


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Dolutegravir inhibits HIV integrase by binding to the integrase active site and blocking the strand transfer step of retroviral Deoxyribonucleic acid (DNA) integration which is essential for the HIV replication cycle.
Pharmacodynamic effects: Antiviral activity in cell culture: The IC50 for dolutegravir in various labstrains using PBMC was 0.5 nM, and when using MT-4 cells it ranged from 0.7-2 nM. Similar IC50s were seen for clinical isolates without any major difference between subtypes; in a panel of 24 HIV-1 isolates of clades A, B, C, D, E, F and G and group O the mean IC50 value was 0.2 nM (range 0.02-2.14). The mean IC50 for 3 HIV-2 isolates was 0.18 nM (range 0.09-0.61).
Antiviral activity in combination with other antiviral agents: No antagonistic effects were seen with dolutegravir and other antiretrovirals tested: stavudine, abacavir, efavirenz, nevirapine, lopinavir, amprenavir, enfuvirtide, maraviroc and raltegravir. In addition, no antagonistic effects were seen for dolutegravir and adefovir, and ribavirin had no apparent effect on dolutegravir activity.
Effect of human serum: In 100% human serum, the mean protein fold shift was 75 fold, resulting in protein adjusted IC90 of 0.064 µg/mL.
Resistance: Mutations selected appeared slowly using the lab-strain HIV-1 IIIB during passage, with substitutions at positions S153Y and F, resulting in a maximal fold change in susceptibility of 4.
Mutation R263K was reported from ART experienced, INI naive individual patients with subtypes B and C, but without effects on dolutegravir susceptibility. G118R lowers the susceptibility to dolutegravir in site directed mutants (FC 10), but was not detected in patients receiving dolutegravir.
Primary mutations for raltegravir/elvitegravir (Q148H/R/K, N155H, Y143R/H/C, E92Q and T66I) do not affect the susceptibility of dolutegravir as single mutations. When mutations listed as secondary integrase inhibitor associated mutations (for raltegravir/elvitegravir) are added to these primary mutations with site directed mutants, dolutegravir susceptibility is still unchanged (FC <2 vs wild type virus), except in the case of Q148-mutations, where a FC of 5-10 or higher is seen with combinations of certain secondary mutations. With strain NL432, starting with site directed mutants harbouring N155H or E92Q, no further selection of resistance was seen (FC unchanged around 1). In contrast, starting with mutants harbouring mutation Q148H (FC 1), a variety of secondary mutations were seen with a consequent increase of FC to values >10.
A clinically relevant phenotypic cut-off value (FC vs wild type virus) has not been determined; genotypic resistance was a better predictor for outcome.
Dolutegravir has a less than or equal to 10 FC against 94% of isolates from raltegravir experienced patients.
Resistance: In previously untreated patients receiving dolutegravir + 2 NRTIs, no development of resistance to the integrase class, or to the NRTI class was seen. In previously untreated patients receiving dolutegravir + lamivudine through week 96, no development of resistance to the integrase class, or to the NRTI class was seen.
In patients with prior failed therapies, but naïve to the integrase class, integrase inhibitor substitutions were observed in patients treated with dolutegravir, which was given in combination with an selected background regimen (BR).
In the presence of integrase class-resistance, treatment emergent integrase resistance typically appeared in patients with a history of the Q148-mutation (baseline or historic). Treatment-emergent mutations or mixtures of mutations observed were L74I, N155H.
In paediatric patients with prior failed therapies, but naïve to the integrase class, the integrase inhibitor substitution G118R was observed in patients treated with dolutegravir, given in combination with an selected background regimen. Dolutegravir FC (fold change as compared to wildtype virus) ranged from 6 to 25-fold.
Effects on electrocardiogram: No relevant effects were seen on the QTc interval, with doses exceeding the clinical dose by approximately three fold.
Pharmacokinetics: Dolutegravir pharmacokinetics are similar between healthy and HIV-infected patients. The PK variability of dolutegravir is low to moderate. Between-patient CVb% for AUC and Cmax ranged from ~20 to 40% and Cτ from 30 to 65%. The between-patient PK variability of dolutegravir was higher in HIV-infected patients than healthy patients. Within-patient variability (CVw%) is lower than between-patient variability.
Film-coated tablets and dispersible tablets do not have the same bioavailability. The relative bioavailability of dispersible tablets is approximately 1.6-fold higher as compared to film-coated tablets. Thus, a 50 mg dolutegravir dose administered as film-coated tablet(s) will have similar exposure to a 30 mg dolutegravir dose administered as six 5 mg dispersible tablets. Similarly, a 40 mg dolutegravir dose administered as four 10 mg film-coated tablets will provide comparable exposure to a 25 mg dolutegravir dose administered as five 5 mg dispersible tablets.
Absorption: Dolutegravir is rapidly absorbed following oral administration, with median Tmax at 2 to 3 hours post dose for tablet formulation.
Food increased the extent and slowed the rate of absorption of dolutegravir. Bioavailability of dolutegravir depends on meal content: low, moderate, and high fat meals increased dolutegravir AUC(0-∞) by 33%, 41%, and 66%, increased Cmax by 46%, 52%, and 67%, prolonged Tmax to 3, 4, and 5 hours from 2 hours under fasted conditions, respectively for the film-coated tablet. These increases may be clinically relevant in the presence of certain integrase class resistance. Therefore, MYLTEGA is recommended to be taken with food by patients infected with HIV with integrase class resistance (see Dosage & Administration).
The absolute bioavailability of dolutegravir has not been established.
Distribution: Dolutegravir is highly bound (>99%) to human plasma proteins based on data. The apparent volume of distribution is 17 L to 20 L in HIV-infected patients. Binding of dolutegravir to plasma proteins is independent of dolutegravir concentration. Total blood and plasma drug-related radioactivity concentration ratios averaged between 0.441 to 0.535, indicating minimal association of radioactivity with blood cellular components. The unbound fraction of dolutegravir in plasma is increased at low levels of serum albumin (<35 g/L) as seen in patients with moderate hepatic impairment.
Dolutegravir is present in cerebrospinal fluid (CSF). In treatment-naïve patients on a stable dolutegravir plus abacavir/lamivudine regimen, dolutegravir concentration in CSF averaged 18 ng/mL (comparable to unbound plasma concentration, and above the IC50).
Dolutegravir is present in the female and male genital tract. AUC in cervicovaginal fluid, cervical tissue and vaginal tissue were 6-10% of those in corresponding plasma at steady state. AUC in semen was 7% and 17% in rectal tissue of those in corresponding plasma at steady state.
Biotransformation: Dolutegravir is primarily metabolized through glucuronidation via UGT1A1 with a minor CYP3A component. Dolutegravir is the predominant circulating compound in plasma; renal elimination of unchanged active substance is low (< 1% of the dose). Fifty-three percent of total oral dose is excreted unchanged in the faeces. It is unknown if all or part of this is due to unabsorbed active substance or biliary excretion of the glucuronidate conjugate, which can be further degraded to form the parent compound in the gut lumen. Thirty-two percent of the total oral dose is excreted in the urine, represented by ether glucuronide of dolutegravir (18.9% of total dose), N-dealkylation metabolite (3.6% of total dose), and a metabolite formed by oxidation at the benzylic carbon (3.0% of total dose).
Drug interactions: Dolutegravir demonstrated no direct, or weak inhibition (IC50>50 μM) of the enzymes cytochrome P450 (CYP)1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6 CYP3A, uridine diphosphate glucuronosyl transferase (UGT)1A1 or UGT2B7, or the transporters Pgp, BCRP, BSEP, OATP1B1, OATP1B3, OCT1, MATE2-K, MRP2 or MRP4. Dolutegravir did not induce CYP1A2, CYP2B6 or CYP3A4. Based on this data, dolutegravir is not expected to affect the pharmacokinetics of medicinal products that are substrates of major enzymes or transporters (see Interactions).
Dolutegravir was not a substrate of human OATP 1B1, OATP 1B3 or OCT 1.
Elimination: Dolutegravir has a terminal half-life of ~14 hours. The apparent oral clearance (CL/F) is approximately 1L/hr in HIV-infected patients based on a population pharmacokinetic analysis.
Linearity/non-linearity: The linearity of dolutegravir pharmacokinetics is dependent on dose and formulation. Following oral administration of film-coated tablet formulations, in general, dolutegravir exhibited nonlinear pharmacokinetics with less than dose-proportional increases in plasma exposure from 2 to 100 mg; however increase in dolutegravir exposure appears dose proportional from 25 mg to 50 mg for the film-coated tablet formulation. With 50 mg film-coated tablet twice daily, the exposure over 24 hours was approximately doubled compared to 50 mg film-coated tablet once daily.
Pharmacokinetic/pharmacodynamic relationship(s): In HIV-1-infected patients treated with dolutegravir monotherapy (ING111521), it demonstrated rapid and dose-dependent antiviral activity, with mean decline in HIV-1 RNA of 2.5 log10 at day 11 for 50 mg dose. This antiviral response was maintained for 3 to 4 days after the last dose in the 50 mg film-coated tablet group.
PK/PD modelling in integrase resistant patients suggest that increasing the dose from 50 mg film-coated tablet twice daily to 100 mg film-coated tablet twice daily may increase the effectiveness of dolutegravir in patients with integrase resistance and limited treatment options due to advanced multi class resistance. The proportion of responders (HIV-1 RNA <50 c/mL) at week 24 was predicted to increase around 4-18% in the patients with Q148 + ≥2 secondary mutations from G140A/C/S, E138A/K/T, L74I. This high dose may be considered in the presence of the Q148 + ≥2 secondary mutations from G140A/C/S, E138A/K/T, L74I in patients with overall limited treatment options due to advanced multi class resistance. There is no clinical data on the safety or efficacy of the 100 mg film-coated tablet twice daily dose. Co-treatment with atazanavir increases the exposure of dolutegravir markedly, and should not be used in combination with this high dose, since safety with the resulting dolutegravir exposure has not been established.
Special patient populations: Children: Steady state simulated plasma exposure at once daily weight band doses n HIV-1 infected infants, children and adolescents aged ≥ 4 weeks to < 18 years is summarized in Table 1. (See Table 1.)
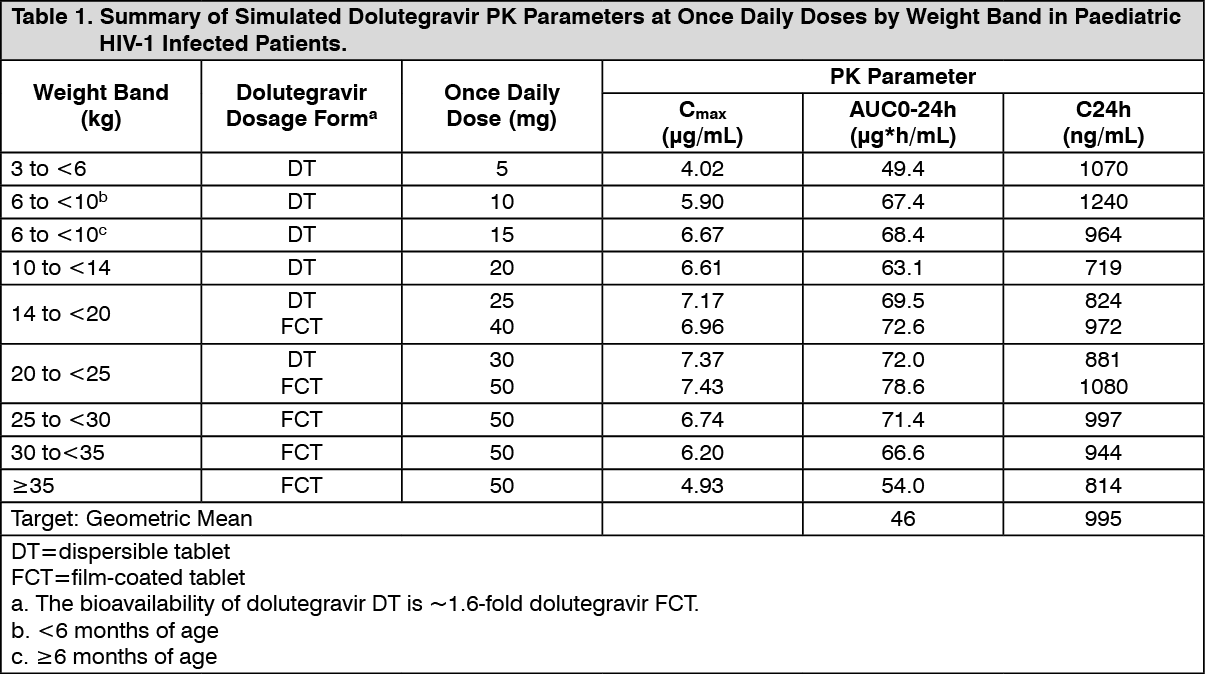 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSteady state simulated plasma exposure at alternative twice daily weight band doses are summarized in Table 2. (See Table 2.)
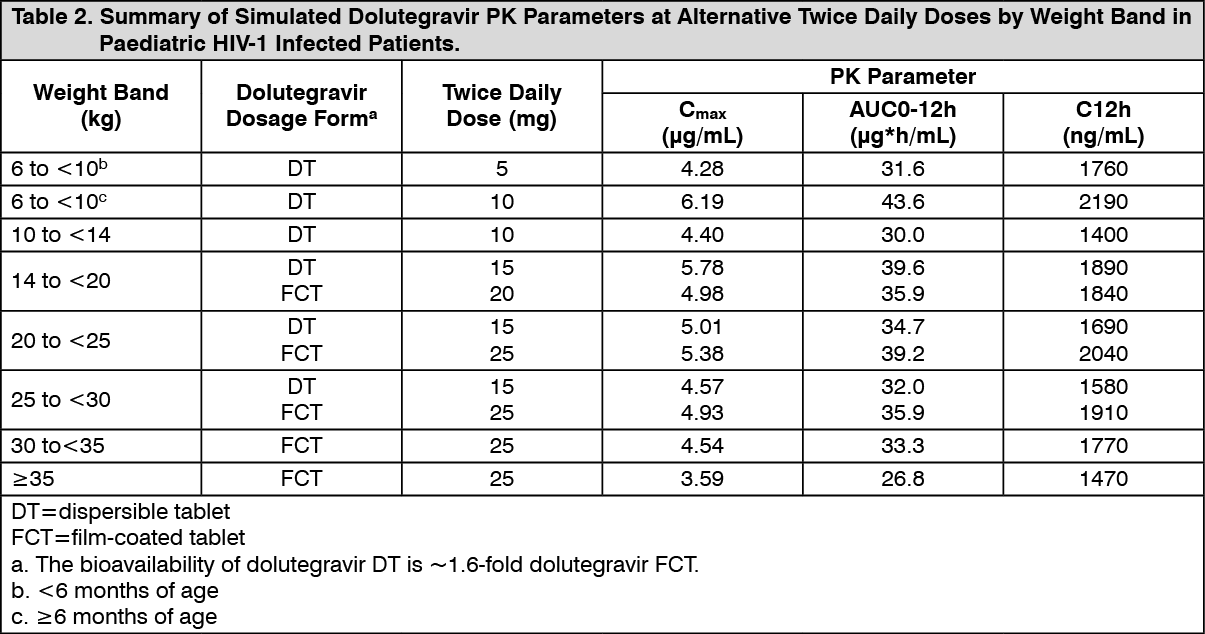 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageElderly: In HIV-1 infected adults showed that there was no clinically relevant effect of age on dolutegravir exposure.
Pharmacokinetic data for dolutegravir in patients >65 years of age are limited.
Renal impairment: Renal clearance of unchanged active substance is a minor pathway of elimination for dolutegravir. The exposure to dolutegravir was decreased by approximately 40% in patients with severe renal impairment. The mechanism for the decrease is unknown. No dosage adjustment is considered necessary for patients with renal impairment. There is no data of use of Dolutegravir in patients on dialysis.
Hepatic impairment: Dolutegravir is primarily metabolized and eliminated by the liver. While the total dolutegravir concentration in plasma was similar, a 1.5- to 2-fold increase in unbound exposure to dolutegravir was observed in patients with moderate hepatic impairment compared to healthy patients. No dosage adjustment is considered necessary for patients with mild to moderate hepatic impairment. There is no data on effect of severe hepatic impairment on the pharmacokinetics of Doluteragravir.
Polymorphisms in drug metabolising enzymes: There is no evidence that common polymorphisms in drug metabolising enzymes alter dolutegravir pharmacokinetics to a clinically meaningful extent. Patients with UGT1A1 genotypes conferring poor dolutegravir metabolism had a 32% lower clearance of dolutegravir and 46% higher AUC via UGT1A1.
Gender: There is no clinically relevant effect of gender on the exposure of dolutegravir.
Race: There is no clinically relevant effect of race on the exposure of dolutegravir. The pharmacokinetics of dolutegravir following single dose oral administration to Japanese patients appear similar to observed parameters in Western (US) patients.
Co-infection with Hepatitis B or C: Population pharmacokinetic analysis indicated that hepatitis C virus co-infection had no clinically relevant effect on the exposure to dolutegravir. There are limited data on patients with hepatitis B co-infection.