For this product, there is no modern clinical documentation which can be used as support for determining the frequency of undesirable effects. Undesirable effects may vary in their incidence depending on the dose received and also when given in combination with other therapeutic agents.
The following convention has been utilised for the classification of frequency: Very common (≥1/10), common (≥1/100 and <1/10), uncommon (≥1/1000 and <1/100), rare (≥1/10,000 and <1/1000), very rare (<1/10,000) and, Not known (cannot be estimated from the available data).
The following table of adverse reactions originated from the use of busulfan, or busulfan in combination with other therapeutic agents. (See Table 2.)
 Click on icon to see table/diagram/image
Description of selected adverse events: Blood and lymphatic system disorders:
Click on icon to see table/diagram/image
Description of selected adverse events: Blood and lymphatic system disorders: Aplastic anaemia (sometimes irreversible) has been reported rarely, typically following long-term conventional doses and also high doses of busulfan.
Respiratory, thoracic and mediastinal disorders: Pulmonary toxicity after either high or conventional dose treatment typically presents with non-specific non-productive cough, dyspnoea and hypoxia with evidence of abnormal pulmonary physiology. Other cytotoxic agents may cause additive lung toxicity (see Interactions). It is possible that subsequent radiotherapy can augment subclinical lung injury caused by busulfan. Once pulmonary toxicity is established the prognosis is poor despite busulfan withdrawal and there is little evidence that corticosteroids are helpful.
Idiopathic pneumonia syndrome is a non-infectious diffuse pneumonia which usually occurs within three months of high-dose busulfan conditioning prior to allogeneic or autologous haemopoietic transplant. Diffuse alveolar haemorrhage may also be detected in some cases after broncholavage. Chest X-rays or CT scans show diffuse or non-specific focal infiltrates and biopsy shows interstitial pneumonitis and diffuse alveolar damage and sometimes fibrosis.
Interstitial pneumonitis may occur following conventional dose use and lead to pulmonary fibrosis. This usually occurs after prolonged treatment over a number of years. The onset is usually insidious but may also be acute. Histological features include atypical changes of the alveolar and bronchiolar epithelium and the presence of giant cells with large hyperchromatic nuclei. The lung pathology may be complicated by superimposed infections. Pulmonary ossification and dystrophic calcification have also been reported.
Hepatobiliary disorders: Busulfan is not generally considered to be significantly hepatotoxic at normal therapeutic doses. However, retrospective review of post mortem reports of patients who had been treated with low-dose busulfan for at least two years for chronic myeloid leukaemia showed evidence of centrilobular sinusoidal fibrosis.
Skin and subcutaneous tissue disorders: Hyperpigmentation occurs, particularly in those with a dark complexion. It is often most marked on the neck, upper trunk, nipples, abdomen and palmar creases. This may also occur as part of a clinical syndrome (see General disorders and administration site conditions as follows).
Reproductive system and breast disorders: Studies of busulfan treatment in animals have shown reproductive toxicity (see Pharmacology: Toxicology: Non-Clinical Information under Actions).
General disorders and administration site conditions: Clinical syndrome (weakness, severe fatigue, anorexia, weight loss, nausea and vomiting and hyperpigmentation of the skin) resembling adrenal insufficiency (Addison's disease) but without biochemical evidence of adrenal suppression, mucous membrane hyperpigmentation or alopecia (see Skin and subcutaneous tissue disorders as previously mentioned) has been seen in a few cases following prolonged busulfan therapy. The syndrome has sometimes resolved when busulfan has been withdrawn.
Many histological and cytological changes have been observed in patients treated with busulfan, including widespread dysplasia affecting uterine cervical, bronchial and other epithelia. Most reports relate to long-term treatment but transient epithelial abnormalities have been observed following short-term, high-dose treatment.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image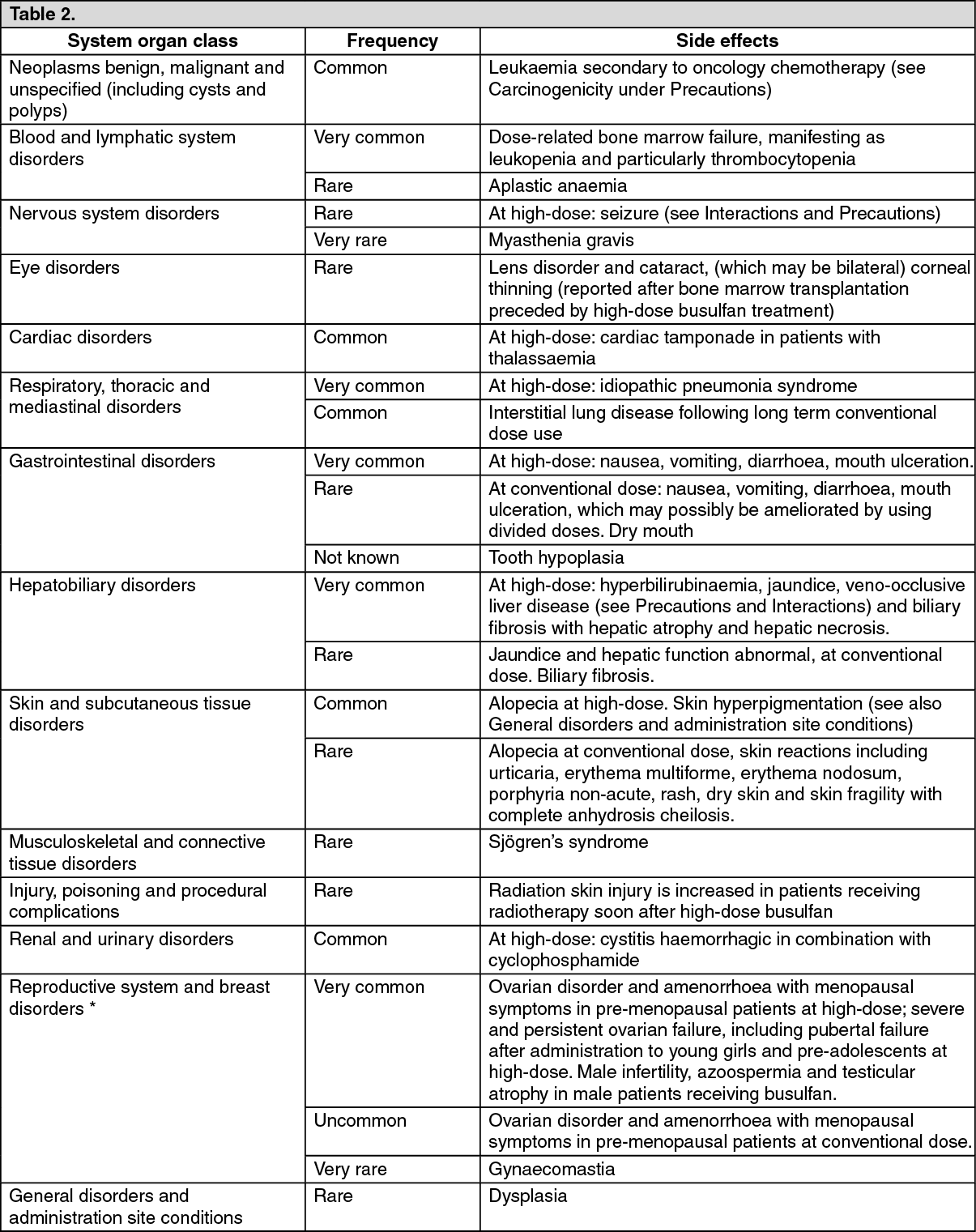 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
