Ethinylestradiol, gestodene.
Each MINULET package contains 21 tablets, each containing 30 mcg ethinyl estradiol and 75 mcg gestodene.
Ethinyl estradiol is a white to creamy white, odorless, crystalline powder. It is insoluble in water and soluble in alcohol, chloroform, ether, vegetable oils, and aqueous solutions of alkali hydroxides.
Gestodene is a white to off-white crystalline powder that is easily soluble in chloroform and dioxane and soluble in acetone and methanol.
Pharmacological class, therapeutic class: Estrogen-progestin combination oral contraceptive (COC)
Pharmacology: Mode of action: COCs suppress gonadotropins in a manner that inhibits ovulation, which leads to contraception.
Pharmacodynamics, clinical efficacy: When taken consistently and correctly, the probable failure rate of COCs is 0.1% per year; however, the failure rate during typical use is 5% per year for all types of oral contraceptives. The efficacy of most methods of contraception depends upon the reliability with which they are used. Method failure is more likely if COC tablets are missed.
Pharmacokinetics: Ethinyl estradiol and gestodene are rapidly and almost completely absorbed from the gastrointestinal tract.
Peak plasma levels of each drug are reached within 1-2 hours. Post maximum concentration curves show two phases with half-lives of 1 and 15 hours in the case of gestodene and 1-3 and approximately 24 hours in the case of ethinyl estradiol.
After oral administration, gestodene unlike ethinyl estradiol is not subject to first-pass metabolism. Following oral administration, gestodene is completely bioavailable, ethinyl estradiol about 40%.
Gestodene is extensively plasma protein bound to sex hormone binding globulin (SHBG). Ethinyl estradiol is bound in plasma to albumin and enhances the binding capacity of SHBG.
The elimination half-life for ethinyl is approximately 25 hours. It is primarily metabolized by aromatic hydroxylation but a wide variety of hydroxylated and methylated metabolites are formed, and these are present both free and as conjugates with glucuronide and sulfate. Conjugated ethinyl estradiol is excreted in bile and subject to enterohepatic recirculation. About 40% of the drug is excreted in the urine and 60% is eliminated in the feces.
The elimination half-life for gestodene is approximately 16-18 hours after multiple oral doses. The drug is primarily metabolized by reduction of the A ring followed by glucuronidation. About 50% of gestodene is excreted in the urine and 33% is eliminated in the feces.
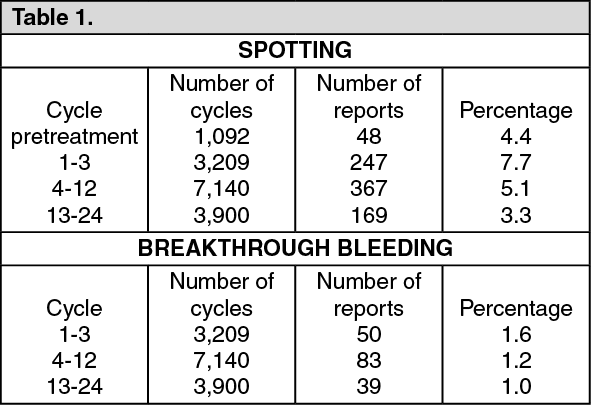
Cycle Control In Clinical Trials: In clinical trials with MINULET including 14,281 cycles of treatment, the overall incidence of spotting was 5.0% and breakthrough bleeding was 0.7%. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Amenorrhea (absence of expected withdrawal bleeding), occurred in 68 of 14,281 treatment cycles, an incidence of 0.5%.
Influence of Missed Tablets: The following table shows that the rate of intermenstrual bleeding is increased by intake errors, i.e., when one or more tablets are omitted. (See Table 2.)
Click on icon to see table/diagram/image
MINULET is indicated for the prevention of pregnancy.
Do not initiate or continue the use of "MINULET" if pregnancy is known or suspected.
How to take "MINULET": Tablets 1-21 contain active ingredients (active tablets).
Tablets must be taken in the order directed on the package every day at about the same time. One active tablet is to be taken daily for 21 consecutive days, a 7-day tablet-free interval. Each subsequent pack is started on the day after the tablet-free interval. A withdrawal bleed usually starts on days 2-3, after the last active tablet, and may not have finished before the next pack is started.
How to start "MINULET": No hormonal contraceptive use within the preceding month: The user should begin taking "MINULET" on Day 1 of her natural menstrual cycle (i.e., the first day of menstrual bleeding).
Beginning "MINULET" use on days 2-7 of the menstrual cycle (e.g., Sunday start) is allowed; however, a nonhormonal back-up method of birth control (e.g., condoms, spermicide) is recommended during the first 7 days of "MINULET" use.
Switching from another COC: Preferably, "MINULET" use should begin the day after the last active tablet of the previous COC pack has been taken but no later than the day following the usual tablet-free or inactive tablet interval of the previous COC.
Switching from a progestin-only method of birth control (pill, implant, intrauterine device [IUD], injection): The user may discontinue use of a progestin-only pill on any day; use of "MINULET" should begin the following day.
"MINULET" use should begin on the same day that a progestin-only implant or a progestin-only IUD is removed.
"MINULET" use should begin on the day that the next progestin-only injection is scheduled.
In each of these situations, the user should be advised to use a nonhormonal back-up method of birth control during the first 7 days of "MINULET" use.
Following first-trimester abortion: "MINULET" use may begin immediately. Additional contraceptive measures are not needed.
Postpartum: Because the immediate postpartum period is associated with an increased risk of thromboembolism, "MINULET" use should begin no sooner than the 28th postpartum day following either delivery in a nonlactating woman or second-trimester abortion. The woman should be advised to use a nonhormonal back-up method of birth control during the first 7 days of "MINULET" use. However, if intercourse has already occurred, pregnancy must be ruled out before "MINULET" use is begun; otherwise, the woman must wait until the first menstrual period before beginning "MINULET" use. See Special Warnings: Venous and arterial thrombosis and thromboembolism under Precautions and Lactation under Use in Pregnancy & Lactation.
Management of missed tablets: Contraceptive protection may be reduced if active tablets are missed, particularly if the missing of tablets extends the "tablet-free" interval.
If one active tablet is missed but is remembered within 12 hours of the usual dose, it should be taken as soon as it is remembered. Subsequent tablets should be taken at the usual time.
If one active tablet is missed and is remembered more than 12 hours after the usual dose or if two or more active tablets are missed, contraceptive protection may be reduced. The last missed tablet should be taken as soon as it is remembered, which may result in the user taking two tablets on the same day. Subsequent tablets should be taken at the usual time. A nonhormonal back-up method of birth control must be used for the next 7 days.
If the user takes the last active tablet before the 7-day interval during which use of a nonhormonal back-up method of birth control is required has ended, the patient must begin a new pack immediately; there should be no tablet-free interval between packs. This prevents an extended break in the tablet-taking interval, thereby reducing the risk of escape ovulation. The user is unlikely to have a withdrawal bleed until all tablets in the new pack are taken, although the patient may experience spotting or breakthrough bleeding on tablet-taking days. If the user does not have a withdrawal bleed after all tablets in the new pack are taken, pregnancy must be ruled out before tablet taking is resumed.
Advice in case of vomiting and/or diarrhea: If vomiting or diarrhea occurs within 4 hours after tablet taking, tablet absorption may be incomplete. Use of tablets from a back-up pack is required, as outlined as follows. Refer to recommendations for MANAGEMENT OF MISSED TABLETS as previously mentioned.
For Monophasic COCs: The user must take the needed active tablet(s) from a back-up pack.
How to delay a period: For Monophasic COCs: To delay a menstrual period, the user should skip the "tablet-free" interval and immediately begin a new pack of "MINULET". The delay may be continued for as long as desired up until all tablets in the new pack are taken. During the delay, the user may experience breakthrough bleeding or spotting. Regular intake of "MINULET" should be resumed after the usual 7-day "tablet-free" interval.
Symptoms of oral contraceptive overdosage in adults and children may include nausea, vomiting, breast tenderness, dizziness, abdominal pain, drowsiness/fatigue; withdrawal bleeding may occur in females. There is no specific antidote and further treatment of overdose, if necessary, is directed to the symptoms.
MINULET must not be used in women with any of the following conditions: Deep vein thrombosis (current or history).
Thromboembolism (current or history).
Cerebrovascular or coronary-artery disease.
Thrombogenic valvulopathies.
Thrombogenic rhythm disorders.
Hereditary or acquired thrombophilias.
Headache with focal neurological symptoms, such as aura.
Diabetes with vascular involvement.
Uncontrolled hypertension.
Known or suspected carcinoma of the breast, or other known or suspected estrogen dependent neoplasia.
Hepatic adenomas or carcinomas, or active liver disease, as long as liver function has not returned to normal.
Undiagnosed vaginal bleeding.
Pancreatitis associated with severe hypertriglyceridemia (current or history).
Known or suspected pregnancy.
Hypersensitivity to any of the components of MINULET.
MINULET is contraindicated for concomitant use with the medicinal products containing ombitasvir, paritaprevir, ritonavir and dasabuvir (see Special Warnings: Hepatic neoplasia/liver disease/hepatitis C under Precautions and Interactions).
Reasons for Immediate Discontinuation of MINULET: The occurrence for the first time of migrainous headaches or the more frequent occurrence of unusually severe headaches.
Acute disturbances of vision, hearing or other perceptual disorders.
First symptoms of thrombophlebitis or thromboembolism.
Development of jaundice (cholestasis), anicteric hepatitis or generalized pruritus.
Increase in epileptic seizures.
Significant rise in blood pressure.
Pregnancy.
Special Warnings: Cigarette smoking increases the risk of serious cardiovascular adverse reactions from COC use. This risk increases with age and with the extent of smoking (in epidemiology studies, smoking 15 or more cigarettes per day was associated with a significantly increased risk), and is quite marked in women over 35 years of age. Women who use COCs should be strongly advised not to smoke.
Venous and arterial thrombosis and thromboembolism: Use of COCs is associated with an increased risk of venous and arterial thrombotic and thromboembolic events.
Minimizing exposure to estrogens and progestins is in keeping with good principles of therapeutics. For any particular estrogen/progestin combination, the dosage regimen prescribed should be one which contains the least amount of estrogen and progestin that is compatible with a low failure rate and the needs of the individual patient.
New acceptors of COCs should be started on preparations containing less than 50 μg of estrogen.
Venous thrombosis and thromboembolism: Use of COCs increases the risk of venous thrombotic and thromboembolic events. Reported events include deep venous thrombosis and pulmonary embolism. For information on retinal vascular thrombosis see Ocular lesions as follows.
The use of any COC carries an increased risk of venous thrombotic and thromboembolic events compared with no use. The excess risk is highest during the first year a woman ever uses a combined oral contraceptive. This increased risk is less than the risk of venous thrombotic and thromboembolic events associated with pregnancy which is estimated as 60 cases per 100,000 women-years. Venous thromboembolism is fatal in 1% to 2% of cases.
Epidemiological studies have shown that the incidence of venous thromboembolism in users of low-estrogen oral contraceptives (<50 mcg ethinyl estradiol) ranges from about 20 to 40 cases per 100,000 women-years; this risk estimate varies according to the progestin. This compares with 5 to 10 cases per 100,000 women-years for non-users.
Several epidemiological studies have demonstrated that women who use COCs that contain ethinyl estradiol (particularly 30 μg) and a progestin such as gestodene are at increased risk for venous thrombotic and thromboembolic events compared with women who use COCs that contain less than 50 μg of ethinyl estradiol and the progestin levonorgestrel. However, data from other studies have not shown this increased risk.
For COCs containing 30 μg of ethinyl estradiol combined with desogestrel or gestodene compared with those containing less than 50 μg of ethinyl estradiol and levonorgestrel, the overall relative risk of venous thrombotic and thromboembolic events has been estimated to range between 1.5 and 2.0. The incidence of venous thrombotic and thromboembolic events for levonorgestrel-containing COCs with less than 50 μg of ethinyl estradiol is approximately 20 cases per 100,000 woman-years of use. For MINULET, the incidence is approximately 30-40 cases per 100,000 women-years of use, i.e., additional 10-20 cases per 100,000 woman-years of use.
All this information should be taken into account when prescribing this COC. When counseling on the choice of contraceptive method(s) all of the previously mentioned information should be considered.
The risk of venous thrombotic and thromboembolic events is further increased in women with conditions predisposing for venous thrombosis and thromboembolism. Caution must be exercised when prescribing COCs for such women.
Examples of predisposing conditions for venous thrombosis and thromboembolism are: obesity; surgery or trauma with increased risk of thrombosis; recent delivery or second-trimester abortion; prolonged immobilization; increasing age.
Further risk factors, which represent contraindications for the use of COCs, are listed in Contraindications.
The relative risk of postoperative thromboembolic complications has been reported to be increased two- to four-fold with the use of COCs. The relative risk of venous thrombosis in women with predisposing conditions is twice that of women without such conditions. If feasible, COCs should be discontinued: for four weeks prior to and for two weeks after elective surgery with increased risk of thrombosis, and during prolonged immobilization.
Because the immediate post-partum period is associated with an increased risk of thromboembolism, COC use should begin no sooner than the 28th postpartum day following either delivery in a nonlactating woman or second-trimester abortion.
Arterial thrombosis and thromboembolism: The use of COCs increases the risk of arterial thrombotic and thromboembolic events. Reported events include myocardial infarction and cerebrovascular events (ischemic and hemorrhagic stroke, transient ischemic attack). For information on retinal vascular thrombosis see Ocular lesions as follows.
The risk of arterial thrombotic and thromboembolic events is further increased in women with underlying risk factors.
Caution must be exercised when prescribing COCs for women with risk factors for arterial thrombotic and thromboembolic events.
Examples of risk factors for arterial thrombotic and thromboembolic events are: smoking; hypertension; hyperlipidemias; obesity; increasing age.
COC users with migraine (particularly migraine with aura) may be at increased risk of stroke (see Contraindications).
Further risk factors, that represent contraindications for the use of COCs are listed in Contraindications.
Ocular lesions: With use of COCs, there have been reports of retinal vascular thrombosis, which may lead to partial or complete loss of vision. If there are signs or symptoms such as visual changes, onset of proptosis or diplopia, papilledema, or retinal vascular lesions, the COC should be discontinued and the cause immediately evaluated.
Blood pressure: Increases in blood pressure have been reported in women taking COCs.
In women with hypertension or a history of hypertension or hypertension-related diseases (including certain renal diseases), another method of birth control may be preferable. If COCs are used in such cases, close monitoring is recommended; if a significant increase in blood pressure occurs, COCs should be discontinued.
Elevated blood pressure associated with COC use will generally return to baseline after stopping COCs, and there appears to be no difference in the occurrence of hypertension among ever-and-never-users.
COC use is contraindicated in women with uncontrolled hypertension (see Contraindications).
Carcinoma of the reproductive organs: Cervical cancer: The most important risk factor for cervical cancer is persistent human papillomavirus infection.
Some studies suggest that COC use may be associated with an increase in the risk of cervical intraepithelial neoplasia or invasive cervical cancer in some populations of women. For example, the results of one meta-analysis of 24 epidemiological studies indicated that among current users of oral contraceptives, the relative risk of invasive cervical cancer increased with increasing duration of use. The relative risk for 5 or more years' use versus never-use was 1.90 (95% confidence interval 1.69-2.13). The relative risk declined after use ceased and by 10 or more years was not significantly different from that in never-users. However, there continues to be controversy about the extent to which such findings may be due to differences in sexual behaviour and other factors. In cases of undiagnosed abnormal genital bleeding, adequate diagnostic measures are indicated.
Breast cancer: Established risk factors for the development of breast cancer include increasing age, family history, obesity, nulliparity, and late age for first full-term pregnancy.
A meta-analysis from 54 epidemiological studies reported that there is slightly increased relative risk (1.24) of having breast cancer diagnosed in women who are using COCs compared to never-users. The increased risk gradually disappears during the course of the 10 years after cessation of COC use. These studies do not provide evidence for causation. The observed pattern of increased risk of breast cancer diagnosis may be due to earlier detection of breast cancer in COC users (due to more regular clinical monitoring), the biological effects of COCs, or a combination of both. Because breast cancer is rare in women under 40 years of age, the excess number of breast cancer diagnoses in current and recent COC users is small in relation to the lifetime risk of breast cancer. Breast cancers diagnosed in ever-users tend to be less advanced clinically than the cancers diagnosed in never-users.
Hepatic neoplasia/liver disease/hepatitis C: In very rare cases hepatic adenomas, and in extremely rare cases, hepatocellular carcinoma may be associated with COC use. The risk appears to increase with duration of COC use. Rupture of hepatic adenomas may cause death through intra-abdominal hemorrhage.
Women with a history of COC-related cholestasis and women who develop cholestasis during pregnancy are more likely to develop cholestasis with COC use. Such patients who use COCs should be carefully monitored and, COC use should be discontinued if cholestasis recurs.
Hepatocellular injury has been reported with COC use. Early identification of drug-related hepatocellular injury can decrease the severity of hepatotoxicity when the drug is discontinued. If hepatocellular injury is diagnosed, patients should stop their COC, use a non-hormonal form of birth control and consult their doctor.
Acute or chronic disturbances of liver function may necessitate the discontinuation of COC use until liver function has returned to normal.
ALT elevations: During clinical trials with patients treated for hepatitis C virus infections (HCV) with the medicinal products containing ombitasvir/paritaprevir/ritonavir and dasabuvir with/without ribavirin, transaminase (ALT) elevations higher than 5 times the upper limit of normal (ULN) occurred significantly more frequent in women using ethinylestradiol-containing medications such as combined hormonal contraceptives (CHCs). Patients who are taking ethinylestradiol-containing medicinal products must switch to an alternative method of contraception (e.g. progestin only contraception or non-hormonal methods) prior to initiating ombitasvir/paritaprevir/ritonavir and dasabuvir therapy (see Contraindications and Interactions).
Migraine/headache: The onset or exacerbation of migraine or development of headache with a new pattern that is recurrent, persistent or severe requires discontinuation of COCs and evaluation of the cause.
Women with migraine (particularly migraine with aura) who take COCs may be at increased risk of stroke. See Contraindications.
Immune: Angioedema: Exogenous estrogens may induce or exacerbate symptoms of angioedema, particularly in women with hereditary angioedema.
Precautions: Medical examinations: Before COC use is initiated, a thorough individual history, family history, and physical examination, including a blood pressure determination, should be performed. An examination of the breasts, liver, extremities, and pelvic organs should also be conducted. A Papanicolaou (Pap) smear should be performed if the patient has been sexually active or if it is otherwise indicated.
Such medical examinations should be repeated at least annually during the use of COCs.
The first follow-up visit should occur 3 months after COCs are prescribed. At each annual visit, examination should include those procedures that were performed at the initial visit, as described previously.
Carbohydrate and lipid effects: Glucose intolerance has been reported in COC users. Women with impaired glucose tolerance or diabetes mellitus who use COCs should be carefully monitored. See Contraindications.
A small proportion of women will have adverse lipid changes while taking OCs. Nonhormonal birth control should be considered in women with uncontrolled dyslipidemias. Persistent hypertriglyceridemia may occur in a small proportion of COC users. Elevations of plasma triglycerides in COC users may lead to pancreatitis and other complications.
Estrogens increase serum high-density lipoproteins (HDL cholesterol), whereas a decline in serum HDL cholesterol has been reported with many progestational agents. Some progestins may elevate low-density lipoprotein (LDL) levels and may render the control of hyperlipidemias more difficult. The net effect of a COC depends on the balance achieved between doses of estrogen and progestin and the nature and absolute amount of progestins used in the contraceptive. The amount of both hormones should be considered in the choice of a COC.
Women who are being treated for hyperlipidemias should be followed closely if they elect to use COCs.
Genital bleeding: In some women withdrawal bleeding may not occur during the tablet free interval. If the COC has not been taken according to directions prior to the first missed withdrawal bleed, or if two consecutive withdrawal bleeds are missed, tablet-taking should be discontinued and a nonhormonal back-up method of birth control should be used until the possibility of pregnancy is excluded.
Breakthrough bleeding/spotting may occur in women taking COCs, especially during the first three months of use. The type and dose of progestin may be important. If this bleeding persists or recurs, nonhormonal causes should be considered and adequate diagnostic measures may be indicated to rule out pregnancy, infection, malignancy, or other conditions. If pathology has been excluded, continued use of the COC or a change to another formulation may solve the problem.
Some women may encounter post-pill amenorrhea (possibly with anovulation) or oligomenorrhea, especially when such a condition was preexistent.
Depression: Women with a history of depression who use COCs should be carefully observed and the drug discontinued if depression recurs to a serious degree. Patients becoming significantly depressed while taking COCs should stop the medication and use an alternative method of birth control in an attempt to determine whether the symptom is drug-related.
Other: Patients should be counseled that this product does not protect against HIV infection (AIDS) or other sexually transmitted diseases.
Diarrhea and/or vomiting may reduce hormone absorption resulting in decreased serum concentrations (see Advice in case of vomiting and/or diarrhea under Dosage & Administration and Interactions).
Effects on ability to drive and use machines: The impact of MINULET on the ability to drive and use machines has not been systematically evaluated. MINULET is not expected to influence the ability to drive or use machines. Cases of dizziness have been reported. Patients should exercise caution until they know that MINULET does not affect these abilities.
Use in Children: Safety and efficacy of COCs have been established in women of reproductive age. Use of these products before menarche is not indicated.
Use in the Elderly: COCs are not indicated for use in postmenopausal women.
Pregnancy: If pregnancy occurs during treatment with COCs, further intake should be discontinued. There is no conclusive evidence that the estrogen and progestin contained in the COC will damage the developing child if conception accidentally occurs during COC use (see Contraindications).
Lactation: Small amounts of contraceptive steroids and/or metabolites have been identified in the milk of nursing mothers and a few adverse effects on the child have been reported, including jaundice and breast enlargement. Lactation may be affected by COCs, as COCs may reduce the quantity and change the composition of breast milk.
The use of COCs is generally not recommended until the nursing mother has completely weaned her child.
Adverse reactions are listed in the Table per CIOMS frequency categories: Very Common: ≥10%; Common: ≥1% and <10%; Uncommon: ≥0.1% and <1%; Rare: ≥0.01% and <0.1%, Very rare: <0.01%.
Use of COCs has been associated with increased risk of the following: Arterial and venous thrombotic and thromboembolic events, including myocardial infarction, stroke, transient ischemic attack, venous thrombosis and pulmonary embolism; Cervical intraepithelial neoplasia and cervical cancer; Breast cancer diagnosis; Benign hepatic tumors (e.g., focal nodular hyperplasia, hepatic adenoma).
See also Special Warnings and Precautions under Precautions. (See Table 3.)
Click on icon to see table/diagram/image
Interactions between ethinyl estradiol (EE) and other substances may lead to decreased or increased serum EE concentrations, respectively.
Concomitant use with the medicinal products containing ombitasvir/paritaprevir/ritonavir and dasabuvir, with or without ribavirin may increase the risk of ALT elevations (see Contraindications and Special Warnings: Hepatic neoplasia/liver disease/hepatitis C under Precautions). Therefore, users must switch to an alternative method of contraception (e.g., progestogen-only contraception or non-hormonal methods) prior to starting therapy with this combination drug regimen. MINULET can be restarted 2 weeks following completion of treatment with this combination drug regimen.
Decreased EE serum concentrations may cause an increased incidence of breakthrough bleeding and menstrual irregularities and may possibly reduce efficacy of the COC.
During concomitant use of EE-containing products and substances that may lead to decreased EE serum concentrations, it is recommended that a nonhormonal back-up method of birth control (such as condoms and spermicide) be used in addition to the regular intake of MINULET.
In the case of prolonged use of such substances COCs should not be considered the primary contraceptive.
After discontinuation of substances that may lead to deceased EE serum concentrations, use of a nonhormonal back-up method is recommended for at least 7 days. Longer use of a back-up method is advisable after discontinuation of substances that have led to induction of hepatic microsomal enzymes, resulting in decreased EE serum concentrations. It may sometimes take several weeks until enzyme induction has completely subsided, depending on dosage, duration of use and rate of elimination of the inducing substance.
Examples of substances that may decrease serum EE concentrations: Any substance that reduces gastrointestinal transit time and, therefore, EE absorption.
Substances that induce hepatic microsomal enzymes, such as rifampicin, rifabutin, barbiturates, primidone, phenylbutazone, phenytoin, dexamethasone, griseofulvin, topiramate, some protease inhibitors, modafinil.
Hypericum perforatum, also known as St. John's wort, and ritonavir* (possibly by induction of hepatic microsomal enzymes).
*Although ritonavir is an inhibitor of cytochrome P450 3A4, treatment with ritonavir has been shown to decrease EE serum concentrations (see previously mentioned).
Examples of substances that may increase serum EE concentrations: Atorvastatin.
Competitive inhibitors for sulfation in the gastrointestinal wall, such as ascorbic acid (vitamin C) and paracetamol (acetaminophen).
Substances that inhibit cytochrome P450 3A4 isoenzymes such as indinavir, fluconazole, and troleandomycin*. Troleandomycin may increase the risk of intrahepatic cholestasis during coadministration with COCs.
EE may interfere with the metabolism of other drugs by inhibiting hepatic microsomal enzymes, or by inducing hepatic drug conjugation, particularly glucuronidation. Accordingly, plasma and tissue concentrations may either be increased (e.g., cyclosporine, theophylline, corticosteroids) or decreased (e.g., lamotrigine).
In patients treated with flunarizine, use of oral contraceptives has been reported to increase the risk of galactorrhea. There have been reports of pregnancy when COCs were co-administered with certain antibiotics (e.g., ampicillin and other penicillins, tetracyclines).
The prescribing information of concomitant medications should be consulted to identify potential interactions.
Laboratory test information: Estrogen-containing preparations can affect many laboratory tests. Some examples are: Increased prothrombin and Factors VII, VIII, IX, and X; decreased antithrombin 3; increased norepinephrine-induced platelet aggregability.
Increased thyroid-binding globulin (TBG) leading to increased circulating total-thyroid hormone, as measured by protein-bound iodine (PBI). T4 by radioimmunoassay. Free T3 resin uptake is decreased, reflecting the elevated TBG; free T4 concentration is unaltered.
Reduced response to metyrapone test.
The results of these tests should not be regarded as reliable until oral contraceptive use has been discontinued for 1-2 months. Abnormal tests should then be repeated.
Oral contraceptives may produce false positive results when neutrophil alkaline phosphatase activity is evaluated for the early diagnosis of pregnancy.
Store below 30°C. Store in a cool, dry place.
G03AA10 - gestodene and ethinylestradiol ; Belongs to the class of progestogens and estrogens in fixed combinations. Used as systemic contraceptives.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image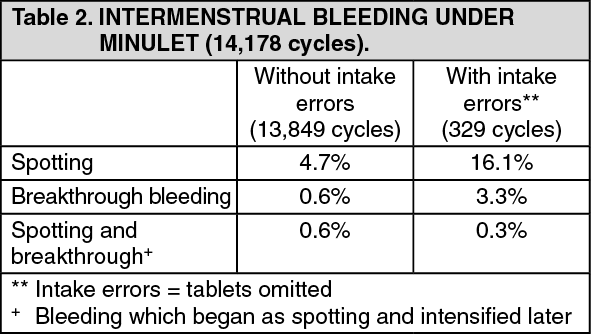 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image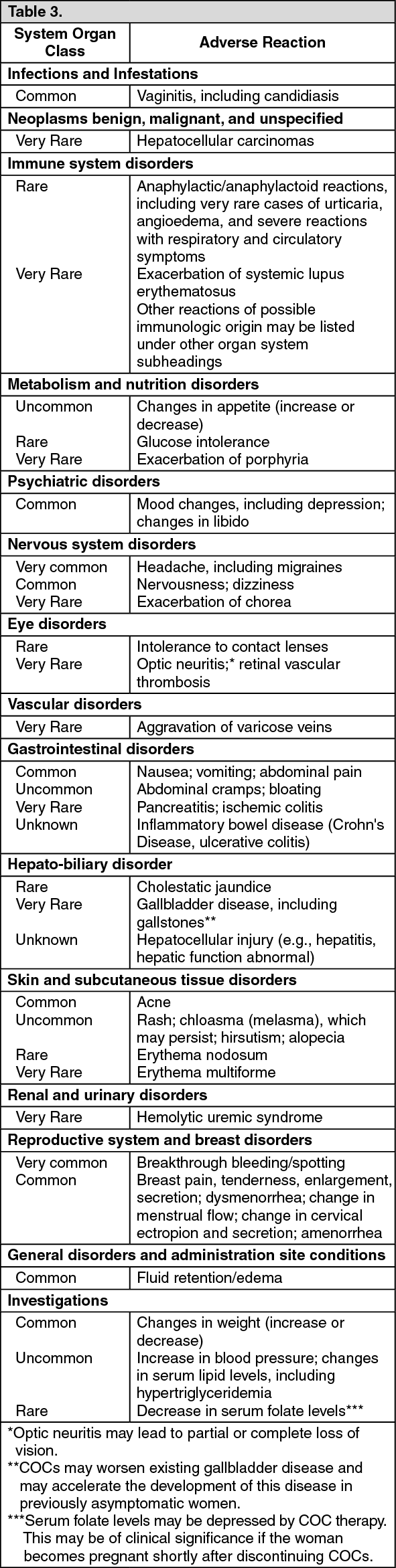 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
