As with other neuromuscular blocking agents, monitoring of neuromuscular function is recommended during the use of NIMBEX in order to individualise dosage requirements.
Use by I.V. bolus injection in adults: Tracheal Intubation: The recommended intubation dose of
NIMBEX for adults is 0.15 mg/kg administered rapidly over 5 to 10 seconds. This dose produces good to excellent conditions for tracheal intubation 120 seconds following injection.
Higher doses will shorten the time to onset of neuromuscular block. Table 2 summarises mean pharmacodynamic data when
NIMBEX injection was administered at doses of 0.1 to 0.4 mg/kg to healthy adult patients during opioid (thiopentone/fentanyl/midazolam) or propofol anaesthesia. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Enflurane or isoflurane anaesthesia may extend the clinically effective duration of an initial dose of NIMBEX by as much as 15%.
Maintenance: Neuromuscular block can be extended with maintenance doses of NIMBEX.
A dose of 0.03 mg/kg provides approximately 20 minutes of additional clinically effective neuromuscular block during opioid or propofol anaesthesia. Consecutive maintenance doses do not result in progressive prolongation of effect.
Spontaneous recovery: Once spontaneous recovery from neuromuscular block is underway, the rate is independent of the NIMBEX
dose administered. During opioid or propofol anaesthesia, the median times from 25 to 75% and from 5 to 95% recovery are approximately 13 and 30 minutes, respectively.
Reversal: Neuromuscular block following NIMBEX
administration is readily reversible with standard doses of anticholinesterase agents. The mean times from 25 to 75% recovery and to full clinical recovery (T
4:T
1 ratio more than or equal to 0.7) are approximately 2 and 5 minutes, respectively, following administration of the reversal agent at an average of 13% T
1 recovery.
Nimbex 2 mg: Use by I.V. bolus injection in children (aged 2 to 12 years of age): Tracheal intubation: The recommended initial intubation dose of NIMBEX in children aged 2 to 12 years is 0.1 mg/kg administered over 5 to 10 seconds. The following table summarises mean pharmacodynamic data obtained during opioid anaesthesia. A dose of 0.1 mg/kg has a faster onset time, a shorter clinical effective duration and a faster spontaneous recovery profile than those observed in adults under similar anaesthesia conditions. (See Table 3.)
Click on icon to see table/diagram/image
Halothane may be expected to extend the clinical effective duration of NIMBEX by up to 20%. No information is available on the use of NIMBEX in children during isoflurane or enflurane anaesthesia but these agents may also be expected to extend the clinically effective duration of a dose of NIMBEX by up to 20%.
Although tracheal intubation has not been specifically studied in this age group, onset is faster than in adults and therefore intubation should also be possible within two minutes of administration.
Maintenance: Neuromuscular block can be extended with maintenance doses of NIMBEX injection. A dose of 0.02 mg/kg provides approximately 9 minutes of additional clinically effective neuromuscular block during halothane anaesthesia. Consecutive maintenance doses do not result in progressive prolongation of effect.
Spontaneous Recovery: Once recovery from neuromuscular block is underway, the rate is independent of the NIMBEX dose administered. During opioid or halothane anesthesia, the median times from 25 to 75% and from 5 to 95% recovery are approximately 11 and 28 minutes, respectively.
Reversal: Neuromuscular block following NIMBEX administration is readily reversible with standard doses of anticholinesterase agents. The mean times from 25 to 75% recovery and to full clinical recovery (T4:T
1 ratio more than or equal to 0.7) are approximately 2 and 5 minutes, respectively, following administration of the reversal agent at an average of 13% T
1 recovery.
Use by I.V. infusion in adults and children (aged 2 to 12 years): Maintenance of neuromuscular block may be achieved by infusion of NIMBEX. An initial infusion rate of 3 micrograms/kg/min (0.18 mg/kg/h) is recommended to restore 89 to 99% T
1 suppression following evidence of spontaneous recovery. After an initial period of stabilisation of neuromuscular block, a rate of 1 to 2 micrograms/kg/min (0.06 to 0.12 mg/kg/h) should be adequate to maintain block in this range in most patients.
Reduction of the infusion rate by up to 40% may be required when NIMBEX is administered during isoflurane or enflurane anaesthesia (see Interactions).
The infusion rate will depend upon the concentration of NIMBEX in the infusion solution, the desired degree of neuromuscular block, and the patient's weight. Table 4 provides guidelines for delivery of undiluted NIMBEX. (See Table 4.)
Click on icon to see table/diagram/image
Steady rate continuous infusion of NIMBEX is not associated with a progressive increase or decrease in neuromuscular blocking effect.
Following discontinuation of infusion of NIMBEX, spontaneous recovery from neuromuscular block proceeds at a rate comparable to that following administration of a single bolus.
Nimbex Forte: Although not specifically in paediatric patients under 2 years of age,
extrapolation of pharmacodynamic data for bolus doses suggests that NIMBEX
infusion rates should be similar.
Nimbex Forte: Use by I.V. bolus injection children (1 month to 12 years of age): Tracheal intubation: As in adults, the recommended initial intubation dose of NIMBEX is 0.15 mg/kg administered rapidly over 5 to 10 seconds.
This dose produces good to excellent conditions for tracheal intubation 120 seconds following injection of NIMBEX. Pharmacodynamic data for this dose are presented in the Table 5 and Table 6. If a shorter clinical duration is required, pharmacodynamic data suggest that a dose of 0.1 mg/kg may produce similar intubation conditions at 120 to 150 seconds.
In paediatric patients aged 1 month to 12 years, NIMBEX has a shorter clinically effective duration and a faster spontaneous recovery profile than those observed in adults under similar anaesthetic conditions. Small differences in the pharmacodynamic profile were observed between the age ranges 1 to 11 months and 1 to 12 years which are summarised in the tables. (See Table 5 and Table 6).
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Halothane may be expected to extend the clinically effective duration of NIMBEX by up to 20%. No information is available on the use of NIMBEX in children during isoflurane or enflurane anaesthesia but these agents may also be expected to extend the clinically effective duration of a dose of NIMBEX
by up to 20%.
Maintenance: Neuromuscular block can be extended with maintenance doses of NIMBEX injection. A dose of 0.02 mg/kg provides approximately 9 min of additional clinically effective neuromuscular block during halothane anaesthesia. Consecutive maintenance doses do not result in progressive prolongation of effect.
Spontaneous recovery: Once recovery from neuromuscular block is underway, the rate is independent of the NIMBEX dose administered. During opioid or halothane anaesthesia, the median times from 25 to 75% and from 5 to 95% recovery are approximately 11 and 28 min, respectively.
Reversal: Neuromuscular block following NIMBEX administration is readily reversible with standard doses of anticholinesterase agents. The mean times from 25 to 75% recovery and to full clinical recovery (T
4:T
1 ratio more than or equal to 0.7) are approximately 2 and 5 min, respectively, following administration of the reversal agent at an average of 13% T
1 recovery.
Nimbex 2 mg: Neonates aged less than 2 years: No dosage recommendation for paediatric patients under 2 years of age can be made until further information becomes available.
Nimbex Forte: Neonates aged less than 1 month: No dosage recommendation for neonates can be made as administration of NIMBEX has not been studied in this patient population.
Elderly: No dosing alterations are required in elderly patients. In these patients NIMBEX has a similar pharmacodynamic profile to that observed in young adult patients but, as with other neuromuscular blocking agents, it may have a slightly slower onset.
Patients with renal impairment: No dosing alterations are required in patients with renal failure. In these patients NIMBEX has a similar pharmacodynamic profile to that observed in patients with normal renal function but it may have a slightly slower onset.
Patients with hepatic impairment: No dosing alterations are required in patients with end-stage liver disease. In these patients NIMBEX has a similar pharmacodynamic profile to that observed in patients with normal hepatic function but it may have a slightly faster onset.
Patients with cardiovascular disease: NIMBEX has been used effectively to provide neuromuscular block in patients undergoing cardiac surgery. When administered by rapid bolus injection (over 5 to 10 seconds) to patients with serious cardiovascular disease NIMBEX has not been associated with clinically significant cardiovascular effects at any dose studied (up to and including 0.4 mg/kg (8 x ED
95).
ICU Patients: NIMBEX may be administered by bolus dose and/or infusion to adult patients in the ICU.
An initial infusion rate of NIMBEX of 3 micrograms/kg/min (0.18 mg/kg/h) is recommended for adult ICU patients. There may be wide inter-patient variation in dosage requirements and these may increase or decrease with time. In clinical studies the average infusion rate was 3 micrograms/kg/min [range 0.5 to 10.2 micrograms/kg/min (0.03 to 0.6 mg/kg/h)]. Table 7 provides guidelines for delivery of undiluted NIMBEX.
The median time to full spontaneous recovery following long-term (up to 6 days) infusion of NIMBEX in ICU patients was approximately 50 minutes. (See Table 7.)
Click on icon to see table/diagram/image
Nimbex 2 mg: The recovery profile after infusions of NIMBEX to ICU patients is independent of duration of infusion.
Nimbex 2 mg and Nimbex Forte: Patients undergoing hypothermic cardiac surgery: There have been no studies of NIMBEX in patients undergoing surgery with induced hypothermia (25°C to 28°C). As with other neuromuscular blocking agents, the rate of infusion required to maintain adequate surgical relaxation under these conditions may be expected to be significantly reduced.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image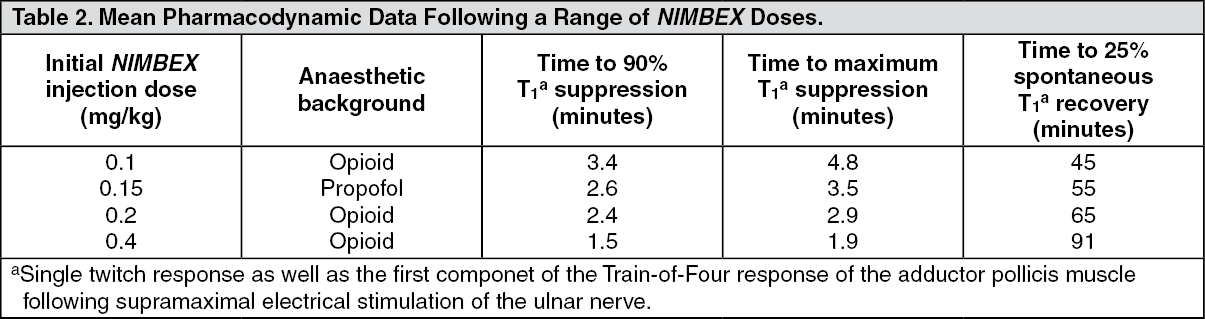 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image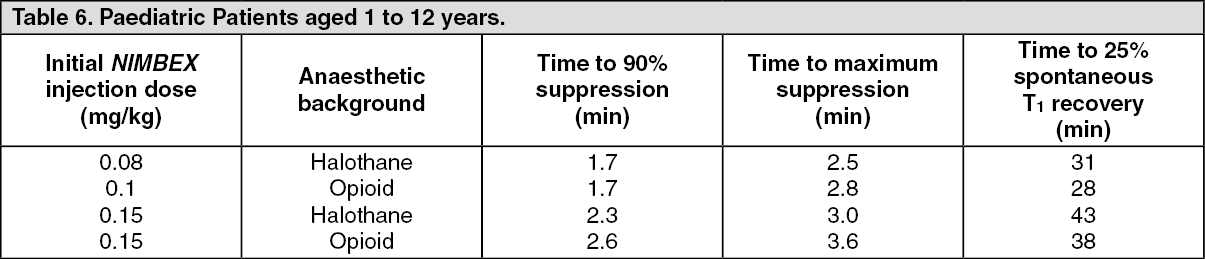 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
