


 Sign Out
Sign Out

Preventive or healing effects in gastritis models: Rebamipide inhibited the development of taurocholic acid-induced gastritis and promoted healing of the mucosal inflammation associated with gastritis in rat experiments.
Prostaglandin-increasing effect: Rebamipide increased the generation of prostaglandin E2 (PGE2) in the gastric mucosa in rats. The drug also increased the contents of PGE2, 15-keto-13, 14-dihydro-PGE2 (a metabolite of PGE2) and PGl2 in the gastric juice. In healthy male subjects, the drug again revealed the increasing effect on the PGE2 content in the gastric mucosa and protected the gastric mucosa from injury caused by ethanol loading.
Cytoprotective effect: Rebamipide exhibited a gastric cytoprotective effect to inhibit the mucosal injury induced by ethanol, strong acid, or strong base in rats. In in vitro studies, the drug also protected cultured gastric epithelial cells obtained from rabbit fetuses against aspirin- or taurocholic acid-induced injury.
In healthy male subjects, the drug inhibited gastric mucosal injury induced by aspirin, ethanol, or HCl-ethanol loading.
Mucus-increasing effect: Rebamipide promoted gastric enzyme activity to synthesize high molecular weight glycoproteins, thickened the superficial mucous layer of gastric mucosa, and increased the amount of gastric soluble mucus in rats. Endogenous PGs were not involved in the increase in soluble mucus.
Mucosal blood flow-increasing effect: Rebamipide increased gastric mucosal blood flow and improved impaired hemodynamics after blood loss in rats.
Effect on mucosal barrier: Rebamipide did not ordinarily affect the gastric transmucosal potential difference in rats, but did inhibit lowering of the potential difference by ethanol.
Effect on gastric alkaline secretion: Rebamipide promoted gastric alkaline secretion in rats.
Effect on mucosal cell turnover: Rebamipide activated gastric mucosal cell proliferation and increased the number of covering epithelial cells in rats.
Effect on gastric mucosal repair: Rebamipide restored the bile acid- or hydrogen peroxide-induced retardation of artificial wound-repair in cultured rabbit gastric epithelial cells.
Effect on gastric secretion: Rebamipide did not alter either basal secretion of gastric juice or secretagogue-stimulated acid secretion.
Effects on reactive oxygen species: Rebamipide scavenged hydroxyl radicals directly and suppressed superoxide production by polymorphonuclear leukocytes. The drug inhibited the gastric mucosal cell injury caused by reactive oxygen species released from neutrophils stimulated by Helicobacter pylori in vitro. The drug reduced the content of lipid peroxide in the gastric mucosa of rats treated with indomethacin under stressed conditions and inhibited the mucosal injury.
Effect on inflammatory cell infiltration in the gastric mucosa: Rebamipide prevented inflammatory cell infiltration in rat models of taurocholic acid-induced gastritis and NSAID-induced or ischemia reperfusion-induced gastric mucosal damage.
Effect on inflammatory cytokine release (interleukin-8) in the gastric mucosa: Rebamipide, taken by the oral route, suppressed the increased production of interleukin-8 in the mucosa of patients with Helicobacter pylori. The drug also inhibited the activation of NF-κB the expression of interleukin-8 mRNA, and the production of interleukin-8 in epithelial cells cocultured with Helicobacter pylori (in vitro).
Clinical Studies: Clinical Efficacy in Gastric Ulcer: MUCOSTA Tablets were studied in patients with gastric ulcer, using endoscopy for objective drug evaluation. In the final endoscopic assessment, the drug achieved complete healing in 60% (200/335) of the patients studied and near-complete healing in 67% (224/335). The clinical usefulness of this drug, based on efficacy and safety was demonstrated in a double-blind study. Six-month follow-up of 67 patients who showed healing at a daily dose of 300 mg revealed that recurrence occurred in only 4 patients (approx. 6%).
Clinical Efficacy in Acute Gastritis and Acute Exacerbation of Chronic Gastritis: MUCOSTA Tablets were studied in patients with acute gastritis or acute exacerbation of chronic gastritis. The drug achieved an 80% (370/461) global efficacy rate in the patients evaluated, with 76% (351 /461) showing moderate or marked improvement. The drug's clinical usefulness was found to be reproducible in a double-blind study.
Pharmacokinetics: Plasma Concentrations: The table as follow shows the pharmacokinetic parameters of rebamipide following single oral administration of MUCOSTA Tablets 100 at the dose of 100 mg to 27 healthy male subjects in a fasted state. (See Table 1.)
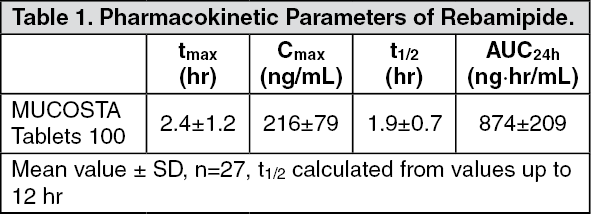 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe absorption of rebamipide following single oral administration at a dose of 150 mg to 6 healthy male subjects in a fed state tended to be slower than that in a fasted state. However, food did not affect bioavailability of the drug in humans. Pharmacokinetic parameters obtained from patients with renal impairment after single oral administration of rebamipide at 100 mg revealed higher plasma concentrations and a longer elimination half-life compared with those in healthy subjects. At steady state, rebamipide plasma concentrations observed in dialyzed renal patients following repeated administration were very close to the values simulated from single administration. Therefore, the drug was not considered to accumulate.
Metabolism: Rebamipide was primarily excreted as the unchanged compound in the urine after single oral administration to healthy adult males at a dose of 600 mg. A metabolite with a hydroxyl group at the 8th position was identified in the urine. However, the excretion of this metabolite was only 0.03% of the administered dose. The enzyme involved in the formation of the metabolite was CYP3A4.
(Note) The usual dosage in adults is 100 mg three times daily.
Excretion: Approximately 10% of the administered dose was excreted in the urine when rebamipide was administered as a single oral dose to healthy adult males at 100 mg.
Protein Binding: Rebamipide at 0.05 -5 μg/mL was added to human plasma in vitro, and 98.4%-98.6% of the drug was bound to plasma proteins.