Pharmacotherapeutic group: antibacterials for systemic use, carbapenems.
ATC code: J01DH02.
Pharmacology: Pharmacodynamics: Mode of action: Meropenem exerts its bactericidal activity by inhibiting bacterial cell wall synthesis in Gram-positive and Gram-negative bacteria through binding to multiple penicillin-binding proteins (PBPs).
Pharmacokinetic/Pharmacodynamic (PK/PD) relationship: Similar to other beta-lactam antibacterial agents, the time that meropenem concentrations exceed the MIC (T>MIC) has been shown to best correlate with efficacy. In preclinical models meropenem demonstrated activity when plasma concentrations exceeded the MIC of the infecting organisms for approximately 40% of the dosing interval. This target has not been established clinically.
Pharmacokinetics: A 30 minute intravenous infusion of a single dose of Meronem in healthy volunteers results in peak plasma levels of approximately 11 μg/mL for the 250 mg dose, 23 μg/mL for the 500 mg dose and 49 μg/mL for the 1g dose.
However, there is no absolute pharmacokinetic proportionality with the administered dose both as regards C
max and AUC. Furthermore, a reduction in plasma clearance from 239 to 205 mL/min for the range of dosage 500 mg to 2 g has been observed.
A 5 minute intravenous bolus injection of Meronem IV in healthy volunteers results in peak plasma levels of approximately 52 μg/mL for the 500 mg dose and 112 μg/mL for the 1g dose.
After an IV dose of 500 mg, plasma levels of meropenem decline to values of 1 μg/mL or less, 6 hours after administration.
When multiple doses are administered at 8 hourly intervals to subjects with normal renal function, accumulation of meropenem does not occur.
In subjects with normal renal function, meropenem's elimination half-life is approximately 1 hour.
Plasma protein binding of meropenem is approximately 2%.
Approximately 70% of the administered dose is recovered as unchanged meropenem in the urine over 12 hours, after which little further urinary excretion is detectable. Urinary concentrations of meropenem in excess of 10 μg/mL are maintained for up to 5 hours after the administration of a 500 mg dose. No accumulation of meropenem in plasma or urine was observed with regimens using 500 mg administered every 8 hours or 1g administered every 6 hours in volunteers with normal renal function.
The only metabolite of meropenem is microbiologically inactive.
Meropenem penetrates well into most body fluids and tissues including cerebrospinal fluid of patients with bacterial meningitis, achieving concentrations in excess of those required to inhibit most bacteria.
The pharmacokinetics in infants and children with infection at doses of 10, 20 and 40 mg/kg showed C
max values approximating to those in adults following 500, 1000 and 2000 mg doses, respectively. Comparison showed consistent pharmacokinetics between the doses and half-lives similar to those observed in adults in all but the youngest subjects (<6 months t1/2
1.6 hours). The mean meropenem clearance values were 5.8 mL/min/kg (6-12 years), 6.2 mL/min/kg (2-5 years), 5.3 mL/min/kg (6-23 months) and 4.3 mL/min/kg (2-5 months). Approximately 60% of the dose is excreted in urine over 12 hours as meropenem with a further 12% as metabolite. Meropenem concentrations in the CSF of children with meningitis are approximately 20% of concurrent plasma levels although there is significant inter-individual variability.
The pharmacokinetics of meropenem in neonates requiring anti-infective treatment showed greater clearance in neonates with higher chronological or gestational age with an overall average half-life of 2.9 hours. Monte Carlo simulation based on a population PK model showed that a dose regimen of 20 mg/kg 8 hourly achieved 60 % T>MIC for
P. aeruginosa in 95 % of pre-term and 91 % of full term neonates.
Pharmacokinetic studies in patients with renal insufficiency have shown the plasma clearance of meropenem correlates with creatinine clearance. Dosage adjustments are necessary in subjects with renal impairment.
Pharmacokinetic studies in the elderly have shown a reduction in plasma clearance of meropenem which correlated with age-associated reduction in creatinine clearance.
Pharmacokinetic studies in patients with liver disease have shown no effects of liver disease on the pharmacokinetics of meropenem.
Toxicology: Preclinical Safety Data: Animal studies indicate that meropenem is well tolerated by the kidney. In animal studies meropenem has shown nephrotoxic effects, only at high dose levels (500 mg/kg).
Effects on the CNS; convulsions in rats and vomiting in dogs, were seen only at high doses (>2000 mg/kg).
For an IV dose the LD
50 in rodents is greater than 2000 mg/kg. In repeat dose studies (up to 6 months) only minor effects were seen including a small decrease in red cell parameters and an increase in liver weight in dogs treated with doses of 500 mg/kg.
There was no evidence of mutagenic potential in the 5 tests conducted and no evidence of reproductive and teratogenic toxicity in studies at the highest possible doses in rats and monkeys; the no effect dose level of a (small) reduction in F
1 body weight in rat was 120 mg/kg.
There was no evidence of increased sensitivity to meropenem in juveniles compared to adult animals. The intravenous formulation was well tolerated in animal studies.
The sole metabolite of meropenem had a similar profile of toxicity in animal studies.
Microbiology: Mechanisms of resistance: Bacterial resistance to meropenem may result from one or more factors: decreased permeability of the outer membrane of Gram-negative bacteria (due to diminished production of porins); reduced affinity of the target PBPs; increased expression of efflux pump components, and production of beta-lactamases that can hydrolyse carbapenems.
Localised clusters of infections due to carbapenem-resistant bacteria have been reported in the European Union.
There is no target-based cross-resistance between meropenem and agents of the quinolone, aminoglycoside, macrolide and tetracycline classes. However, bacteria may exhibit resistance to more than one class of antibacterials agents when the mechanism involved include impermeability and/or an efflux pump(s).
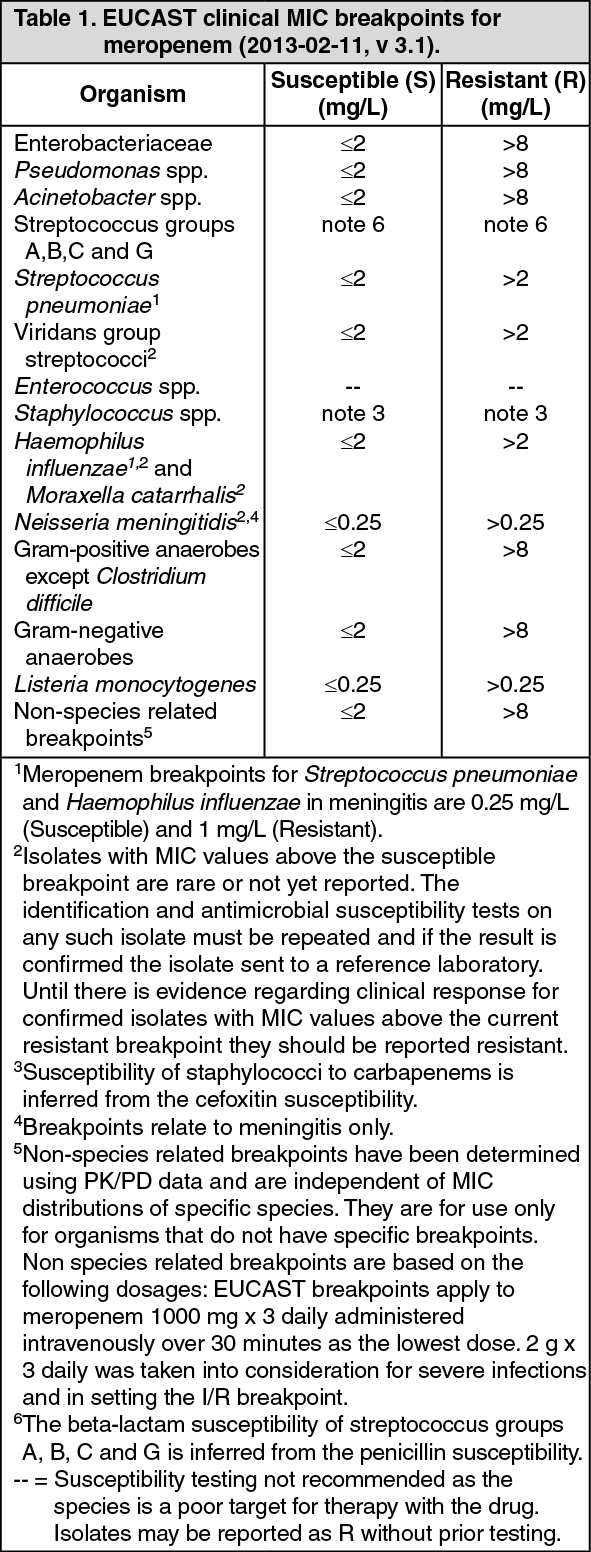
Breakpoints: European Committee on Antimicrobial Susceptibility Testing (EUCAST) clinical breakpoints for MIC testing are presented as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent in at least some types of infections is questionable.
The following table of pathogens listed is derived from clinical experience and therapeutic guidelines. (See Table 2.)
Click on icon to see table/diagram/image


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image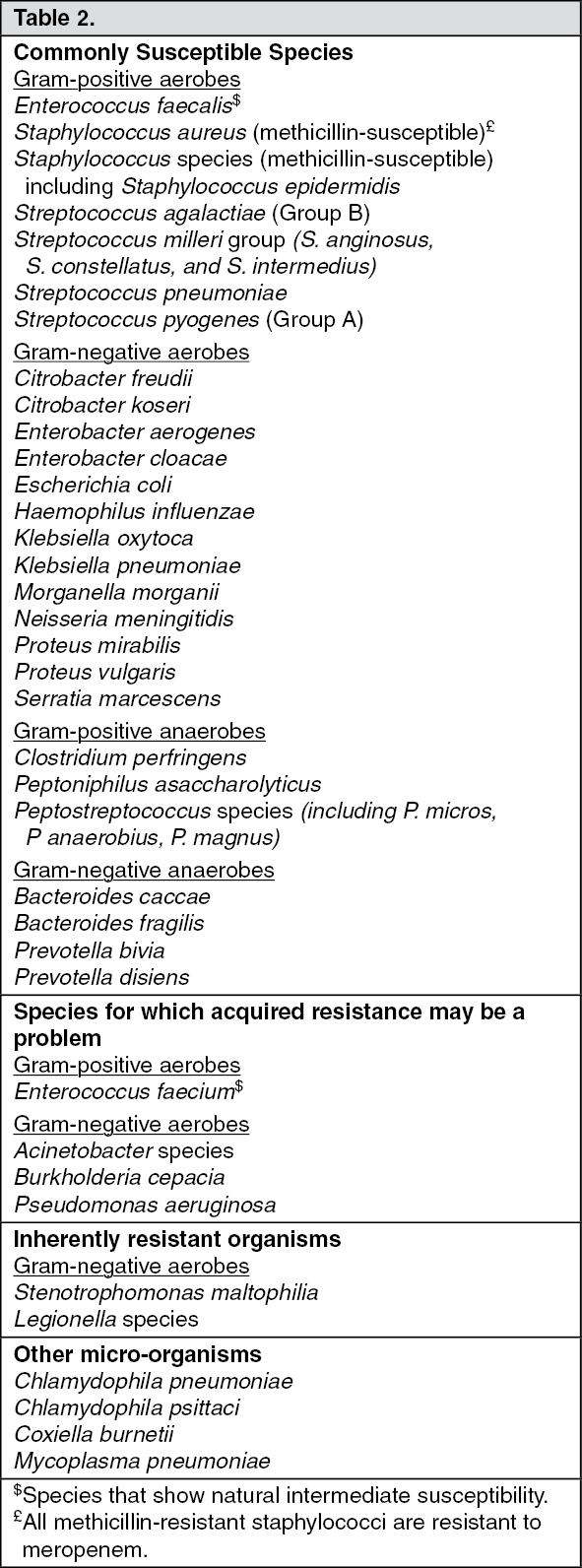 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image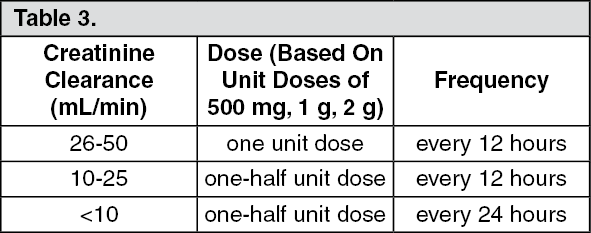 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
