Each ml contains 1.0mg of Cisplatin.
One vial of 50ml of concentrate contains 50mg of Cisplatin Injection.
Description after Dilution: Dilution in NaCl Solution 0.9% - A clear colourless to slightly pale yellow solution.
Dilution in mixture of NaCl Solution 0.9% and glucose Solution 5.0% (1:1) - A clear colourless to slightly pale yellow solution.
Pharmacotherapeutic Group: Other antineoplastic agents, Platinum compounds. ATC Code: L01XA01.
Pharmacology: Pharmacodynamics: Cisplatin is an inorganic compound which contains a heavy metal [cis-diamminedichloridoplatinum (II)]. It inhibits DNA-synthesis by the formation of DNA cross-links. Protein and RNA synthesis are inhibited to a lesser extent.
Although the most important mechanism of action seems to be inhibition of DNA synthesis, other mechanisms can also contribute to the antineoplastic activity of cisplatin, including the increase of tumour immunogenicity. The oncolytic properties of cisplatin are comparable to the alkylating agents. Cisplatin also has immunosuppressive, radio sensitising, and antibacterial properties. Cisplatin seems to be cell-cycle non-specific. The cytotoxic action of cisplatin is caused by binding to all DNA-bases, with a preference for the N-7 position of guanine and adenosine.
Pharmacokinetics: After intravenous administration cisplatin quickly distributes across all tissues; cisplatin badly penetrates in the central nervous system. The highest concentrations are reached in the liver, kidneys, bladder, muscle tissue, skin, testes, prostate, pancreas and spleen.
After intravenous administration the elimination of filterable, non-protein bound cisplatin runs biphasic, with an initial and terminal half-life of 10-20 minutes and 32-53 minutes, respectively.
The elimination of the total quantity of platinum runs triphasic with half-lives of 14 minutes, and 274 minute and 53 days respectively.
Cisplatin is bound to plasma proteins for 90%.
The excretion primarily takes place via the urine: 27-43% of the administered dose is recovered in the urine in the first five days after the treatment. Platinum is also excreted in the bile.
Cisplatin may be used single or in combination with other chemotherapeutic agents in the treatment of: Metastatic non-seminomatous germ cell carcinoma.
Advanced stage, refractory ovarian carcinoma.
Advanced stage, refractory bladder carcinoma.
Refractory squamous cell carcinoma of the head and neck.
Cisplatin 1.0 mg/ml concentrate for solution for infusion is to be diluted before administration.
The diluted solution should be administered only intravenously by infusion (see as follows). For administration, any device containing aluminium that may come in contact with cisplatin (sets for intravenous infusion, needles, catheters, syringes) must be avoided.
Adults and children: The cisplatin dosage depends on the primary disease, the expected reaction, and on whether cisplatin is used for monotherapy or as a component of combination chemotherapy. The dosage directions are applicable for both adults and children.
For monotherapy, the following two dosage regimens are recommended: Single dose of 50 to 120 mg/m2 body surface every 3 to 4 weeks; 15 to 20 mg/m2/day for five days, every 3 to 4 weeks.
If cisplatin is used in combination chemotherapy, the dose of cisplatin must be reduced. A typical dose is 20 mg/m2 or more once every 3 to 4 weeks.
For treatment of cervical cancer cisplatin is used in combination with radiotherapy. A typical dose is 40 mg/m2 weekly for 6 weeks.
For warnings and precautions to be considered prior to the start of the next treatment cycle.
In patients with renal dysfunction or bone marrow depression, the dose should be reduced adequately.
Route of Administration: The cisplatin solution for infusion prepared according to instructions should be administered by intravenous infusion over a period of 6 to 8 hours.
Adequate hydration must be maintained from 2 to 12 hours prior to administration until minimum 6 hours after the administration of cisplatin. Hydration is necessary to cause sufficient diuresis during and after treatment with cisplatin. It is realised by intravenous infusion of one of the following solutions: Sodium chloride solution 0.9%; Mixture of sodium chloride solution 0.9% and glucose solution 5% (1:1).
Hydration prior to treatment with cisplatin: Intravenous infusion of 100 to 200 ml/hour for a period of 6 to 12 hours, with a total amount of at least 1L.
Hydration after termination of the administration of cisplatin: Intravenous infusion of another 2 litres at a rate of 100 to 200 ml per hour for a period of 6 to 12 hours.
Forced diuresis may be required should the urine secretion be less than 100 to 200 ml/hour after hydration. Forced diuresis may be realised by intravenously administering 37.5g mannitol as a 10% solution (375 ml mannitol solution 10%), or by administration of a diuretic if the kidney functions are normal.
Mode of administration: Intravenous Administration.
Symptoms of overdose involve mentioned side effects in an excessive manner.
Efficient hydration and osmotic diuresis can aid in reduction of toxicity, provided this is applied immediately after overdose.
In case of overdose (=200 mg/m2), direct effects on the respiratory centre are possible, which might result in life threatening respiratory disorders and acid base equilibrium disturbance due to passage of the blood brain barrier.
An acute overdose of Cisplatin may result in renal failure, liver failure, deafness, ocular toxicity (including detachment of the retina), significant myelosuppression, untreatable nausea and vomiting and/or neuritis. An overdose may be fatal.
There is no specific antidote in the event of an overdose of Cisplatin. Even if haemodialysis is initiated 4 hours after the overdose it has little effect on the elimination of cisplatin from the body following a strong and rapid fixation of Cisplatin to proteins.
Treatment in the event of an overdose consists of general support measures.
Convulsions may be treated with appropriate anticonvulsants. Renal function, cardiovascular function and blood counts should be monitored daily in order to assess the potential toxicity to these systems. Serum magnesium and calcium levels should be carefully monitored as should symptoms and signs of voluntary muscle irritability. If symptomatic tetany develops, electrolyte supplements should be administered. Serum liver enzymes and uric acid should also be monitored daily after an acute overdose.
If fever develops during prolonged myelosuppression, appropriate presumptive antibiotic coverage should be instilled after cultures have been obtained.
Cisplatin is contraindicated in patients: With hypersensitivity to cisplatin or other platinum compounds or to any of the excipients;
With pre-existing renal impairment*;
In dehydrated condition (pre- and post-hydration is required to prevent serious renal dysfunction);
With myelosuppression;
With pre-existing hearing impairment*;
With neuropathy caused by cisplatin;
Who are breast-feeding;
In combination with live vaccines, including yellow fever vaccine;
In combination with phenytoin in prophylactic use.
* Due to the fact that cisplatin is nephrotoxic and neurotoxic (in particular ototoxic). These toxicities may be cumulative if disorders of this type pre-exist.
This cytostatic agent had a more marked toxicity than is usually found in antineoplastic chemotherapy.
Renal toxicity, which is above-all cumulative, is severe and requires particular precautions during administration.
Nausea and vomiting may be intense and require adequate antiemetic treatment. Close supervision must also be carried out with regard to ototoxicity, myelodepression and anaphylactic reactions.
CAUTION: CYTOTOXIC AGENT.
Cisplatin reacts with metallic aluminium to form a black precipitate of platinum. All aluminium containing IV sets, needles, catheters and syringes should be avoided.
Cisplatin may only be administered under the supervision of a physician qualified in oncology with experience in the use of antineoplastic chemotherapy.
Appropriate monitoring and management of the treatment and its complications are only possible if adequate diagnosis and exact treatment conditions are available.
Cisplatin is proven to be cumulative ototoxic, nephrotoxic, and neurotoxic. The toxicity caused by cisplatin may be amplified by the combined use with other medicinal products, which are toxic for the said organs or systems.
Male and female patients during and for at least 6 months after the treatment with cisplatin.
Nephrotoxicity: Cisplatin causes severe cumulative nephrotoxicity. A urine output of 100 mL/hour or greater will tend to minimize cisplatin nephrotoxicity. This can be accomplished by prehydration with 2 litres of an appropriate intravenous solution, and similar post cisplatin hydration (recommended 2,500 mL/m2/24 hours). If vigorous hydration is insufficient to maintain adequate urinary output, an osmotic diuretic may be administered (eg, mannitol). Hyperuricaemia and hyperalbuminaemia may predispose to cisplatin-induced nephrotoxicity.
Neuropathies: Severe cases of neuropathies have been reported.
These neuropathies may be irreversible and may manifest by paresthesia, areflexia and a proprioceptive loss and a sensation of vibrations. A loss of motor function has also been reported. A neurologic examination must be carried out at regular intervals. Special caution must be exercised for patients with peripheral neuropathy not caused by cisplatin.
Ototoxicity: Ototoxicity has been observed in up to 31% of patients treated with a single dose of cisplatin 50mg/m2, and is manifested by tinnitus and/or hearing loss in the high frequency range (4000 to 8000Hz). Decreased ability to hear conversational tones may occur occasionally. Ototoxic effect may be more pronounced in children receiving cisplatin. Hearing loss can be unilateral or bilateral and tends to become more frequent and severe with repeated doses; however, deafness after initial dose of cisplatin has been reported rarely. Ototoxicity may be enhanced with prior simultaneous cranial irradiation and may be related to peak plasma concentration of cisplatin. It is unclear whether cisplatin induced ototoxicity is reversible. Careful monitoring by audiometry should be performed prior to initiation of therapy and prior to subsequent doses of cisplatin. Vestibular toxicity has also been reported.
Before, during and after administration of cisplatin, the following parameters resp. organ functions must be determined: Renal function; Hepatic function; Haematopoiesis functions (number of red and white blood cells and blood platelets); Serum electrolytes (calcium, sodium, potassium, magnesium).
These examinations must be repeated every week over the entire duration of the treatment with cisplatin. Repeating administration of cisplatin must be delayed until normal values are achieved for the following parameters: Serum creatinine < 130 μmol/l rsp. 1.5 mg/dl,
Urea < 25 mg/dl,
White blood cells > 4.000/μl resp. > 4.0 x 109/l,
Blood platelets > 100.000/μl resp. > 100 x 109/l.
Audiogram: results within the normal range.
Allergic phenomena: As with other platinum-based products, hypersensitivity reactions appearing in most cases during perfusion may occur, and necessitate discontinuation of the perfusion and an appropriate symptomatic treatment. Cross reactions, sometimes fatal, have been reported with all the platinum compounds (see Contraindications and Side Effects). Anaphylactic-like reactions to cisplatin have been observed. These reactions can be controlled by administration of antihistamines, adrenaline and/or glucocorticoids.
Hepatic function and haematological formula: The haematological formula and the hepatic function must be monitored at regular intervals.
Carcinogenic potential: In humans, in the rare cases the appearance of acute leukaemia has coincided with use of Cisplatin, which was in general associated with other leukaemogenic agents. Cisplatin is a bacterial mutagen and causes chromosome aberrations in cultures on animal cells. Carcinogenicity is possible but has not been demonstrated. Cisplatin is teratogenetic and embryo toxic in mice.
Injection site reactions: Injection site reactions may occur during the administration of cisplatin. Given the possibility of extravasation, it is recommended to closely monitor the infusion site for possible infiltration during drug administration. A specific treatment for extravasation reactions is unknown at this time.
Preparation of the intravenous solution: As with all other potentially toxic products, precautions are essential when handling the cisplatin solution. Skin lesions are possible in the event of accidental exposure to the product. It is advisable to wear gloves. In the event the cisplatin solution comes into contact with the skin or mucous membranes, wash the skin or mucous membranes vigorously with soap and water.
Conforming to the procedures appropriate for the manipulation and elimination of cytostatic agents is recommended.
Before administering the solution to the patient, verify the clarity of the solution and the absence of particles.
Special care is required for patients with acute bacterial or viral infections.
Male and female patients have to use effective contraception during and for at least 6 months after the treatment with cisplatin.
Pregnancy and lactation: Cisplatin may be toxic to the foetus when administered to a pregnant woman. Animal studies have shown reproductive toxicity and transplacental carcinogenity.
During treatment with Cisplatin and for a minimum of the following 6 months, appropriate measures must be taken to avoid pregnancy; this applies to patients of both sexes.
Genetic consultation is recommended if the patient wishes to have children after ending the treatment.
Since a treatment with cisplatin may cause irreversible infertility, it is recommended that men, who wish to become fathers in the future, ask for advice regarding cryoconservation of their sperm prior to treatment.
Breast-feeding: Cisplatin is excreted in breast milk. Patients treated with cisplatin must not breastfeed.
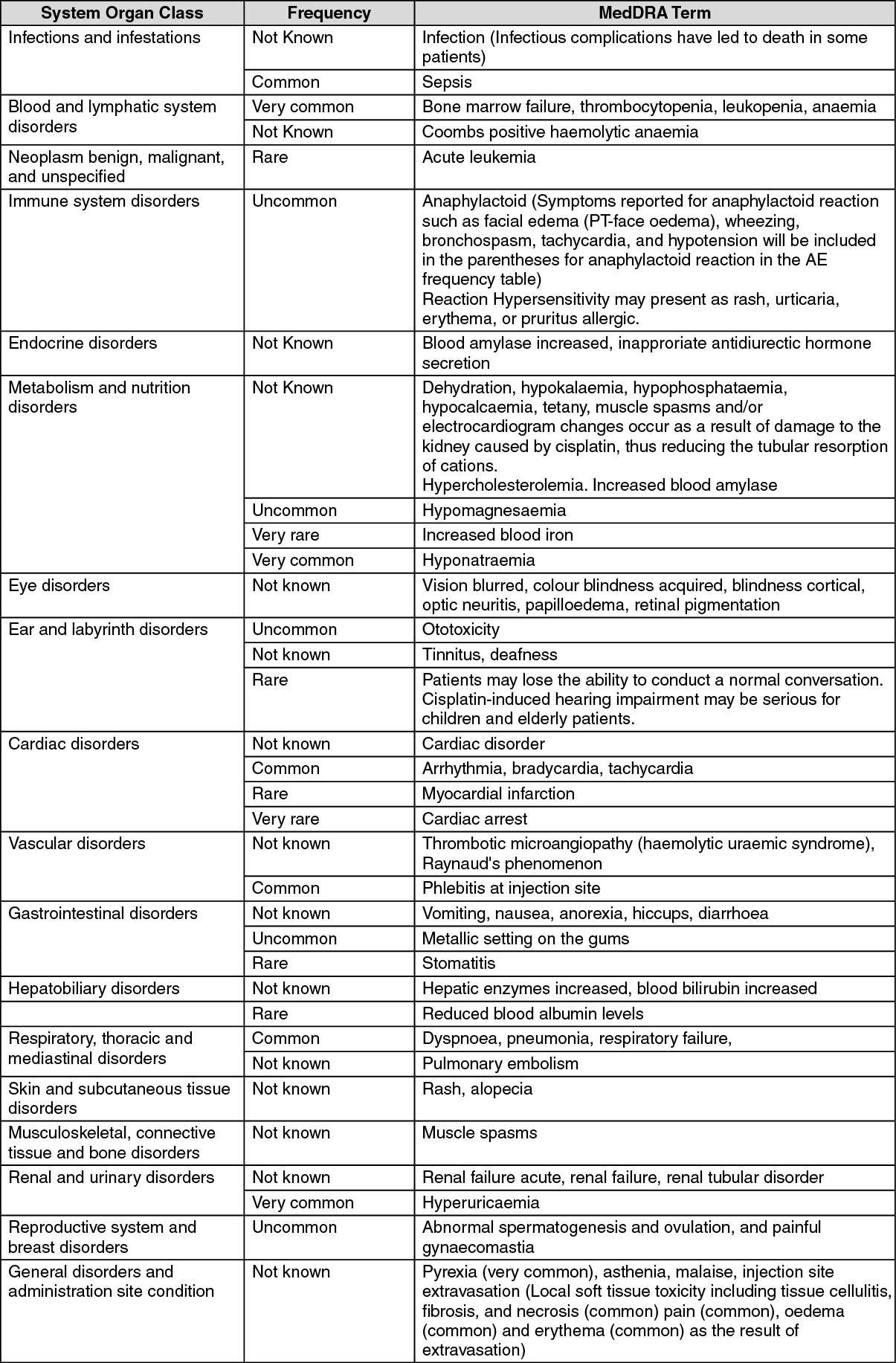
Undesirable effects depend on the used dose and may have cumulative effects.
The most frequently reported adverse events (>10%) of cisplatin were haematological (leukopenia, thrombocytopenia and anaemia), gastrointestinal (anorexia, nausea, vomiting and diarrhoea), ear disorders (hearing impairment), renal disorders (renal failure, nephrotoxicity, hyperuricaemia) and fever.
Serious toxic effects on the kidneys, bone marrow and ears have been reported in up to about one third of patients given a single dose of cisplatin; the effects are generally dose-related and cumulative. Ototoxicity may be more severe in children.
Hypersensitivity may present as rash, urticaria, erythema, or pruritus allergic. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Simultaneous use of myelosuppressives or radiation will boost the effects of cisplatin's myelosuppressive activity. The occurrence of nephrotoxicity caused by cisplatin may be intensified by concomitant treatment with antihypertensives containing furosemide, hydralazine, diazoxide, and propranolol.
Nephrotoxic substances: Concomitant administration of nephrotoxic (e.g. cephalosporins, aminoglycosides or Amphotericin B or contrast media) or ototoxic (e.g. aminoglycosides) medicinal products will potentiate the toxic effect of cisplatin on the kidneys. During or after treatment with cisplatin caution is advised with predominantly renally eliminated substances, e.g. cytostatic agents such as bleomycin and methotrexate, because of potentially reduced renal elimination.
Cisplatin given in combination with bleomycin and vinblastin can lead to a Raynaud-phenomenon. The renal toxicity of ifosfamide may be greater when used with cisplatin or in patients who have previously been given cisplatin.
Reduction of the blood's lithium values was noticed in a few cases after treatment with cisplatin combined with bleomycin and etoposide. It is therefore recommended to monitor the lithium values. It may be required to adjust the dosage of allopurinol, colchicine, probenecid, or sulfinpyrazone if used together with cisplatin, since cisplatin causes an increase in serum uric acid concentration. Cisplatin given in combination with bleomycin and vinblastin can lead to a Raynaud-phenomenon. In a study of cancer patients with metastatic or advanced tumors, docetaxel in combination with cisplatin induced more severe neurotoxic effects (dose-related and sensoric) than either drug as a single agent in similar doses.
Chelating agents like penicillamine may diminish the effectiveness of cisplatin.
In concomitant use of cisplatin and ciclosporin the excessive immunosuppression with risk of lymphoproliferation is to be taken into consideration.
Ototoxic substances: Concomitant administration of ototoxic (e.g. aminoglycosides, loop diuretics) medicinal products will potentiate the toxic effect of cisplatin on auditory function. Except for patients receiving doses of cisplatin exceeding 60 mg/m2, whose urine secretion is less than 1000 ml per 24 hours, no forced diuresis with loop diuretics should be applied in view of possible damage to the kidney tract and ototoxicity.
Ifosfamide may increase hearing loss due to cisplatin.
Weakened live vaccines: Yellow fever vaccine is strictly contraindicated because of the risk of fatal systemic vaccinal disease (see Contraindications). In view of the risk of generalised illness, it is advisable to use an inactive vaccine if available.
Oral anticoagulants: In the event of simultaneous use of oral anticoagulants, it is advisable regularly to check the INR.
Antihistamines, Phenothiazines and others: Simultaneous use of antihistamines, buclizine, cyclizine, loxapine, meclozine, phenothiazines, thioxanthenes or trimethobenzamides may mask ototoxicity symptoms (such as dizziness and tinnitus).
Anticonvulsive substances: Serum concentrations of anticonvulsive medicines may remain at subtherapeutic levels during treatment with cisplatin. Cisplatin may reduce the absorption of phenytoin resulting in reduced epilepsy control when phenytoin is given as current treatment. During cisplatin therapy starting a new anticonvulsivant treatment with phenytoin is strictly contraindicated (see Contraindications).
Pyridoxine + altretamine combination: During a randomised study of the treatment of advanced ovarian cancer, the response time was unfavourably affected when pyridoxine was used in combination with altretamine (hexamethylmelamine) and Cisplatin.
Paclitaxel: Treatment with cisplatin prior to an infusion with paclitaxel may reduce the clearance of paclitaxel by 33% and therefore can intensify neurotoxicity.
Incompatibilities: Do not bring in contact with aluminium. Cisplatin reacts with metal aluminium to form a black precipitate of platinum. All aluminium-containing IV sets, needles, catheters and syringes should be avoided. Cisplatin decomposes with solution in media with low chloride content; the chloride concentration should at least be equivalent to 0.45% of sodium chloride.
In the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products.
Antioxidants (such as sodium metabisulphite), bicarbonates (sodium bicarbonate), sulfates, fluorouracil and paclitaxel may inactivate cisplatin in infusion systems.
Storage condition for unopened vial: Store below 30°C.
Store in the original package in order to protect from light.
Storages condition with dilution: 0.9 % w/v Sodium Chloride: Store up to 24 hours at room temperature 20°C-25°C when store in the infusion bag. The diluted solution should be protected from light. Do not store diluted solutions in the refrigerator or freezer.
Mixture of 0.9 % w/v Sodium Chloride and 5 % w/v Glucose Injection (1:1): Store up to 24 hours at room temperature 20ºC-25°C when store in the infusion bag. The diluted solution should be protected from light. Do not store diluted solutions in the refrigerator or freezer.
Shelf-Life: Unopened vial: 2 years.
After opening of the vial: Each vial is for single use and should be used immediately after opening. If not used immediately, in-use storage times and conditions are the responsibility of the user.
Once added to the infusion bag: From a microbiological point of view, reconstitution/dilution must take place in controlled and aseptic conditions and the medicinal product should be used immediately. If not used immediately, in-use storage times and conditions are the responsibility of the user.
Once added as recommended into the infusion bag, the Cisplatin Injection, if stored between 20ºC-25°C, is stable for 24 hours. It should be used within 24 hours (including the one hour infusion IV administration).
L01XA01 - cisplatin ; Belongs to the class of platinum-containing antineoplastic agents. Used in the treatment of cancer.
Platol soln for infusion 50 mg/50 mL
1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
