300 mg: Each capsule contains: Gabapentin 300 mg.
400 mg: Each capsule contains: Gabapentin 400mg.
600 mg: Each film-coated tablet contains Gabapentin 600 mg.
Excipients/Inactive Ingredients: 600 mg: Maize starch, Crospovidone, Copovidone, Isopropyl Alcohol, Cellulose, microcrystalline (Avicel PH102 & Ceolus KG100), Magnesium stearate, Opadry White YS-1-18111 and Methylene Chloride.
Pharmacology: Pharmacodynamics: 300 & 400 mg: Gabapentin is structurally related to the neurotransmitter GABA (gamma-aminobutyric acid) but it does not modify GABAA or GABAB radioligand binding, it is not converted metabolically into GABA or a GABA agonist, and it is not an inhibitor of GABA uptake or degradation.
Gabapentin was tested in radioligand binding assays at concentrations up to 100 μM and did not exhibit affinity for a number of other common receptor sites, including benzodiazepine, glutamate, N-methyl-D-aspartate (NMDA), quisqualate, kainate, atrychnine-insensitive or strychnine-sensitive glycine, alpha 1, alpha 2, or beta adrenergic, adenosine A1 or A2, cholinergic muscarinic or nicotinic, dopamine D1 or D2, histamine H1, serotonin S1 or S2, opiate mu, delta or kappa, cannabinoid 1, voltage-sensitive calcium channel sites labeled with nitrendipine or diltiazem, or at voltage-sensitive sodium channel sites labeled with batrachotoxinin A 20-alpha-benzoate. Furthermore, Gabapentin did not alter the cellular uptake of dopamine, noradrenaline, or serotonin.
600 mg: Gabapentin is structurally related to the neurotransmitter GABA (gamma-aminobutyric acid) but its mechanism of action is different from that of several other active substances that interact with GABA synapses including valproate, barbiturates, benzodiazepines, GABA transaminase inhibitors, GABA uptake inhibitors, GABA agonists, and GABA prodrugs. In vitro studies with radiolabeled gabapentin have characterized a novel peptide binding site in rat brain tissues including neocortex and hippocampus that may relate to anticonvulsant and analgesic activity of gabapentin and its structural derivatives. The binding site for gabapentin has been identified as the alpha 2-delta subunit of voltagegated calcium channels.
Gabapentin at relevant concentrations does not bind to other common drug or neurotransmitter receptors of the brain including GABAA, GABAB, benzodiazepine, glutamate, glycine or N-methyl-d-aspartate receptors.
Gabapentin does not interact with sodium channels in vitro and so differs from phenytoin and carbamazepine. Gabapentin partially reduces responses to the glutamate agonist Nmethyl-D-aspartate (NMDA) in some test systems in vitro, but only at concentrations greater than 100 μm, which are not achieved in vivo. Gabapentin slightly reduces the release of monoamine neurotransmitters in vitro.
Pharmacokinetics: 300 & 400 mg: All pharmacological actions following Gabapentin administration are due to the activity of the parent compound; Gabapentin is not appreciably metabolized in humans.
Absorption: 300 & 400 mg: Gabapentin bioavailability is not dose proportional; i.e., as dose is increased, bioavailability decreases. Bioavailability of Gabapentin is approximately 60%, 47%, 34%, 33%, and 27% following 900, 1200,, 2400, 3600, and 4800 mg/day given in 3 divided doses, respectively. Food has only a slight effect on the rate and extent of absorption of Gabapentin (14% increase in AUC and Cmax).
600 mg: Following oral administration, peak plasma gabapentin concentrations are observed within 2 to 3 hours. Gabapentin bioavailability (fraction of dose absorbed) tends to decrease with increasing dose. Absolute bioavailability of a 300 mg capsule is approximately 60 %. Food, including a high-fat diet, has no significant effect on gabapentin pharmacokinetics. Gabapentin pharmacokinetics are not affected by repeated administration.
Distribution: 300 & 400 mg: Less than 3% of Gabapentin circulates bound to plasma protein. The apparent volume of distribution of Gabapentin after 150 mg intravenous administration is 58±6 L (Mean ±SD). In patients with epilepsy, steady-state predose (Cmin) concentrations of Gabapentin in cerebrospinal fluid were approximately 20% of the corresponding plasma concentrations.
600 mg: Gabapentin is not bound to plasma proteins and has a volume of distribution equal to 57.7 litres. In patients with epilepsy, gabapentin concentrations in cerebrospinal fluid (CSF) are approximately 20 % of corresponding steady-state trough plasma concentrations.
Gabapentin is present in the breast milk of breast-feeding women.
Metabolism: There is no evidence of Gabapentin metabolism in humans. Gabapentin does not induce hepatic mixed function oxidase enzymes responsible for drug metabolism.
Elimination: 300 & 400 mg: Gabapentin is eliminated from the systemic circulation by renal excretion as unchanged drug.
Gabapentin elimination half-life is 5 to 7 hours and is unaltered by dose or following multiple dosing. Gabapentin elimination rate constant, plasma clearance, and renal clearance are directly proportional to creatinine clearance.
600 mg: Gabapentin is eliminated unchanged solely by renal excretion. The elimination half-life of gabapentin is independent of dose and averages 5 to 7 hours.
In elderly patients, and in patients with impaired renal function, gabapentin plasma clearance is reduced. Gabapentin elimination-rate constant, plasma clearance, and renal clearance are directly proportional to creatinine clearacne.
Gabapentin is removed from plasma by haemodialysis. Dosage adjustment in patients with compromised renal function or undergoing haemodialysis is recommended.
Linearity/Non-linearity: 600 mg: Gabapentin bioavailability (fraction of dose absorbed) decreases with increasing dose which imparts non-linearity to pharmacokinetic parameters which include the bioavailability parameter (F) e.g. Ae%, CL/F, Vd/F. Elimination pharmacokinetics (pharmacokinetic parameters which do not include F such as CLr and T1/2), are best described by linear pharmacokinetics. Steady state plasma gabapentin concentrations are predictable from single-dose data.
Epilepsy: Gabapentin is indicated as adjunctive therapy in the treatment of partial seizures with and without secondary generalization in adults and children aged ≥ 3 years.
Safety and effectiveness for adjunctive therapy in pediatric patients below the age of 3 years have not been established.
Treatment of peripheral neuropathic pain: Gabapentin is indicated for the treatment of peripheral neuropathic pain such as painful diabetic neuropathy, post-herpetic and trigeminal neuralgia in adults ≥ 18 years.
Safety and effectiveness in patients below the age of 18 years have not been established.
300 & 400 mg: General: Gabapentin is given orally with or without food.
When in the judgement of the clinician there is a need for dose reduction, discontinuation, or substitution with an alternative medication, this should be done gradually over a minimum of one week.
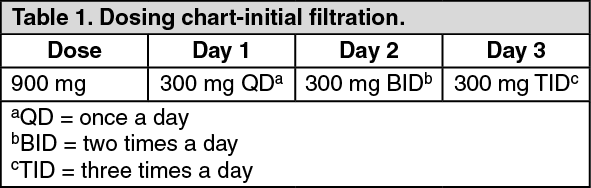
Epilepsy: Adults and pediatric patients over 12 years of age: The effective dose of Gabapentin is 900 to 3600 mg/day. Therapy may be initiated by administering 300mg three times a day (TID) on Day 1, or by titrating the dose as described in Table 1. Thereafter, the dose can be increased in three equally divided doses upto a maximum dose of 3600 mg/day. Dosages upto 4800 mg/day have been well tolerated in long-term open-label clinical studies. The maximum time between doses in the three times a day (TID) schedule should not exceed 12 hours to prevent breakthrough convulsions. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pediatric Patients Age 3-12 years: The starting dose should range from 10-15 mg/kg/day in 3 equally divided doses, and the effective dose reached by upward titration over a period of approximately 3 days. The effective dose of Gabapentin in patients 5 years of age and older is 25-35 mg/kg/day and given in divided doses (three times a day). The effective dose in pediatric patients aged 3 to less than 5 years is 40 mg/kg/day and given in divided doses (three times a day). Dosages upto 50 mg/kg/day have been well tolerated in longterm clinical study. The maximum time interval between doses should not exceed 12 hours. It is not necessary to monitor Gabapentin plasma concentrations to optimize Gabapentin therapy. Further, Gabapentin may be used in combination with other antiepileptic drugs without concern for alteration of the plasma concentrations of Gabapentin or serum concentrations of other antiepileptic drugs.
Neuropathic Pain in Adults: The starting dose is 900 mg/day given as three equally divided doses, and increased if necessary, based on response, upto a maximum dose of 3600 mg/day. Therapy should be initiated by titrating the dose as described in Table 1.
Dosage adjustment in Renal Impairment function for patients with Neuropathic pain or Epilepsy: Dosage adjustment is recommended in patients with compromised renal function as described in Table 2 and or those undergoing hemodialysis. (See Table 2.)
Click on icon to see table/diagram/image
Dosage adjustment in patients undergoing Hemodialysis: For patients undergoing hemodialysis who have never received gabapentin, a loading dose of 300 to 400mg is recommended, then 200 to 300 mg of gabapentin following each 4 hours of hemodialysis.
600 mg: Posology and method of administration: Gabapentin can be given orally with or without food. When in the judgment of the clinician there is a need for dose reduction, discontinuation, or substitution with an alternative medication, this should be done gradually over a minimum of one week. (See Table 3.)
Click on icon to see table/diagram/image
Epilepsy: Adults and Children >12years: The effective dosing range was 900 to 3600 mg/day. Therapy may be initiated by titrating the dose as described in Table 1 or by administering 300 mg three times a day (TID) on Day 1. Thereafter, based on individual patient response and tolerability, the dose can be further increased in 300 mg/day increments every 2-3 days up to a maximum dose of 3600 mg/day. Dosages up to 4800 mg/day have been well tolerated in long–term open-label clinical studies. The maximum time interval between doses in the three times a day (TID) schedule should not exceed 12 hours to prevent breakthrough convulsions.
Children 3-12 years: The starting dose should range from 10 to 15 mg/kg/day given in equally divided doses (3 times a day), and the effective dose is reached by upward titration over a period of approximately three days. The effective dose of gabapentin in children aged 6 years and older is 25 to 35 mg/kg/day in equally divided doses (3 times a day). The effective dose of gabapentin in children aged 3 to < 5 years is 40 mg/kg/ day in equally divided doses (3 times a day). Dosages up to 50 mg/kg/day have been well tolerated in longterm clinical study. The maximum time interval between doses should not exceed 12 hours.
It is not necessary to monitor Gabapentin plasma concentrations to optimize Gabapentin therapy. Further, Gabapentin may be used in combination with other antiepileptic drugs without concern for alteration of the plasma concentrations of Gabapentin or serum concentrations of other antiepileptic drugs.
Peripheral neuropathic pain: Adults: The starting dose is 900 mg/day given as three equally divided doses and increased if necessary, based on individual patient response and tolerability, the maximum dose of 3600 mg/day.
Dosage Adjustment in Impaired Renal Function fort Patients with Neuropathic pain or Epilepsy: Dosage adjustment is recommended in patients with compromised renal function as described in Table 4 and/ or those undergoing haemodialysis. (See Table 4.)
Click on icon to see table/diagram/image
Dosage adjustment in patients undergoing haemodialysis: For anuric patients undergoing haemodialysis who have never received gabapentin, a loading dose of 300 to 400 mg is recommended, then 200 to 300 mg of gabapentin following each 4 hours of haemodialysis, is recommended.
Mode of administration: Oral administration.
Acute, life-threatening toxicity may not occur with gabapentin overdoses of up to 49 g.
Symptoms of the overdoses included dizziness, double vision, slurred speech, drowsiness, lethargy and mild diarrhoea. All patients recovered fully with supportive care. Reduced absorption of gabapentin at higher doses may limit drug absorption at the time of overdosing and, hence, minimize toxicity from overdoses.
Although gabapentin can be removed by haemodialysis, based on prior experience it is usually not required. However, in patients with severe renal impairment, haemodialysis may be indicated.
300 & 400 mg: An oral lethal dose of gabapentin was not identified in mice and rats given doses as high as 8000 mg/kg. Signs of acute toxicity in animals included ataxis, labored breathing, ptosis, hypoactivity, or excitation.
Hypersensitivity to the active substance or to any of the excipients.
General: Although there is no evidence of rebound seizures with gabapentin, abrupt withdrawal of anticonvulsants in epileptic patients may precipitate status epilepticus.
Gabapentin is not generally considered effective in the treatment of absence seizures.
Patients who require concomitant treatment with morphine may experience increases in gabapentin concentrations.
Patients should be carefully observed for signs of CNS depression, such as somnolence, and the doses of gabapentin or morphine should be reduced appropriately.
Information for Patients: To assure safe and effective use of gabapentin, the following information and instructions should be given to patients: Inform the physician about any prescription or nonprescription medications, alcohol or drugs the patient is currently taking or planning to take during treatment with gabapentin.
The patient should inform the physician if the patient is pregnant, or if the patient is planning to become pregnant, or if the patient becomes pregnant while they are taking gabapentin.
Gabapentin is excreted in human milk, and the effect on the nursing infant is unknown. The patient should inform the physician if they are breast feeding an infant.
The patient should not allow more than 12 hours between gabapentin doses to prevent breakthrough convulsions.
Effects on the ability to drive or operate machinery: Gabapentin may impair the patient's ability to drive a car or operate potentially dangerous machinery. Patients should be advised not to drive a car or operate potentially dangerous machinery. Until it is known that this medication does not affect their ability to engage in these activities, do not drive a car or operate potentially dangerous machinery.
Usage in Pregnancy: There are no adequate and well-controlled data from the use of gabapentin in pregnant women. Because animal reproduction studies are not always, predictive of human response, the potential risk for humans is unknown. Gabapentin should not be used during pregnancy unless the potential benefit to the mother clearly outweighs the potential risk to the fetus.
Usage in Nursing Mothers: Gabapentin is excreted in human milk. Because the effect on the breast-fed infant is unknown, caution should be exercised when gabapentin is administered to a breastfeeding mother.
Gabapentin should be used in breast-feeding mothers only if the benefits clearly outweigh the risks.
300 & 400 mg: The adverse reactions in epilepsy (adjunctive and monotherapy) and neuropathic pain have been provided in a single list as follows by class and frequency (very common >1/10), common (>1/100, <1/10), uncommon (>1/1000, <1/100) and rare (>1/10000, <1/1,000).
Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness.
Infections and infestations: Very common: Viral infection. Common: Pneumonia, respiratory infection, urinary tract infection, infection, otitis media.
Blood and the lymphatic system disorders: Common: leucopenia. Rare: thrombocytopenia.
Immune system disorders: Rare: allergic reactions (e.g. urticaria).
Metabolism and Nutrition Disorders: Common: anorexia, increased appetite.
Psychiatric disorders: Common: hostility, confusion and emotional lability, depression, anxiety, nervousness, thinking abnormal. Rare: hallucinations.
Nervous system disorders: Very Common: somnolence, dizziness, ataxia. Common: convulsions, hyperkinesias, dysarthria, amnesia, tremor, insomnia, headache, sensations such as paresthesia, hypaesthesia, coordination abnormal, nystagmus, increased, decreased or absent reflexes. Rare: movement disorders (e.g. choreoathetosis, dyskinesia, dystonia).
Eye disorders: Common: visual disturbances such as ambiyopia, diplopia.
Ear and labyrinth disorders: Common: vertigo. Rare: tinnitus.
Cardiac disorders: Rare: palpitations.
Vascular disorder: Common: hypertension, vasodilatation.
Respiratory, thoracic and mediastinal disorders: Common: dyspnea, bronchitis, pharyngitis, cough, rhinitis.
Gastrointestinal disorders: Common: vomiting, nausea, dental abnormalities, gingivitis, diarrhea, abdominal pain, dyspepsia, constipation, dry mouth or throat, flatulence. Rare: pancreatitis.
Hepatobiliary disorders: Rare: hepatitis, jaundice.
Skin and subcutaneous tissue disorders: Common: facial oedema, purpura most often described as bruises resulting from physical trauma, rash, pruritus, and acne. Rare: Stevens-Johnson syndrome, angioedema, erythema multiforme, alopecia.
Musculoskeletal, connective tissue and bone disorders: Common: arthralgia, myalgia, back pain, twitching.
Renal and urinary disorders: Common: Incontinence. Rare: acute renal failure.
Reproductive system and breast disorders: Common: impotence.
600 mg: The adverse reactions observed during clinical studies conducted in epilepsy adjunctive Therapy frequently occurring treatment-emergent signs and symptoms during placebo controlled studies are summarized as follows: Body as a Whole: Asthenia, malaise, facial edema.
Cardiovascular System: Hypertension.
Digestive System: Flatulence, anorexia, gingivitis.
Hemic/Lymphatic Systems: Purpura most often described as bruises resulting from physical trauma.
Musculoskeletal System: Arthralgia.
Nervous System: Vertigo; hyperkinesia; increased, decreased or absent reflexes; paresthesia, anxiety, hostility.
Respiratory System: Pneumonia.
Urogenital System: Urinary tract infection.
Special Senses: Abnormal vision most often described as a visual disturbance.
Children: The most commonly observed adverse events reported with the use of gabapentin in combination with other antiepileptic drugs in children 3-12 years, not seen in equal frequency among placebo-treated patients, were viral infection, fever, nausea and/or vomiting, and somnolence.
No interaction between Gabapentin and phenobarbital, phenytoin, valproic acid, or carbamazepine has been observed.
Coadministration of Gabapentin with oral contraceptives containing norethindrone and/or ethinyl estradiol, does not influence the steady-state pharmacokinetics of either component.
Coadministration of Gabapentin with antacids containing aluminium and magnesium reduces Gabapentin bioavailability by about 20%. It is recommended that Gabapentin be taken at the earliest two hours following antacid administration.
Renal excretion of Gabapentin is unaltered by probenecid.
A slight decrease in renal excretion of gabapentin that is observed when it is coadministered with cimetidine is not expected to be of clinical importance.
300 & 400 mg: Gabapentin is not appreciably metabolized nor does it interfere with the metabolism of commonly coadministered antiepileptic drugs.
Laboratory tests: False positive readings were reported with the Ames N-Multi-stix SG dipstick test when gabapentin was added to other anticonvulsant drugs. To determine urinary protein, the more specific sulfosalicylic acid precipitation procedure is recommended.
600 mg: Gabapentin steady-state pharmacokinetics are similar for healthy subjects and patients with epilepsy receiving these antiepileptic agents.
Do not store above 30°C.
Shelf-Life: 24 months.
N02BF01 - gabapentin ; Belongs to the class of gabapentinoids. Used to relieve pain and other conditions.
Onegaba cap 300 mg
10 × 10's;3 × 10's
Onegaba cap 400 mg
3 × 10's
Onegaba FC tab 600 mg
3 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image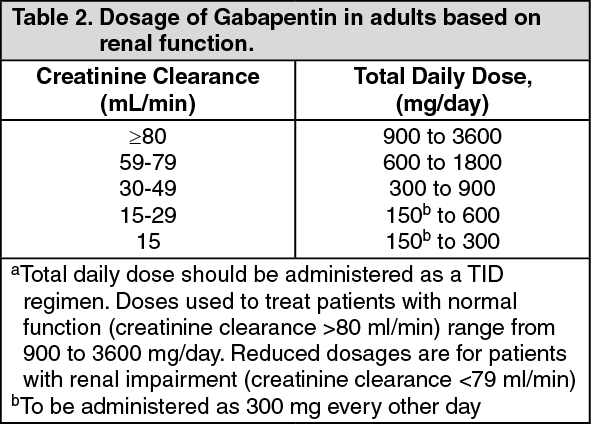 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image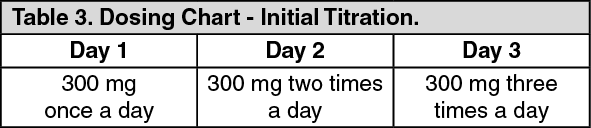 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
