Active Ingredient: Each film coated tablet contains: Moxifloxacin Hydrochloride: 436.8mg (eq. to Moxifloxacin 400mg).
Pharmacotherapeutic group: Quinolone antibacterials, fluoroquinolones. ATC code: J01MA14.
Pharmacodynamics: Mechanism of action: Moxifloxacin is active against a wide range of Gram-positive and Gram-negative pathogens.
The bactericidal action of moxifloxacin results from the inhibition of both type II topoisomerases (DNA gyrase and topoisomerase IV) required for bacterial DNA replication, transcription and repair. It appears that the C8-methoxy moiety contributes to enhanced activity and lower selection of resistant mutants of Gram-positive bacteria compared to the C8-H moiety. The presence of the bulky bicycloamine substituent at the C-7 position prevents active efflux, associated with the norA or pmrA genes seen in certain Gram-positive bacteria.
Moxifloxacin exhibits a concentration dependent killing rate.
Mechanism of resistance: Resistance mechanisms that inactivate penicillins, cephalosporins, aminoglycosides, macrolides and tetracyclines do not interfere with the antibacterial activity of moxifloxacin. Other resistance mechanisms such as permeation barriers (common in Pseudomonas aeruginosa) and efflux mechanisms may also effect susceptibility to moxifloxacin.
Moxifloxacin is a poor substrate for active efflux mechanisms in Gram-positive organisms.
Moxifloxacin inhibits both topoisomerase II and IV with similar activity in some Gram-positive bacteria, such bacteria may be resistant to other quinolones, but susceptible to moxifloxacin.
Microbiological Susceptibility: The prevalence of acquired resistance may vary geographically and with time for selected species and local information of resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought where the local prevalence of resistance is such that utility of the agent in at least some types of infections is questionable.
Pharmacokinetics: Absorption and Bioavailability: Following oral administration moxifloxacin is rapidly and almost completely absorbed. The absolute bioavailability amounts to approximately 91%.
Pharmacokinetics are linear in the range of 50 - 800 mg single dose and up to 600 mg once daily dosing over 10 days. Following a 400 mg oral dose peak concentrations of 3.1 mg/l are reached within 0.5 - 4 h post administration. Peak and trough plasma concentrations at steady-state (400 mg once daily) were 3.2 and 0.6 mg/l, respectively. At steady-state the exposure within the dosing interval is approximately 30% higher than after the first dose.
Distribution: Moxifloxacin is distributed to extravascular spaces rapidly; after a dose of 400 mg an AUC of 35 mgh/l is observed. The steady state volume of distribution (Vss) is approximately 2 l/kg. Moxifloxacin shows protein binding of approximately 40 - 42% independent of the concentration of the drug. Moxifloxacin is mainly bound to serum albumin.
Biotransformation: Moxifloxacin undergoes Phase II biotransformation and is excreted via renal and biliary/faecal pathways as unchanged drug as well as in the form of a sulpho-compound (M1) and a glucuronide (M2), both are microbiologically inactive.
Elimination: Moxifloxacin is eliminated from plasma with a mean terminal half-life of approximately 12 hours.
Concomitant administration of moxifloxacin with ranitidine or probenecid did not alter renal clearance of the parent drug.
Elderly and patients with low body weight: Higher plasma concentrations are observed in healthy volunteers with low body weight (such as women) and in elderly volunteers.
Renal impairment: The pharmacokinetic properties of moxifloxacin are not significantly different in patients with renal impairment (including creatinine clearance >20ml/min/1.73m2). As renal function decreases, concentrations of the M2 metabolite (glucuronide) increase by up to a factor of 2.5 (with a creatine clearance of <30ml/min/1.73m2).
Hepatic impairment: On the basis of the pharmacokinetic studies carried out so far in patients with liver failure (Child Pugh A, B), it is not possible to determine whether there are any differences compared with healthy volunteers. Impaired liver function was associated with higher exposure to M1 in plasma, whereas exposure to parent drug was comparable to exposure in healthy volunteers. There is insufficient experience in the clinical use of moxifloxacin in patients with impaired liver function.
Moxifloxacin tablets are indicated for the treatment of adults (> 18 years of age) with the following bacterial infections caused by susceptible strains: Acute sinusitis*; Acute exacerbations of chronic bronchitis*; Community acquired pneumonia; Mild to moderately severe inflammatory pelvic diseases (i.e. Infections of the upper female genital tract, including salpingitis and endometritis), without an associated tubo-ovarian or pelvic abscess.
Moxifloxacin 400 mg film-coated tablets are not recommended for monotherapy of mild to moderately severe inflammatory pelvic diseases. Preferably, they should be administered in combination with another suited antibiotic (such as cephalosporin), due to the increasing resistance of Neisseria gonorrhoeae to moxifloxacin; that is, unless moxifloxacin-resistant Neisseria gonorrhoeae can be ruled out: Complicated skin and skin structure infections; Complicated intra-abdominal infections including polymicrobial infections such as abscesses.
*Moxifcin film coated tablet 400mg should be only used: When Pseudomonas is considered AND the patient is allergic to antipseudomonal penicillins/cephalosporins; For resistant organisms with no other alternative antibiotics available.
Consideration should be given to official guidance on the appropriate use of antibacterial agents.
Dose (adults): The recommended dose for Moxifloxacin is 400mg once daily (1 film-coated tablet) for the previously mentioned indications and should not be exceeded.
Duration of treatment: The duration of treatment should be determined by the severity of the indication or clinical response.
The following general recommendations for the treatment of upper and lower respiratory tract infections are made: Bronchitis: acute exacerbation of chronic bronchitis, 5 days.
Pneumonia: community acquired pneumonia, 10 days.
Sinusitis: acute sinusitis, 7 days.
Mild to moderately severe inflammatory pelvic diseases: 14 days.
Complicated skin and skin structure infections total treatment duration for sequential therapy (intravenous followed by oral therapy): 7 - 21 days.
Complicated intraabdominal infections total treatment duration for sequential therapy (intravenous followed by oral therapy): 5 - 14 days.
The recommended duration of treatment for the indication being treated should not be exceeded.
Geriatric patients: No adjustment of dosage is required in the elderly.
Pediatric Patients: The efficacy of Moxifloxacin in children and adolescents has not been established. No recommendation on posology can be made. The safety of Moxifloxacin in children below the age of 6 years has not been established.
Ethnic differences: No adjustment of dosage is required in ethnic groups.
Patients with hepatic impairment: No dosage adjustment is required in patients with impaired liver function.
Patients with renal impairment: No dose adjustment is required in patients with renal impairment (including creatinine clearance < 30mL/min/1.73m2) and in patients on chronic dialysis i.e. hemodialysis and continuous ambulatory peritoneal dialysis.
Route of Administration: For oral use. The film-coated tablet should be swallowed whole with sufficient liquid/water and may be taken independent of meals.
Symptoms: See Adverse Reactions.
Treatment: No specific counter measures after accidental overdose are recommended. In the event of overdose, symptomatic treatment should be implemented. ECG monitoring should be undertaken, because of the possibility of QT interval prolongation.
Concomitant administration of charcoal with a dose of 400 mg oral moxifloxacin will reduce systemic availability of the drug by more than 80%. The use of charcoal early during absorption may be useful to prevent excessive increase in the systemic exposure to moxifloxacin in cases of oral overdose.
Hypersensitivity to moxifloxacin, other quinolones or to any of the excipients.
Pregnancy and lactation.
Patients below 18 years of age.
Patients with a history of tendon disease/disorder related to quinolone treatment.
Changes in cardiac electrophysiology have been observed following exposure to moxifloxacin, in the form of QT prolongation. For reasons of drug safety, moxifloxacin is therefore contraindicated in patients with: Congenital or documented acquired QT prolongation; Electrolyte disturbances, particularly in uncorrected hypokalaemia; Bradycardia; Heart failure with reduced left-ventricular ejection fraction; Previous history of symptomatic arrhythmias.
Moxifloxacin should not be used concurrently with other drugs that prolong the QT interval.
Moxifloxacin is also contraindicated in patients with impaired liver function (Child Pugh C) and in patients with transaminases increase > 5 fold ULN.
The use of moxifloxacin should be avoided in patients who have experienced serious adverse reactions in the past when using quinolone or fluoroquinolone containing products (see Adverse Reactions). Treatment of these patients with moxifloxacin should only be initiated in the absence of alternative treatment options and after careful benefit/risk assessment.
The benefit of moxifloxacin treatment especially in infections with a low degree of severity should be balanced with the information as follows.
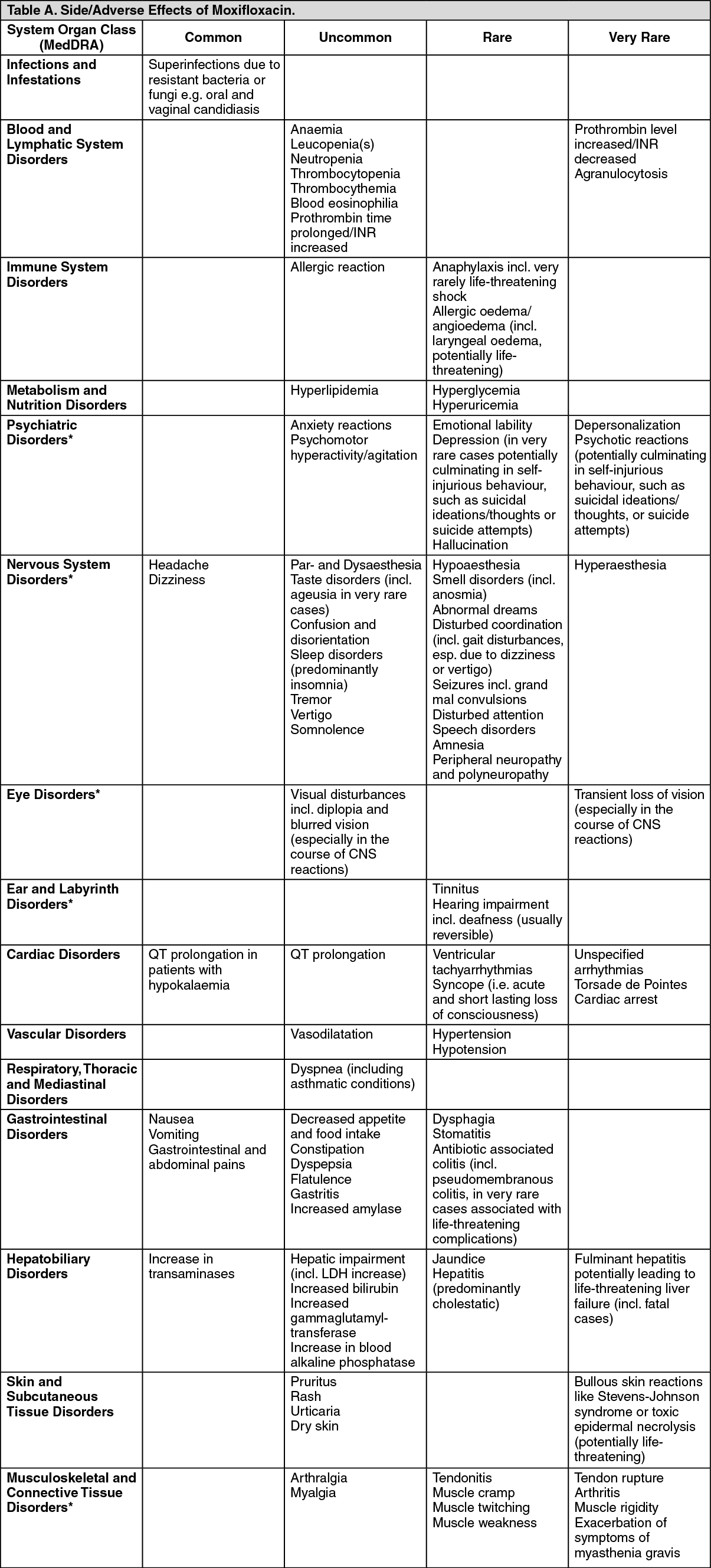
Prolonged, disabling and potentially irreversible serious adverse drug reactions: Very rare cases of prolonged (continuing months or years), disabling and potentially irreversible serious adverse drug reactions affecting different, sometimes multiple, body systems (musculoskeletal, nervous, psychiatric and senses) have been reported in patients receiving quinolones and fluoroquinolones irrespective of their age and pre-existing risk factors. Moxifloxacin should be discontinued immediately at the first signs or symptoms of any serious adverse reaction and patients should be advised to contact their prescriber for advice.
Prolongation of QTc interval and potentially QTc-prolongation-related clinical conditions: Moxifloxacin has been shown to prolong the QTc interval on the electrocardiogram. Medication that can reduce potassium levels should be used with caution in patients receiving moxifloxacin.
Moxifloxacin should be used with caution in patients with ongoing proarrhythmic conditions (especially women and elderly patients), such as acute myocardial ischaemia or QT prolongation as this may lead to an increased risk for ventricular arrhythmias (incl. torsade de pointes) and cardiac arrest. The magnitude of QT prolongation may increase with increasing concentrations of the drug. Therefore, the recommended dose should not be exceeded.
If signs of cardiac arrhythmia occur during treatment with moxifloxacin, treatment should be stopped and an ECG should be performed.
Hypersensitivity/allergic reactions: Hypersensitivity and allergic reactions have been reported for fluoroquinolones including moxifloxacin after first administration. Anaphylactic reactions can progress to a life-threatening shock, even after the first administration. In cases of clinical manifestations of severe hypersensitivity reactions moxifloxacin should be discontinued and suitable treatment (e.g. treatment for shock) initiated.
Severe liver disorders: Cases of fulminant hepatitis potentially leading to liver failure (including fatal cases) have been reported with moxifloxacin. Patients should be advised to contact their doctor prior to continuing treatment if signs and symptoms of fulminant hepatic disease develop such as rapidly developing asthenia associated with jaundice, dark urine, bleeding tendency or hepatic encephalopathy.
Liver function tests/investigations should be performed in cases where indications of liver dysfunction occur.
Exacerbation of myasthenia gravis: Fluoroquinolones have neuromuscular blocking activity and may exacerbate muscle weakness in person with myasthenia gravis. Post marketing serious adverse events, including deaths and requirement for ventilator support have been associated with fluoroquinolones use in persons with myasthenia gravis. Avoid fluoroquinolones in patients with known history of myasthenia gravis.
Patients with myasthenia gravis: Moxifloxacin should be used with caution in patients with myasthenia gravis because the symptoms can be exacerbated.
Serious bullous skin reactions: Cases of bullous skin reactions like Stevens-Johnson syndrome or toxic epidermal necrolysis have been reported with moxifloxacin. Patients should be advised to contact their doctor immediately prior to continuing treatment if skin and/or mucosal reactions occur.
Patients predisposed to seizures: Quinolones are known to trigger seizures. Use should be with caution in patients with CNS disorders or in the presence of other risk factors which may predispose to seizures or lower the seizure threshold. In case of seizures, treatment with moxifloxacin should be discontinued and appropriate measures instituted.
Peripheral neuropathy: Cases of sensory or sensorimotor polyneuropathy resulting in paraesthesia, hypoaesthesia, dysaesthesia, or weakness have been reported in patients receiving quinolones and fluoroquinolones. Patients under treatment with moxifloxacin should be advised to inform their doctor prior to continuing treatment if symptoms of neuropathy such as pain, burning, tingling, numbness, or weakness develop in order to prevent the development of potentially irreversible condition (see Adverse Reactions).
Psychiatric reactions: Psychiatric reactions may occur even after the first administration of quinolones, including moxifloxacin. In very rare cases depression or psychotic reactions have progressed to suicidal thoughts and self-injurious behaviour such as suicide attempts. In the event that the patient develops these reactions, moxifloxacin should be discontinued and appropriate measures instituted. Caution is recommended if moxifloxacin is to be used in psychotic patients or in patients with history of psychiatric disease.
Severe cutaneous adverse reactions: Severe cutaneous adverse reactions (SCARs) including toxic epidermal necrolysis (TEN: also known as Lyell's syndrome), Stevens Johnson syndrome (SJS) and Acute Generalised Exanthematous Pustulosis (AGEP), which could be life-threatening or fatal, have been reported with moxifloxacin. At the time of prescription, patients should be advised of the signs and symptoms of severe skin reactions and be closely monitored. If signs and symptoms suggestive of these reactions appear, moxifloxacin should be discontinued immediately, and an alternative treatment should be considered. If the patient has developed a serious reaction such as SJS, TEN or AGEP with the use of moxifloxacin, treatment with moxifloxacin must not be restarted in this patient at any time.
Antibiotic-associated diarrhoea incl. colitis: Antibiotic-associated diarrhoea (AAD) and antibiotic-associated colitis (AAC), including pseudomembranous colitis and Clostridium difficile-associated diarrhoea, has been reported in association with the use of broad spectrum antibiotics including moxifloxacin and may range in severity from mild diarrhoea to fatal colitis.
Therefore it is important to consider this diagnosis in patients who develop serious diarrhoea during or after the use of moxifloxacin. If AAD or AAC is suspected or confirmed, ongoing treatment with antibacterial agents, including moxifloxacin, should be discontinued and adequate therapeutic measures should be initiated immediately. Furthermore, appropriate infection control measures should be undertaken to reduce the risk of transmission. Drugs inhibiting peristalsis are contraindicated in patients who develop serious diarrhoea.
Tendinitis and tendon rupture: Tendinitis and tendon rupture (especially but not limited to Achilles tendon), sometimes bilateral, may occur as early as within 48 hours of starting treatment with fluoroquinolones and have been reported to occur even up to several months after discontinuation of treatment. The risk of tendinitis and tendon rupture is increased in older patients (above 60 years of age), with renal impairment, patients with solid organ transplants, and those treated concurrently with corticosteroids. Therefore, concomitant use of corticosteroids should be avoided.
At the first sign of tendinitis (e.g. painful swelling, inflammation) the treatment with moxifloxacin should be discontinued and alternative treatment should be considered. The affected limb(s) should be appropriately treated (e.g. immobilisation). Corticosteroids should not be used if signs of tendinopathy occur.
Aortic aneurysm and dissection: Epidemiologic studies report an increased risk of aortic aneurysm and dissection after intake of fluoroquinolones, particularly in the older population. Therefore, fluoroquinolones should only be used after careful benefit-risk assessment and after consideration of other therapeutic options in patients with positive family history of aneurysm disease, or in patients diagnosed with pre-existing aortic aneurysm and/or aortic dissection, or in presence of other risk factors or conditions predisposing for aortic aneurysm and dissection (e.g. Marfan syndrome, vascular Ehlers-Danlos syndrome, Takayasu arteritis, giant cell arteritis, Behcet's disease, hypertension, known atherosclerosis). In case of sudden abdominal, chest or back pain, patients should be advised to immediately consult a physician in an emergency department.
Vision disorders: If vision becomes impaired or any effects on the eyes are experienced, an eye specialist should be consulted immediately.
Dysglycemia: As with all fluoroquinolones, disturbances in blood glucose, including both hypoglycemia and hyperglycemia have been reported with moxifloxacin. In moxifloxacin-treated patients, dysglycemia occurred predominantly in elderly diabetic patients receiving concomitant treatment with an oral hypoglycemic agent (e.g. sulfonylurea) or with insulin. Cases of hypoglycaemic coma have been reported. In diabetic patients, careful monitoring of blood glucose is recommended.
Prevention of photosensitivity reactions: Quinolones have been shown to cause photosensitivity reactions in patients. However, studies have shown that moxifloxacin has a lower risk to induce photosensitivity. Nevertheless patients should be advised to avoid exposure to either UV irradiation or extensive and/or strong sunlight during treatment with moxifloxacin.
Patients with glucose-6-phosphate dehydrogenase deficiency: Patients with a family history of, or actual glucose-6-phosphate dehydrogenase deficiency are prone to haemolytic reactions when treated with quinolones. Therefore, moxifloxacin should be used with caution in these patients.
Patients with pelvic inflammatory disease: For patients with complicated pelvic inflammatory disease (e.g. associated with a tubo-ovarian or pelvic abscess), for whom an intravenous treatment is considered necessary, treatment with Moxifcin F.C. Tablet 400mg is not recommended.
Pelvic inflammatory disease may be caused by fluoroquinolone-resistant Neisseria gonorrhoeae. Therefore in such cases empirical moxifloxacin should be co-administered with another appropriate antibiotic (e.g. a cephalosporin) unless moxifloxacin-resistant Neisseria gonorrhoeae can be excluded. If clinical improvement is not achieved after 3 days of treatment, the therapy should be reconsidered.
Patients with special cSSSI: Clinical efficacy of intravenous moxifloxacin in the treatment of severe burn infections, fasciitis and diabetic foot infections with osteomyelitis has not been established.
Interference with biological tests: Moxifloxacin therapy may interfere with the Mycobacterium spp. culture test by suppression of mycobacterial growth causing false negative results in samples taken from patients currently receiving moxifloxacin.
Patients with MRSA infections: Moxifloxacin is not recommended for the treatment of MRSA infections. In case of a suspected or confirmed infection due to MRSA, treatment with an appropriate antibacterial agent should be started.
Information about excipients: Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Effects on Ability to Drive and Use Machine: No studies on the effects of moxifloxacin on the ability to drive and use machines have been performed.
However, fluoroquinolones including moxifloxacin may result in an impairment of the patient's ability to drive or operate machinery due to CNS reactions (e.g. dizziness; acute, transient loss of vision) or acute and short lasting loss of consciousness (syncope). Patients should be advised to see how they react to moxifloxacin before driving or operating machinery.
Patients with renal impairment: Elderly patients with renal disorders should use moxifloxacin with caution if they are unable to maintain adequate fluid intake, because dehydration may increase the risk of renal failure.
Use in Children: Due to adverse effects on the cartilage in juvenile animals, the use of moxifloxacin in children and adolescents < 18 years is contraindicated.
Pregnancy, Breastfeeding: The safety of moxifloxacin in human pregnancy, lactating or nursing women has not been evaluated. Therefore, moxifloxacin must not be used in pregnant women.
Tabulated list of adverse reactions: (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Reporting of suspected adverse reactions:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
An additive effect on QT interval prolongation of moxifloxacin and other medicinal products that may prolong the QTc interval cannot be excluded. This might lead to an increased risk of ventricular arrhythmias, including torsade de pointes. Therefore, co-administration of moxifloxacin with any of the following medicinal products is contraindicated: anti-arrhythmics class IA (e.g. quinidine, hydroquinidine, disopyramide); anti-arrhythmics class III (e.g. amiodarone, sotalol, dofetilide, ibutilide); antipsychotics (e.g. phenothiazines, pimozide, sertindole, haloperidol, sultopride); tricyclic antidepressive agents; certain antimicrobial agents (saquinavir, sparfloxacin, erythromycin IV, pentamidine, antimalarials particularly halofantrine); certain antihistaminics (terfenadine, astemizole, mizolastine); others (cisapride, vincamine IV, bepridil, diphemanil).
Moxifloxacin should be used with caution in patients who are taking medication that can reduce potassium levels (e.g. loop and thiazide-type diuretics, laxatives and enemas [high doses], corticosteroids, amphotericin B) or medication that is associated with clinically significant bradycardia.
An interval of about 6 hours should be left between administration of agents containing bivalent or trivalent cations (e.g. antacids containing magnesium or aluminium, didanosine tablets, sucralfate and agents containing iron or zinc) and administration of moxifloxacin.
Concomitant administration of charcoal with an oral dose of 400 mg moxifloxacin led to a pronounced prevention of drug absorption and a reduced systemic availability of the drug by more than 80%. Therefore, the concomitant use of these two drugs is not recommended.
A large number of cases showing an increase in oral anticoagulant activity have been reported in patients receiving antibacterial agents. A precautionary measure would be to more frequently monitor the INR. If necessary, the oral anticoagulant dosage should be adjusted as appropriate.
Store at temperature below 30°C. Protect from moisture.
Shelf Life: 3 years.
J01MA14 - moxifloxacin ; Belongs to the class of fluoroquinolones. Used in the systemic treatment of infections.
Moxifcin FC tab 400 mg
1 × 5's;10 × 10's;10 × 5's;2 × 5's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image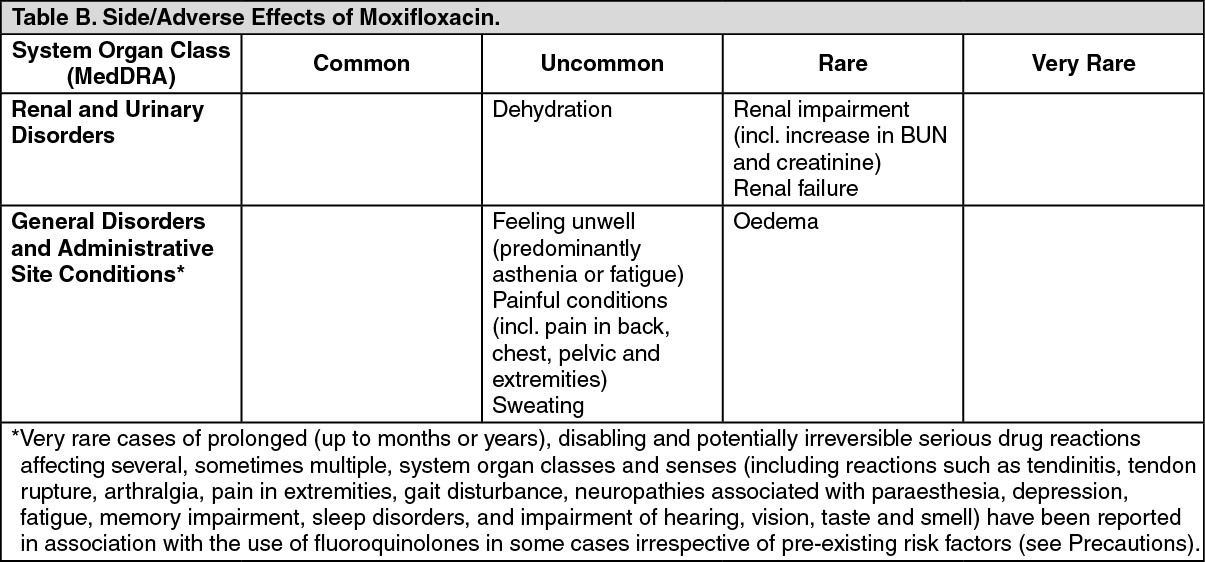 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
