


 Sign Out
Sign Out

Pharmacodynamics: Mechanism of action: NIMEDINE consists of two components: imipenem and cilastatin sodium in a 1:1 ratio by weight.
Imipenem, also referred to as N-formimidoyl-thienamycin, is a semi-synthetic derivative of thienamycin, the parent compound produced by the filamentous bacterium Streptomyces cattleya.
Imipenem exerts its bactericidal activity by inhibiting bacterial cell wall synthesis in Gram-positive and Gram-negative bacteria through binding to penicillin-binding proteins (PBPs).
Cilastatin sodium is a competitive, reversible and specific inhibitor of dehydropeptidase-I, the renal enzyme which metabolizes and inactivates imipenem. It is devoid of intrinsic antibacterial activity and does not affect the antibacterial activity of imipenem.
Pharmacokinetic/Pharmacodynamic (PK/PD) relationship: Similar to other beta-lactam antibacterial agents, the time that imipenem concentrations exceed the MIC (T>MIC) has been shown to best correlate with efficacy.
Mechanism of resistance: Resistance to imipenem may be due to the following: Decreased permeability of the outer membrane of Gram-negative bacteria (due to diminished production of porins).
Imipenem may be actively removed from the cell with an efflux pump.
Reduced affinity of PBPs to imipenem.
Imipenem is stable to hydrolysis by most beta-lactamases, including penicillinases and cephalosporinases produced by gram-positive and gram-negative bacteria, with the exception of relatively rare carbapenem hydrolysing beta-lactamases. Species resistant to other carbapenems do generally express co-resistance to imipenem. There is no target-based cross-resistance between imipenem and agents of the quinolone, aminoglycoside, macrolide and tetracycline classes.
Breakpoints: EUCAST MIC breakpoints for imipenem to separate susceptible (S) pathogens from resistant (R) pathogens are as follows (v 1,1 2010-04-27): Enterobacteriaceae 1: S ≤2 mg/l, R >8 mg/l; Pseudomonas spp. 2: S ≤4 mg/l, R >8 mg/l; Acinetobacter spp.: S ≤2 mg/l, R >8 mg/l; Staphylococcus spp. 3: Inferred from cefoxitin susceptibility; Enterococcus spp.: S ≤4 mg/l, R >8 mg/l; Streptococcus A, B, C, G: The beta-lactam susceptibility of beta-haemolytic streptococcus groups A, B, C and G is inferred from the penicillin susceptibility; Streptococcus pneumoniae 4: S ≤2 mg/l, R >2 mg/l; Other streptococci 4: S ≤2 mg/l, R >2 mg/l; Haemophilus influenzae 4: S ≤2 mg/l, R>2 mg/l; Moraxalla catarrhalis 4: S ≤2 mg/l, R >2 mg/l; Neisseria gonorrhoeae: There is insufficient evidence that Neisseria gonorrhoeae is a good target for therapy with imipenem; Gram-positive anaerobes: S ≤2 mg/l, R >8 mg/l; Gram-negative anaerobes: S ≤2 mg/l, R >8 mg/l; Non-species related breakpoints 5: S ≤2 mg/l, R >8 mg/l.
1 Proteus and Morganella species are considered poor targets for imipenem.
2 The breakpoints for Pseudomonas relate to high dose frequent therapy (1 g every 6 hours).
3 Susceptibility of staphylococci to carbapenems is inferred from the cefoxitin susceptibility.
4 Strains with MIC values above the susceptible breakpoint are very rare or not yet reported. The identification and antimicrobial susceptibility tests on any such isolate must be repeated and if the result is confirmed the isolate must be sent to a reference laboratory. Until there is evidence regarding clinical response for confirmed isolates with MIC above the current resistant breakpoint they should be reported resistant.
5 Non-species related breakpoint have been determined mainly on the basis of PK/PD data and are independent of MIC distributions of specific species. They are for use only for species not mentioned in the overview of species-related breakpoints or footnotes.
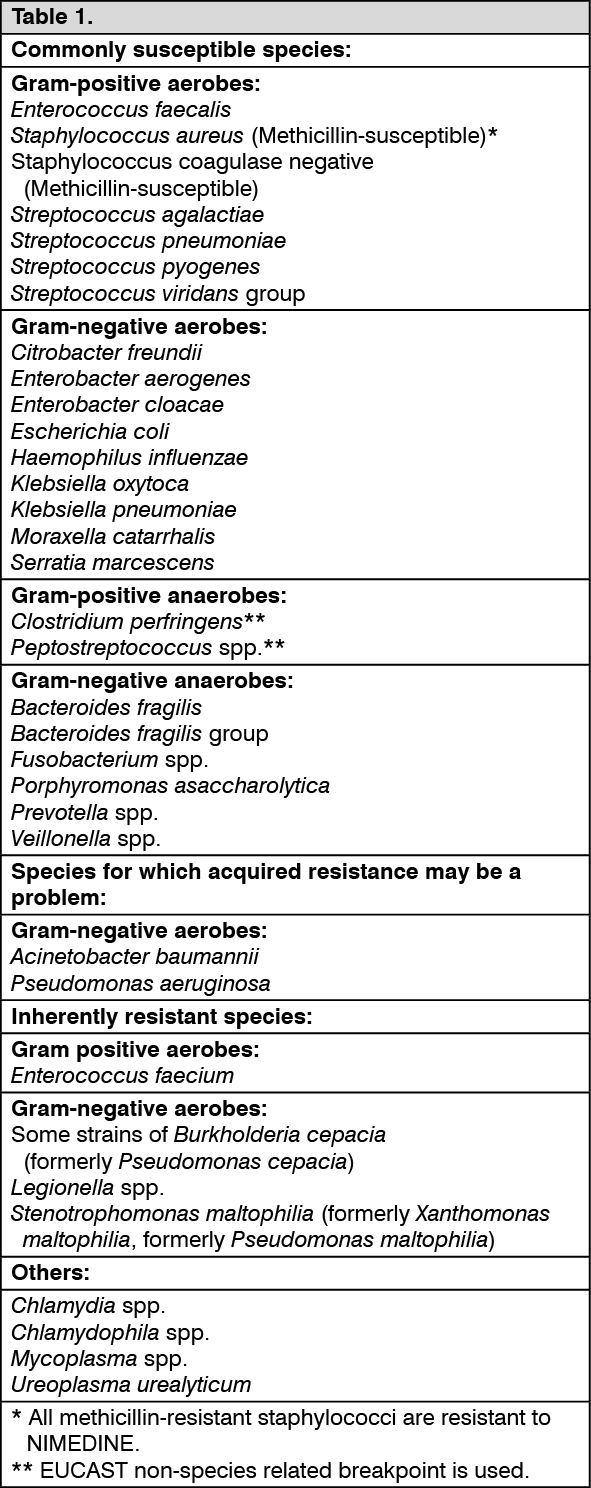
Susceptibility: The prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent in at least some types of infections is questionable. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Imipenem: Plasma concentrations: In normal volunteers, intravenous infusion of NIMEDINE over 20 minutes resulted in peak plasma levels of imipenem ranging from 12 to 20 μg/ml for the 250 mg/250 mg dose, from 21 to 58 μg/ml for the 500 mg/500 mg dose, and from 41 to 83 μg/ml for the 1000 mg/1000 mg dose. The mean peak plasma levels of imipenem following the 250 mg/250 mg, 500 mg/500 mg, and 1000 mg/1000 mg doses were 17, 39, and 66 μg/ml, respectively. At these doses, plasma levels of imipenem decline to below 1 μg/ml or less in four to six hours.
Distribution: The binding of imipenem to human serum proteins is approximately 20%.
Biotransformation and elimination: When administered alone, imipenem is metabolized in the kidneys by dehydropeptidase-I. Individual urinary recoveries ranged from 5 to 40%, with an average recovery of 15-20% in several studies.
Cilastatin is a specific inhibitor of dehydropeptidase-I enzyme and effectively inhibits metabolism of imipenem so that concomitant administration of imipenem and cilastatin allows therapeutic antibacterial levels of imipenem to be attained in both urine and plasma.
The plasma half-life of imipenem was one hour. Approximately 70% of the administered antibiotic was recovered intact in the urine within ten hours, and no further urinary excretion of imipenem was detectable. Urine concentrations of imipenem exceeded 10 μg/ml for up to eight hours after a 500 mg/500 mg dose of NIMEDINE. The remainder of the administered dose was recovered in the urine as antibacterially inactive metabolites, and faecal elimination of imipenem was essentially nil.
No accumulation of imipenem in plasma or urine has been observed with regimens of NIMEDINE, administered as frequently as every six hours, in patients with normal renal function.
Cilastatin: Plasma concentrations: Peak plasma levels of cilastatin, following a 20 minute intravenous infusion of NIMEDINE, ranged from 21 to 26 μg/ml for the 250 mg/250 mg dose, from 21 to 55 μg/ml for the 500 mg/500 mg dose and from 56 to 88 μg/ml for the 1000 mg/1000 mg dose. The mean peak plasma levels of cilastatin following the 250 mg/250 mg, 500 mg/500 mg, and 1000 mg/1000 mg doses were 22, 42, and 72 μg/ml respectively.
Distribution: The binding of cilastatin to human serum proteins is approximately 40%.
Biotransformation and elimination: The plasma half-life of cilastatin is approximately one hour. Approximately 70-80% of the dose of cilastatin was recovered unchanged in the urine as cilastatin within 10 hours of administration of NIMEDINE. No further cilastatin appeared in the urine thereafter. Approximately 10% was found as the N-acetyl metabolite, which has inhibitory activity against dehydropeptidase comparable to that of cilastatin. Activity of dehydropeptidase-I in the kidney returned to normal levels shortly after the elimination of cilastatin from the blood stream.
Renal insufficiency: Following a single 250 mg/250 mg intravenous dose of NIMEDINE, the area under the curve (AUCs) for imipenem increased 1.1-fold, 1.9-fold, and 2.7-fold in subjects with mild (Creatinine Clearance (CrCL) 50-80 ml/min/1.73 m2), moderate (CrCL 30-<50 ml/min/1.73 m2), and severe (CrCL <30 ml/min/1.73 m2) renal impairment, respectively, compared to subjects with normal renal function (CrCL >80 ml/min/1.73 m2), and AUCs for cilastatin increased 1.6-fold, 2.0-fold, and 6.2-fold in subjects with mild, moderate, and severe renal impairment, respectively, compared to subjects with normal renal function. Following a single 250 mg/250 mg intravenous dose of NIMEDINE given 24 hours after haemodialysis, AUCs for imipenem and cilastatin were 3.7-fold and 16.4-fold higher, respectively, as compared to subjects with normal renal function. Urinary recovery, renal clearance and plasma clearance of imipenem and cilastatin decrease with decreasing renal function following intravenous administration of NIMEDINE. Dose adjustment is necessary for patients with impaired renal function (see Dosage & Administration).
Hepatic insufficiency: The pharmacokinetics of imipenem in patients with hepatic insufficiency have not been established. Due to the limited extent of hepatic metabolism of imipenem, its pharmacokinetics are not expected to be affected by hepatic impairment. Therefore, no dose adjustment is recommended in patients with hepatic impairment (see Dosage & Administration).
Paediatric patients: The average clearance (CL) and volume of distribution (Vdss) for imipenem were approximately 45% higher in paediatric patients (3 months to 14 years) as compared to adults. The AUC for imipenem following administration of 15/15 mg/kg per body weight of NIMEDINE to paediatric patients was approximately 30% higher than the exposure in adults receiving a 500 mg/500 mg dose. At the higher dose, the exposure following administration of 25/25 mg/kg NIMEDINE to children was 9% higher as compared to the exposure in adults receiving a 1000 mg/1000 mg dose.
Elderly: In healthy elderly volunteers (65 to 75 years of age with normal renal function for their age), the pharmacokinetics of a single dose of NIMEDINE 500 mg/500 mg administered intravenously over 20 minutes were consistent with those expected in subjects with slight renal impairment for which no dose alteration is considered necessary. The mean plasma half-lives of imipenem and cilastatin were 91 ± 7.0 minutes and 69 ± 15 minutes, respectively. Multiple dosing has no effect on the pharmacokinetics of either imipenem or cilastatin, and no accumulation of NIMEDINE was observed (see Dosage & Administration).