


 Sign Out
Sign Out




The average exposure to edoxaban 60 mg (including 30 mg dose reduced) was 2.5 years among 7,012 patients in ENGAGE AF-TIMI 48 and 251 days among 4,118 patients in Hokusai-VTE.
Adverse reactions were experienced by 2,256 (32.2%) of the patients treated with edoxaban 60 mg (30 mg dose reduced) in the ENGAGE AF-TIMI 48 study and 1,249 (30.3%) in the Hokusai-VTE study.
In both studies, the most common adverse reactions related to bleeding with edoxaban 60 mg based on adjudicated terms included cutaneous soft tissue haemorrhage (up to 5.9%) and epistaxis (up to 4.7%), while vaginal haemorrhage (9.0%) was the most common bleeding-related adverse reaction in Hokusai-VTE only.
Bleeding can occur at any site and may be severe and even fatal (see Precautions).
Common other adverse reactions for edoxaban were anaemia, rash and abnormal liver function tests.
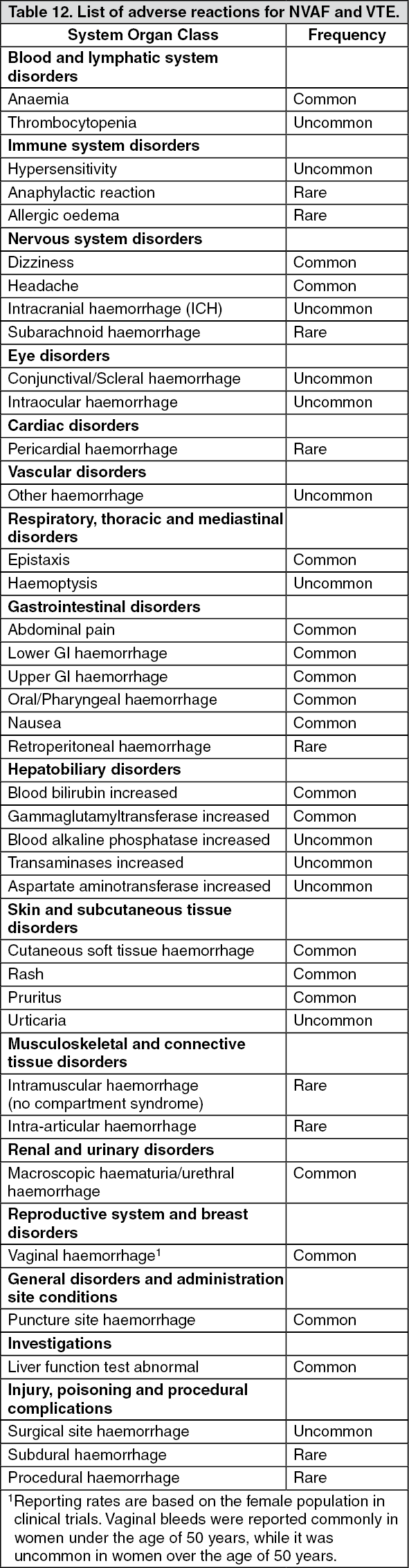
Tabulated list of adverse reactions: Table 12 provides the list of adverse reactions from the two pivotal Phase 3 studies in patients with VTE (DVT and PE) (Hokusai-VTE study) and AF (ENGAGE AF-TIMI 48 study) combined for both indications. The adverse reactions are classified by System Organ Class and frequency, using the following convention: Very common (≥ 1/10), Common (≥ 1/100 to < 1/10), Uncommon (≥ 1/1,000 to < 1/100), Rare (≥ 1/10,000 to < 1/1,000), Very rare (< 1/10,000), not known (cannot be estimated from the available data). (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Due to the pharmacological mode of action, the use of Lixiana may be associated with an increased risk of occult or overt bleeding from any tissue or organ which may result in post haemorrhagic anaemia. The signs, symptoms, and severity (including fatal outcome) will vary according to the location and degree or extent of the bleeding and/or anaemia (see Management of bleeding under Overdosage). In the clinical studies mucosal bleedings (e.g. epistaxis, gastrointestinal, genitourinary) and anaemia were seen more frequently during long term edoxaban treatment compared with VKA treatment. Thus, in addition to adequate clinical surveillance, laboratory testing of haemoglobin/haematocrit could be of value to detect occult bleeding, as judged to be appropriate. The risk of bleedings may be increased in certain patient groups e.g. those patients with uncontrolled severe arterial hypertension and/or on concomitant treatment affecting haemostasis (see Haemorrhagic risk in Precautions). Menstrual bleeding may be intensified and/or prolonged. Haemorrhagic complications may present as weakness, paleness, dizziness, headache or unexplained swelling, dyspnoea, and unexplained shock.
Known complications secondary to severe bleeding such as compartment syndrome and renal failure due to hypoperfusion have been reported for Lixiana. Therefore, the possibility of haemorrhage is to be considered in evaluating the condition in any anticoagulated patient.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system.
View ADR Monitoring Form