 2a, 3a, 4a, 5a and 6a have been evaluated
in vitro with the highest concentration capped at 1,000 nM ravidasvir. Resistant colonies emerged on most plates, with the number of resistant colonies being lower at the higher concentrations of ravidasvir. At a ravidasvir concentration of 1,000 nM only a small number of colonies were observed with HCV genotype 2a and 4a NS5A replicon cells. Genotyping of replicons from recovered colonies confirmed the presence of resistance substitutions.
Consistent with patterns of resistance-associated substitutions for other NS5A inhibitors, one or more changes at amino acid positions 28, 30, 31 and 93 within domain 1 of the NS5A protein were observed. Additional substitutions, such as P58L (4a NS5A) and T58A (6a NS5A), emerged at lower concentrations of ravidasvir, but these were not present at high ravidasvir concentrations (1,000 nM). Colony formation assays using HCV genotype 1a replicon cells yielded the most diverse set of substitutions, suggesting that multiple single and linked substitutions confer resistance in this genotype. This is in contrast with the results obtained using the HCV genotype 2a, 3a, and 6a NS5A replicon cell lines, which consistently yielded single preferred substitutions F28S (genotypes 2a and 6a) and Y93H (genotype 3a) that conferred high-level resistance. Similar to the linked substitutions found in genotype 1a replicon cells, combination substitutions L31F/V+Y93H (genotype 1b), L30H+Y93H (genotype 4a) and Q30H+L31F (genotype 5a) are required to achieve high level resistance.
In clinical studies: Ravida monotherapy: Three days of Ravida monotherapy at doses ranging from 40 mg to 240 mg once daily led to a rapid reduction of HCV RNA level in 35/40 subjects. Seven of the 35 had NS5A resistance associated variants (RAVs) at baseline. The 5 non-responders, who had <1 log
10 reduction in HCV RNA on day 4, included one genotype 1b subject with genetically linked R30Q+L31I+Y93H RAVs, one genotype 2a with F28L+L31M, two genotype 3A with Y93H and one genotype 3a with A30K.
As wild-type virus was eliminated, treatment-emergent RAVs were detected in 31/32 genotype 1 subjects 8-48 hours after first dose, however these were not further enriched with continued treatment, indicating that Ravida can inhibit replication of these resistant variants. The percentage of linked substitutions was low overall in all genotype 1 subjects, consistent with enrichment of pre-existing variants rather than emergence of new strains.
The most common emergent RAVs in genotype 1a subjects were M28T, Q30R, Q30H, L31M, Y93H and Y93C, with Q30R the most frequent. In genotype 1b subjects, R30Q, L31M and Y93H were the most common emergent RAVs, with Y93H the most frequent. Y93H was the most frequent emergent RAV in the genotype 3a subjects.
Ravida in combination with NS5B inhibitor: Viral resistance has been assessed in HCV chronically infected adults with no or compensated cirrhosis treated with Ravida plus sofosbuvir in the STORM-C-1 study. The study population included 301 subjects infected with virus genotypes 1 (42%), 2 (1%), 3 (52%) and 6 (6%). Among the 81 cirrhotic subjects, 65% had genotype 3 infection.
HCV RNA sequences were obtained for 292/301 subjects (all except 4 non-virological failures and 5 for whom sequencing failed). NS5A RAVs were detected in 91/292 (31.2%) at baseline. The distribution of the RAVs was heterogeneous across genotypes, with 28V and 93H predominantly found in the genotype 1a subjects, 93H in genotype 1b, 93H and 62L in genotype 3a; 30K and 31M in genotype 3b, and 28V and 93S in genotype 6. The impact of baseline RAVs on SVR12 is shown in Table 2. (See Table 2.)
Click on icon to see table/diagram/image
The presence of single or multiple baseline NS5A RAVs did not impact treatment outcomes for genotypes 1a, 1b, 2 or 3b. SVR12 in subjects with one or more RAVs was 93.5% in genotype 3a and 78.6% in genotype 6. Among the 23 genotype 3a subjects with the NS5A 93H RAV, 21 (91.3%) achieved SVR12. 11 of the genotype 6 subjects, including all 3 virological failures, had the NS5A double RAV 28V+93S. 10 of these 11 were genotype 6n, which has both RAVs in the reference baseline sequence.
There was no emergence of new NS5A RAVs in any of the subjects who experienced virological failure. One genotype 6n subject had an emergent NS5B (sofosbuvir) RAV (282T/C) after virological failure.
Cross-resistance: A series of cross-resistance assays was performed and the data indicate that ravidasvir retained its ability to inhibit each of these resistant variants with EC
50 values equivalent to those observed in the wild-type genotype 1b replicon cells, confirming the ability of ravidasvir to inhibit variants that emerge with other distinct classes of HCV inhibitors. Ravidasvir-resistant variants retained their susceptibility to other classes of HCV inhibitors. Ravidasvir can be used in combination with other classes of HCV inhibitors to help prevent the emergence of resistant strains.
Clinical efficacy and safety: Ravidasvir + NS5B inhibitor: The efficacy and safety of Ravida 200 mg QD (once daily) + sofosbuvir 400 mg QD was evaluated in the pivotal study STORM-C-1 conducted in Malaysia and Thailand. The primary efficacy endpoint of STORM-C-1 was sustained virologic response 12 weeks after end of treatment (SVR12) as determined by HCV RNA level <LLOQ using a real-time polymerase chain reaction (PCR) method (Roche COBAS AmpliPrep/TaqMan or Abbott m2000 system).
Of the 301 subjects enrolled in STORM-C-1, 220 non-cirrhotic subjects were allocated to Ravida + sofosbuvir for 12 weeks and 81 compensated cirrhotic subjects were allocated to Ravida + sofosbuvir for 24 weeks. A total of 298 (99%) subjects completed the study and 3 (1%) subjects (2 non-cirrhotic and 1 cirrhotic) prematurely discontinued the study due to adverse events. Demographic and baseline characteristics are summarised in Table 3. (See Table 3.)
Click on icon to see table/diagram/image
High SVR12 results above 95% were observed in the key subpopulations including cirrhotic (96.3%) and non-cirrhotic subjects (97.3%), HIV co-infected (96.7%) or not (97.1%), previous IFN experienced (96.0%) or not (97.5%), and across genotype 1a (99.0%), genotype 1b (100.0%), and genotype 3a (96.4%). Genotype 3 cirrhotic subjects achieved 96.8% SVR12. Subjects with genotype 6 achieved 81.3% SVR12 (13 of 16 subjects). Both genotype 2 subjects achieved SVR12.
No significant association was observed between SVR12 and sex, age, ethnicity (Malay, Thai, other), site, baseline BMI, cirrhotic status, baseline HCV RNA, baseline ALT, baseline AST, IL28B, prior interferon-based HCV treatment status, or HIV co-infection status (p>0.05).
Treatment with Ravida + sofosbuvir led to a rapid decrease in viral load. The mean HCV ribonucleic acid (RNA) count was 6.15 log
10 IU/mL at baseline and decreased to 2.03 log
10 IU/mL at week 1, 1.18 log
10 IU/mL at week 4, 1.14 log
10 IU/mL at week 8, and 1.12 log
10 IU/mL at week 12.
Table 4 shows summary of the main efficacy results.
Overall, 9 subjects (6 [3%] non-cirrhotic subjects and 3 [4%] cirrhotic subjects) did not achieve SVR12; 1 subject due to virological breakthrough, 4 subjects due to virological relapse, and 4 subjects due to non-virologic failure (Table 5). Genotype 3 status, HIV status, and prior interferon-based HCV treatment status did not appear to affect SVR12 rate. Three virological failures were observed in the genotype 6 group. No other risk factors were identified among the subjects who failed treatment. (See Tables 4 and 5.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Ravidasvir + other DAAs: In published clinical studies, ravidasvir 200 mg once daily demonstrated ≥ 95% SVR12 across all tested genotypes when combined with other appropriate DAAs (Table 6). (See Table 6.)
Click on icon to see table/diagram/image
Pharmacokinetics: The mean steady-state pharmacokinetic parameters of ravidasvir in 25 HCV mono-infected subjects receiving 200 mg ravidasvir and 400 mg sofosbuvir QD are presented in Table 7. (See Table 7.)
Click on icon to see table/diagram/image
Absorption: Following oral administration of ascending single doses (80-320 mg) to healthy subjects, ravidasvir was relatively rapidly absorbed with concentrations peaking at a median of 1.5 to 2 hours post-dose. Ravidasvir C
max and AUC increased in a dose-proportional manner and 24-hour post dose plasma concentrations were above ravidasvir EC
90 values for HCV genotypes 1 to 7. When dosed for 5 days, values of AUC
0-∞ on day 1 and AUCτ on day 5 were similar.
Compared with healthy volunteers, subjects with chronic HCV infection seem to have higher inter-subject variability. Ravidasvir C
max and AUC
0-∞ were generally lower in HCV subjects than in healthy volunteers, while T
max was similar in both groups.
Effects of food: When taken with food, the average C
max was reduced compared to the fasted condition, however the relative bioavailability was essentially unchanged (fed/fasted 103.4%). Median T
max was slightly delayed for the fed condition compared to the fasted condition (3.0 versus 2.0 hours). There is not expected to be a clinically relevant food effect with ravidasvir. Ravida can be taken with or without food.
Distribution: Ravidasvir is highly bound to plasma proteins, with an estimated fraction unbound of 1.9%, and is not widely distributed to and bound in extravascular tissues. The apparent volume of distribution (Vz/F) values were approximately 100 L at all dose levels and independent of the administered dose.
In vivo studies in animals show that distribution to the liver, an important target organ for antiviral efficacy, is higher than to plasma.
Biotransformation: Metabolism in hepatic microsomes from all species was negligible, and oxidative metabolism of ravidasvir by human liver S9 fractions did not produce detectable glutathione conjugates. Mono-oxidation was the predominant metabolic pathway in all species studied, however, the pattern of metabolites varied between species.
In vivo human studies indicated that ravidasvir was metabolically very stable, with only modest (~2%) metabolite formation detected. The most abundant metabolites in humans (M6 and M7, both of minor importance) resulted from mono-oxidation of ravidasvir.
Ravidasvir is not a substrate for the transport proteins OATP1B1, OATP1B3, or BCRP but is a substrate for P-gp. There is low likelihood that cytochrome P450 inhibitors or inducers would have a clinically meaningful effect on ravidasvir levels.
Elimination: Biliary excretion of ravidasvir appears to be the primary route of elimination of the absorbed dose, while renal excretion appears to be negligible. Following oral administration of ascending single doses in healthy volunteers, the relationship between AUC
0-∞ and dose was linear indicating that the clearance for ravidasvir is independent of the administered dose.
In healthy volunteers, when 320 mg ravidasvir was administered once daily for 5 days, mean AUC
0-∞ and AUCτ values were similar on Days 1 and 5, and resultant estimates for apparent clearance were nearly identical on Days 1 and 5, indicating that dosing for 5 days does not lead to either significant accumulation or induced elimination of ravidasvir. The pharmacokinetic profile supports dosing once a day.
Pharmacokinetic/pharmacodynamic relationship: HCV RNA levels were measured in chronic HCV-infected subjects dosed with 40 to 240 mg ravidasvir once daily for 3 days. HCV RNA levels rapidly declined from baseline in all cohorts with mean maximal reductions of 3.2, 3.5, 3.5 and 3.8 log
10 IU/mL for the 40, 80, 160 mg and 240 mg doses, respectively. The HCV reductions for the 3 higher doses (3.5 to 3.8 log
10 IU/mL) suggest that ravidasvir doses ≥80 mg once daily are near the top of the efficacy dose-response curve in HCV subjects. Plasma levels well above EC
50 and EC
90 were achieved with once daily dosing, leading to a reduction of viral load in all tested genotypes.
Linearity: The relationship of C
max and AUC to the dose appears linear in the dose range tested in healthy volunteers (80 mg to 320 mg) and HCV subjects (40 mg to 240 mg).
Pharmacokinetics in special populations: No specific pharmacokinetic studies have been conducted in special populations.
Race and gender: No clinically relevant pharmacokinetic differences due to race or gender have been identified for ravidasvir.
Toxicology: Preclinical Safety Data: In repeat toxicity studies, ravidasvir was well tolerated in the rat. Reversible effects of increased organ weight and ratios of adrenal glands, microvesicular vacuolation and diffuse hypertrophy of the zona fasciculata in the adrenal glands were observed. These were associated with increases in cholesterol, low-density lipoprotein and triglycerides. This was observed at the highest dose of 750 mg/kg/day. The no observed adverse effect level (NOAEL) of ravidasvir in rats was established at 300 mg/kg/day, at which AUC
0-24 was approximately 7.6 times the clinical AUC
0-24 at 200 mg. In the monkey, only mild fecal changes (discolored, loose, soft and mucoid stools) were observed at the dose of 500 mg/kg/day. The NOAEL of ravidasvir in monkeys was considered to be 500 mg/kg/day, at which AUC
0-24 was 0.8 times and 1.4 times in males and females, respectively, the clinical AUC
0-24 at 200 mg.
Ravidasvir was not genotoxic in a battery of
in vitro or
in vivo assays, including bacterial mutagenicity, chromosome aberration using human peripheral blood lymphocytes and
in vivo rat micronucleus assays.
Carcinogenicity studies with ravidasvir have not been conducted. No evidence of mutagenic or clastogenic potential was observed in two
in vitro tests (Ames bacterial mutagenicity, Mammalian Chromosomal Aberration Assay inhuman lymphocytes) or in an
in vivo oral micronucleus study in the rat.
In animal reproduction studies, ravidasvir had no effects on fertility, embryofoetal development, lactation and postnatal development or sexual maturation at any dose (maximum 750 mg/kg/day) when administered orally to rats. However in rabbits, ravidasvir produced embryotoxicity and skeletal abnormalities at doses ≥100 mg/kg/day. Based on these teratogenic effects, the NOAEL for embryofoetal development in the rabbit was considered to be 25 mg/kg/day, at which the AUC
last was at least 1.7 times the clinical AUC
0-24 at 200 mg. In view of these effects, Ravida is not recommended in pregnancy and, based on the possible excretion of ravidasvir in milk, breast-feeding is not recommended when taking Ravida.
Ravidasvir had no effects on the eyes or skin of pigmented rats in a definitive phototoxicity study at doses up to 750 mg/kg/day and is therefore considered not to be phototoxic.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image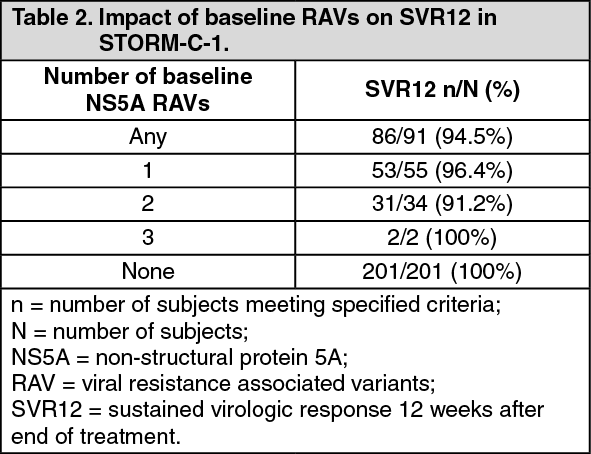 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image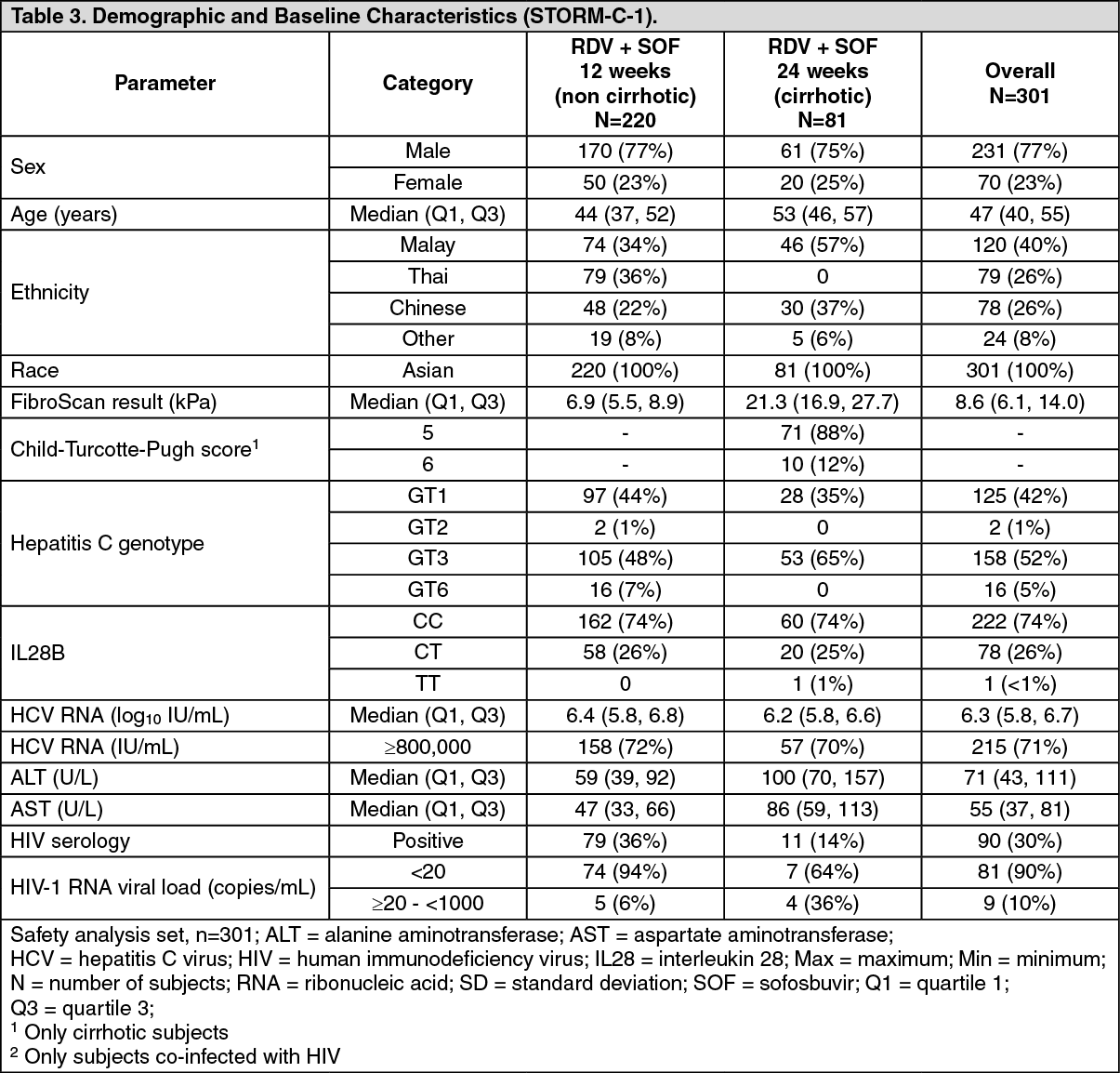 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image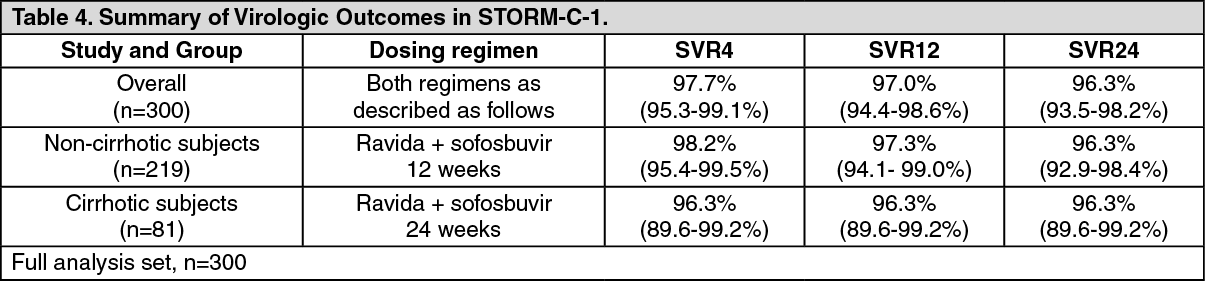 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image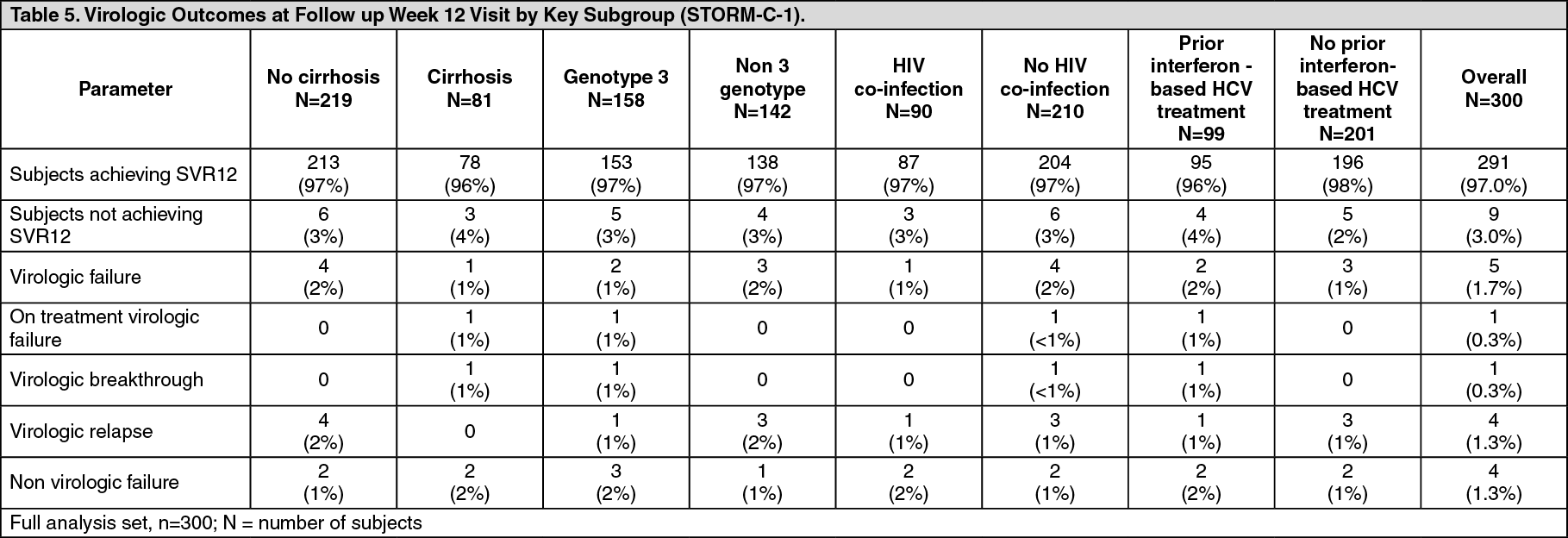 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image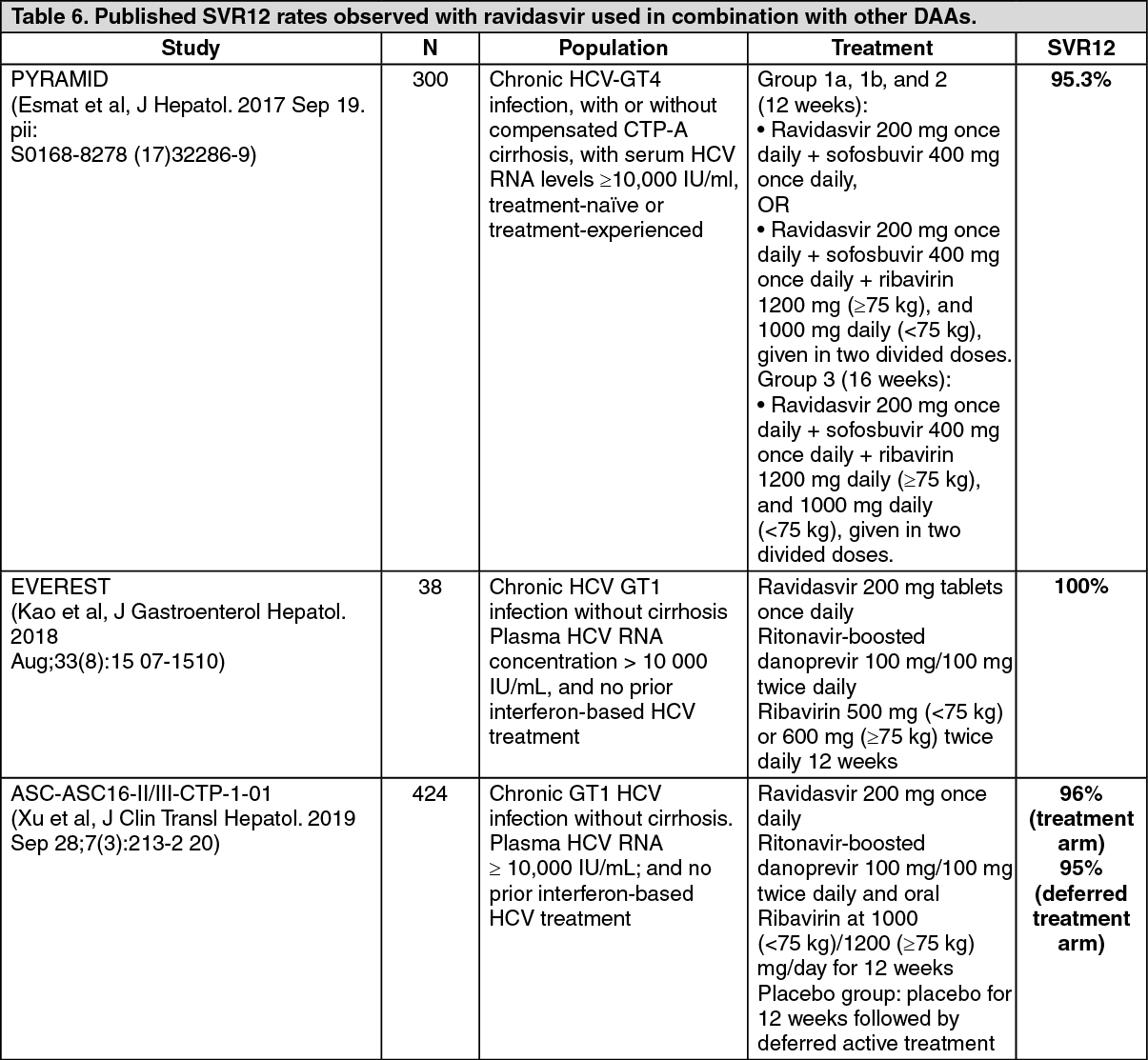 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
