Each Film Coated Tablet contains: Tenofovir Alafenamide fumarate equivalent to Tenofovir Alafenamide 25 mg.
Excipients with known effects: Each film-coated tablet contains 67.957 mg of lactose monohydrate.
Excipients/Inactive Ingredients: Core tablet: Lactose Monohydrate, Microcrystalline Cellulose, Croscarmellose Sodium, Magnesium Stearate.
Film coat: Polyvinyl Alcohol, Polyethylene Glycol, Titanium Dioxide & Talc.
Pharmacotherapeutic group: Antiviral for systemic use, nucleoside and nucleotide reverse transcriptase inhibitors. ATC code: J05AF13.
Pharmacology: Mechanism of action: Tenofovir alafenamide is a phosphonamidate prodrug of tenofovir (2'-deoxyadenosine monophosphate analogue). Tenofovir alafenamide enters primary hepatocytes by passive diffusion and by the hepatic uptake transporters OATP1B1 and OATP1B3. Tenofovir alafenamide is primarily hydrolyzed to form tenofovir by carboxylesterase 1 in primary hepatocytes. Intracellular tenofovir is subsequently phosphorylated to the pharmacologically active metabolite tenofovir diphosphate. Tenofovir diphosphate inhibits HBV replication through incorporation into viral DNA by the HBV reverse transcriptase, which results in DNA chain termination.
Tenofovir has activity that is specific to hepatitis B virus and human immunodeficiency virus (HIV-1 and HIV-2). Tenofovir diphosphate is a weak inhibitor of mammalian DNA polymerases that include mitochondrial DNA polymerase γ and there is no evidence of mitochondrial toxicity in vitro based on several assays including mitochondrial DNA analyses.
Antiviral activity: The antiviral activity of tenofovir alafenamide was assessed in HepG2 cells against a panel of HBV clinical isolates representing genotypes A-H. The EC50 (50% effective concentration) values for tenofovir alafenamide ranged from 34.7 to 134.4 nM, with an overall mean EC50 of 86.6 nM. The CC50 (50% cytotoxicity concentration) in HepG2 cells was > 44400 nM.
Resistance: No amino acid substitutions associated with resistance to Tenofovir alafenamide were identified in these isolates (genotypic and phenotypic analyses).
Cross-resistance: The antiviral activity of tenofovir alafenamide was evaluated against a panel of isolates containing nucleos(t)ide reverse transcriptase inhibitor mutations in HepG2 cells. HBV isolates expressing the rtV173L, rtL180M, and rtM204V/I substitutions associated with resistance to lamivudine remained susceptible to tenofovir alafenamide (< 2-fold change in EC50). HBV isolates expressing the rtL180M, rtM204V plus rtT184G, rtS202G, or rtM250V substitutions associated with resistance to entecavir remained susceptible to tenofovir alafenamide. HBV isolates expressing the rtA181T, rtA181V, or rtN236T single substitutions associated with resistance to adefovir remained susceptible to tenofovir alafenamide; however, the HBV isolate expressing rtA181V plus rtN236T exhibited reduced susceptibility to tenofovir alafenamide (3.7-fold change in EC50). The clinical relevance of these substitutions is not known.
Pharmacokinetics: Absorption: Following oral administration of Tenofovir alafenamide under fasted conditions in adult patients with chronic hepatitis B, peak plasma concentrations of tenofovir alafenamide were observed approximately 0.48 hours post-dose. In patients with CHB, mean steady state AUC0-24 for tenofovir alafenamide and tenofovir were 0.22 μg·hr/mL and 0.32 μg·hr/mL, respectively. Steady state Cmax for tenofovir alafenamide and tenofovir were 0.18 and 0.02 μg/mL, respectively. Relative to fasting conditions, the administration of a single dose of Tenofovir alafenamide with a high fat meal resulted in a 65% increase in tenofovir alafenamide exposure.
Distribution: The binding of tenofovir alafenamide to human plasma proteins was approximately 80%. The binding of tenofovir to human plasma proteins is less than 0.7% and is independent of concentration over the range of 0.01-25 μg/mL.
Biotransformation: Metabolism is a major elimination pathway for tenofovir alafenamide in humans, accounting for > 80% of an oral dose. It is shown that tenofovir alafenamide is metabolized to tenofovir (major metabolite) by carboxylesterase-1 in hepatocytes; and by cathepsin A in peripheral blood mononuclear cells (PBMCs) and macrophages. Tenofovir alafenamide is hydrolysed within cells to form tenofovir (major metabolite), which is phosphorylated to the active metabolite, tenofovir diphosphate. Tenofovir alafenamide is not metabolized by CYP1A2, CYP2C8, CYP2C9, CYP2C19, or CYP2D6. Tenofovir alafenamide is minimally metabolized by CYP3A4.
Elimination: Renal excretion of intact tenofovir alafenamide is a minor pathway with < 1% of the dose eliminated in urine. Tenofovir alafenamide is mainly eliminated following metabolism to tenofovir. Tenofovir alafenamide and tenofovir have a median plasma half-life of 0.51 and 32.37 hours, respectively. Tenofovir is renally eliminated from the body by the kidneys by both glomerular filtration and active tubular secretion.
Linearity/non-linearity: Tenofovir alafenamide exposures are dose proportional over the dose range of 8 to 125 mg.
Pharmacokinetics in special populations: Age, gender and ethnicity: No clinically relevant differences in pharmacokinetics according to age or ethnicity have been identified. Differences in pharmacokinetics according to gender were not considered to be clinically relevant.
Hepatic impairment: In patients with severe hepatic impairment, total plasma concentrations of tenofovir alafenamide and tenofovir are lower than those with normal hepatic function. When corrected for protein binding, unbound (free) plasma concentrations of tenofovir alafenamide in severe hepatic impairment and normal hepatic function are similar.
Renal impairment: No clinically relevant differences in tenofovir alafenamide or tenofovir pharmacokinetics were observed between healthy subjects and patients with severe renal impairment (estimated CrCl > 15 but < 30 mL/min).
Paediatric population: No clinically relevant differences in tenofovir alafenamide or tenofovir pharmacokinetics were observed between adolescent and adult HIV-1-infected subjects.
Tenofovir Alafenamide is indicated for the treatment of chronic hepatitis B in adults and adolescents (aged 12 years and older with body weight at least 35 kg) (see Pharmacology: Pharmacodynamics under Actions).
Therapy should be initiated by a physician experienced in the management of chronic hepatitis B.
Posology: Adults and adolescents (aged 12 years and older with body weight at least 35 kg): one tablet once daily.
Treatment discontinuation: Treatment discontinuation may be considered as follows (See Precautions): In HBeAg-positive patients without cirrhosis, treatment should be administered for at least 6-12 months after HBe seroconversion (HBeAg loss and HBV DNA loss with anti-HBe detection) is confirmed or until HBs seroconversion or until there is loss of efficacy. (See Precautions). Regular reassessment is recommended after treatment discontinuation to detect virological relapse.
In HBeAg-negative patients without cirrhosis, treatment should be administered at least until HBs seroconversion or until there is evidence of loss of efficacy. With prolonged treatment for more than 2 years, regular reassessment is recommended to confirm that continuing the selected therapy remains appropriate for the patient.
Missed dose: If a dose is missed and less than 18 hours have passed from the time it is usually taken, the patient should take Tenofovir alafenamide as soon as possible and then resume their normal dosing schedule. If more than 18 hours have passed from the time it is usually taken, the patient should not take the missed dose and should simply resume the normal dosing schedule. If the patient vomits within 1 hour of taking Tenofovir alafenamide, the patient should take another tablet. If the patient vomits more than 1 hour after taking Tenofovir alafenamide, the patient does not need to take another tablet.
Special populations: Elderly: No dose adjustment of Tenofovir alafenamide is required in patients aged 65 years and older (see Pharmacology: Pharmacokinetics under Actions).
Renal impairment: No dose adjustment of Tenofovir alafenamide is required in adults or adolescents (aged at least 12 years and of at least 35 kg body weight) with estimated creatinine clearance (CrCl) ≥ 15 mL/min or in patients with CrCl < 15 mL/min who are receiving haemodialysis.
On days of haemodialysis, Tenofovir alafenamide should be administered after completion of haemodialysis treatment (see Pharmacology: Pharmacokinetics under Actions).
No dosing recommendations can be given for patients with CrCl < 15 mL/min who are not receiving haemodialysis (See Precautions).
Hepatic impairment: No dose adjustment of Tenofovir alafenamide is required in patients with hepatic impairment (See Precautions & Pharmacology: Pharmacokinetics under Actions).
Paediatric population: The safety and efficacy of Tenofovir alafenamide in children younger than 12 years of age, or weighing < 35 kg, have not yet been established. No data are available.
MODE OF ADMINISTRATION: Oral. Tenofovir alafenamide film-coated tablets should be taken with food.
If overdose occurs the patient must be monitored for evidence of toxicity. Treatment of overdose with Tenofovir alafenamide consists of general supportive measures including monitoring of vital signs as well as observation of the clinical status of the patient. Tenofovir is efficiently removed by haemodialysis with an extraction coefficient of approximately 54%. It is not known whether tenofovir can be removed by peritoneal dialysis.
Hypersensitivity to the active substance or to any of the excipients.
HBV transmission: Patients must be advised that Tenofovir alafenamide does not prevent the risk of transmission of HBV to others through sexual contact or contamination with blood. Appropriate precautions must continue to be used.
Patients with decompensated liver disease: There are no data on the safety and efficacy of Tenofovir alafenamide in HBV-infected patients with decompensated liver disease and who have a Child Pugh Turcotte (CPT) score > 9 (i.e. class C). These patients may be at higher risk of experiencing serious hepatic or renal adverse reactions. Therefore, hepatobiliary and renal parameters should be closely monitored in this patient population.
Exacerbation of hepatitis: Flares on treatment: Spontaneous exacerbations in chronic hepatitis B are relatively common and are characterised by transient increases in serum alanine aminotransferase (ALT). After initiating antiviral therapy, serum ALT may increase in some patients. In patients with compensated liver disease, these increases in serum ALT are generally not accompanied by an increase in serum bilirubin concentrations or hepatic decompensation. Patients with cirrhosis may be at a higher risk for hepatic decompensation following hepatitis exacerbation, and therefore should be monitored closely during therapy.
Flares after treatment discontinuation: Acute exacerbation of hepatitis has been reported in patients who have discontinued treatment for hepatitis B, usually in association with rising HBV DNA levels in plasma. The majority of cases are self-limited but severe exacerbations, including fatal outcomes, may occur after discontinuation of treatment for hepatitis B. Hepatic function should be monitored at repeated intervals with both clinical and laboratory follow-up for at least 6 months after discontinuation of treatment for hepatitis B. If appropriate, resumption of hepatitis B therapy may be warranted. In patients with advanced liver disease or cirrhosis, treatment discontinuation is not recommended since post-treatment exacerbation of hepatitis may lead to hepatic decompensation. Liver flares are especially serious, and sometimes fatal in patients with decompensated liver disease.
Renal impairment: Patients with creatinine clearance < 30 mL/min: The use of Tenofovir alafenamide once daily in patients with CrCl ≥15 mL/min but < 30 mL/min and in patients with CrCl < 15 mL/min who are receiving haemodialysis is based on very limited pharmacokinetic data and on modelling and simulation. There are no safety data on the use of Tenofovir alafenamide to treat HBV-infected patients with CrCl < 30 mL/min.
The use of Tenofovir Alafenamide is not recommended in patients with CrCl < 15 mL/min who are not receiving haemodialysis.
Nephrotoxicity: A potential risk of nephrotoxicity resulting from chronic exposure to low levels of tenofovir due to dosing with tenofovir alafenamide cannot be excluded.
Patients co-infected with HBV and hepatitis C or D virus: There are no data on the safety and efficacy of Tenofovir alafenamide in patients co-infected with hepatitis C or D virus. Co-administration guidance for the treatment of hepatitis C should be followed.
Hepatitis B and HIV co-infection: HIV antibody testing should be offered to all HBV-infected patients whose HIV-1 infection status is unknown before initiating therapy with Tenofovir alafenamide. In patients who are co-infected with HBV and HIV, Tenofovir alafenamide should be co-administered with other antiretroviral agents to ensure that the patient receives an appropriate regimen for treatment of HIV.
Co-administration with other medicinal products: Tenofovir alafenamide should not be co-administered with products containing tenofovir alafenamide, tenofovir disoproxil fumarate or adefovir dipivoxil.
Co-administration of Tenofovir alafenamide with certain anticonvulsants (e.g. carbamazepine, oxcarbazepine, phenobarbital and phenytoin), antimycobacterials (e.g. rifampicin, rifabutin and rifapentine) or St. John's wort, all of which are inducers of P-glycoprotein (P-gp) and may decrease tenofovir alafenamide plasma concentrations, is not recommended.
Co-administration of Tenofovir alafenamide with strong inhibitors of P-gp (e.g. itraconazole and ketoconazole) may increase tenofovir alafenamide plasma concentrations. Co-administration is not recommended.
Lactose intolerance: MyTAFF contains lactose monohydrate. Consequently, patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency, or glucose-galactose malabsorption should not take this medicinal product.
Effects on Ability to Drive and Use Machine: Tenofovir alafenamide has no or negligible influence on the ability to drive and use machines. Patients should be informed that dizziness has been reported during treatment with Tenofovir alafenamide.
Pregnancy: There are no or limited amount of data (less than 300 pregnancy outcomes) from the use of tenofovir alafenamide in pregnant women. However, a large amount of data on pregnant women (more than 1000 exposed outcomes) indicates no malformative nor feto/neonatal toxicity associated with the use of tenofovir disoproxil fumarate. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity. The use of Tenofovir alafenamide may be considered during pregnancy, if necessary.
Breast-feeding: It is not known whether tenofovir alafenamide is secreted in human milk. However, in animal studies it has been shown that tenofovir is secreted into milk. There is insufficient information on the effects of tenofovir in newborns/infants. A risk to the breastfed child cannot be excluded; therefore, Tenofovir alafenamide should not be used during breast-feeding.
Fertility: No human data on the effect of Tenofovir alafenamide on fertility are available. Animal studies do not indicate harmful effects of tenofovir alafenamide on fertility.
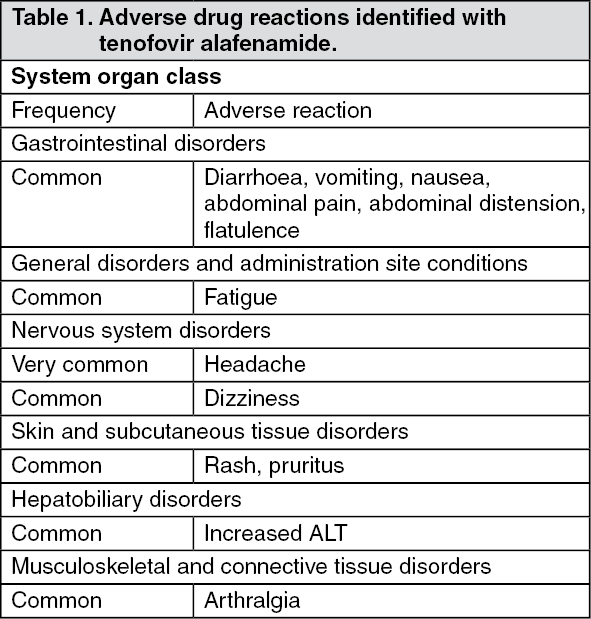
Summary of the safety profile: The most frequently reported adverse reactions were headache, nausea, and fatigue.
Tabulated summary of adverse reactions: The following adverse drug reactions have been identified with tenofovir alafenamide in patients with chronic hepatitis B (Table 1). The adverse reactions are listed as follows by body system organ class and frequency. Frequencies are defined as follows: very common, common, uncommon, rare or very rare. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Interaction studies have only been performed in adults. Tenofovir alafenamide should not be co-administered with medicinal products containing tenofovir disoproxil fumarate, tenofovir alafenamide or adefovir dipivoxil.
Medicinal products that may affect tenofovir alafenamide: Tenofovir alafenamide is transported by P-gp and breast cancer resistance protein (BCRP). Medicinal products that are P-gp inducers (e.g., rifampicin, rifabutin, carbamazepine, phenobarbital or St. John's wort) are expected to decrease plasma concentrations of tenofovir alafenamide, which may lead to loss of therapeutic effect of Tenofovir alafenamide. Co-administration of such medicinal products with Tenofovir alafenamide is not recommended. Co-administration of Tenofovir alafenamide with medicinal products that inhibit P-gp and/or BCRP may increase plasma concentration of tenofovir alafenamide. Co-administration of strong inhibitors of P-gp with Tenofovir alafenamide is not recommended. Tenofovir alafenamide is a substrate of OATP1B1 and OATP1B3. The distribution of tenofovir alafenamide in the body may be affected by the activity of OATP1B1 and/or OATP1B3.
Effect of tenofovir alafenamide on other medicinal products: Tenofovir alafenamide is not an inhibitor of CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, or CYP2D6. It is not an inhibitor of CYP3A. Tenofovir alafenamide is not an inhibitor of human uridine diphosphate glucuronosyltransferase (UGT) 1A1. It is not known whether tenofovir alafenamide is an inhibitor of other UGT enzymes.
Drug interaction information for Tenofovir alafenamide with potential concomitant medicinal products is summarised in Table 2 as follows (increase is indicated as "↑", decrease as "↓", no change as "↔"; twice daily as "b.i.d.", single dose as "s.d.", once daily as "q.d."; and intravenously as "IV"). (See Tables 2A, 2B and 2C.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Special precautions for disposal: No special requirements. Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Incompatibilities: Not applicable.
Store in a dry place below 30°C. Store in the original container.
Shelf-Life: 24 months.
J05AF13 - tenofovir alafenamide ; Belongs to the class of nucleoside and nucleotide reverse transcriptase inhibitors. Used in the systemic treatment of viral infections.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image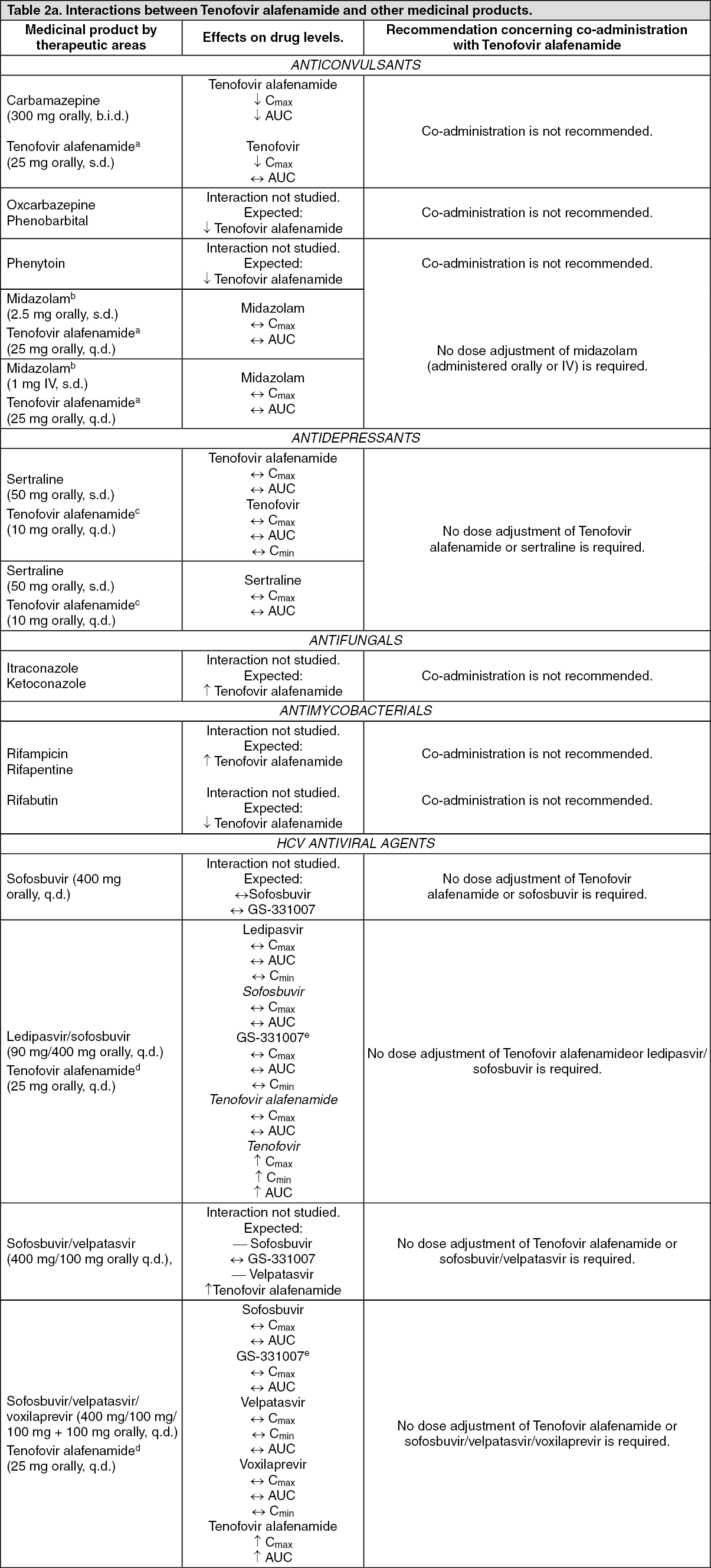 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image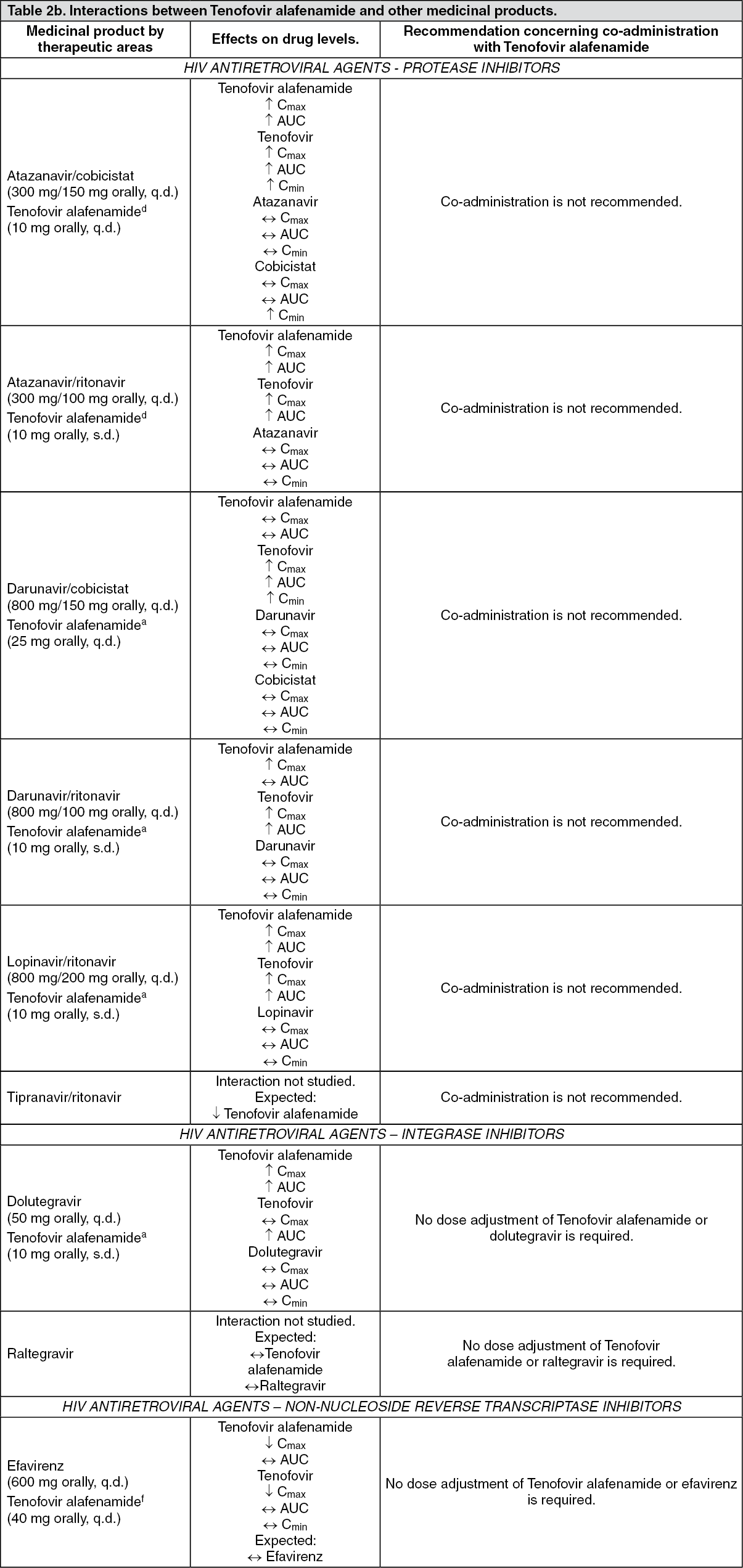 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
